Bone Marrow Transplantation (2018) 53:701–707
https://doi.org/10.1038/s41409-018-0177-6
ARTICLE
Lenalidomide vs bortezomib maintenance choice post-autologous
hematopoietic cell transplantation for multiple myeloma
Jennifer Huang1 Sharon Phillips2 Michael Byrne3 Wichai Chinratanalab3 Brian G. Engelhardt3
Stacey A. Goodman3 Shelton L. Harrell3 Madan Jagasia3 Adetola Kassim3 Kyle T. Rawling3 Bipin N. Savani3
Salyka Sengsayadeth3 R. Frank Cornell3
●
●
●
●
●
●
●
●
●
●
●
●
1234567890();,:
1234567890();,:
Received: 3 November 2017 / Revised: 18 February 2018 / Accepted: 23 March 2018 / Published online: 27 April 2018
© Macmillan Publishers Limited, part of Springer Nature 2018
Abstract
Maintenance therapy post-autologous hematopoietic cell transplantation (AHCT) with either lenalidomide or bortezomib for
multiple myeloma (MM) have separately been shown to improve progression-free survival (PFS), but have never been
directly compared. We performed a retrospective study to investigate progression-free and overall survival outcomes and
toxicities of lenalidomide maintenance therapy compared with bortezomib maintenance in MM patients post-AHCT. This
study included 156 patients who received post-AHCT lenalidomide or bortezomib maintenance therapy for MM. The
primary outcome was PFS. Ninety-two patients received lenalidomide maintenance and 64 received bortezomib maintenance
post-AHCT. By multivariable analysis, maintenance therapy choice and cytogenetics risk did not impact PFS or OS. Staging
by International Staging System and pre-maintenance disease response were the greatest predictors for PFS. Treatmentrelated toxicities were as anticipated with 5.4% of patients receiving maintenance lenalidomide experiencing secondary
primary malignancies (SPMs) compared with 3% for bortezomib. These findings suggest there were no differences in PFS or
OS between lenalidomide and bortezomib maintenance therapy options for post-transplantation MM patients. These data
should be validated in a larger, prospective cohort to determine if maintenance choice should be guided by side effect profile
and patient anticipated tolerance rather than by disease biology alone.
Introduction
Multiple myeloma (MM) is a malignant hematological
disorder characterized by monoclonal proliferation of
plasma cells. Autologous hematopoietic stem cell transplantation (AHCT) for MM is commonly used for patients
with newly diagnosed myeloma in eligible patients [1–4].
AHCT and routine use of modern therapies has improved
the 5-year survival rates, from 34.8% (1998–2001) to
* R. Frank Cornell
robert.f.cornell@vanderbilt.edu
1
Department of Medicine, Vanderbilt University Medical Center,
Nashville, TN, USA
2
Division of Biostatistics and Quantitative Sciences, Vanderbilt
University Medical Center, Nashville, TN, USA
3
Division of Hematology/Oncology, Vanderbilt University Medical
Center, Nashville, TN, USA
44.6% (2006–2009) [5–11]. Despite these advances, MM
remains incurable and relapse occurs for most patients [12].
Post-AHCT maintenance therapy is one approach for
sustaining disease control and prolonging progression-free
survival (PFS) [3, 13–16]. Optimal choice for maintenance
therapy has not yet been established, but various agents
have been used, including corticosteroids, thalidomide,
lenalidomide, and bortezomib in various combinations
[15–22]. While they have collectively been shown to
improve PFS, their impact on overall survival (OS) is
unclear, with some studies demonstrating OS benefit and
others not [1, 15, 22–24]. Post-AHCT maintenance guidelines commonly recommend use of lenalidomide for
standard-risk disease and bortezomib for intermediate and
high-risk disease based on cytogenetics [22, 25–27].
Lenalidomide and bortezomib are two maintenance
therapy options with low toxicity profiles that may offer
survival benefit [16, 21]. Limited data are available evaluating the outcomes in patients who receive lenalidomide
compared with bortezomib maintenance therapy. The aim
of this study was to compare the PFS of lenalidomide and
�702
bortezomib as post-AHCT maintenance therapy for newly
diagnosed MM.
Methods
Patients and study design
A retrospective study of 156 patients with newly diagnosed
MM was performed. Evaluable patients received AHCT at
Vanderbilt University Medical Center with melphalan
conditioning for newly diagnosed MM between 2004 and
2016 after induction with lenalidomide-based and/or
bortezomib-based therapy. The primary outcome was PFS.
Secondary outcomes were OS and treatment-related toxicities. Patients who received tandem transplantations
(autologous or allogeneic) and patients with a diagnosis
other than MM were excluded (n = 17). Patients receiving
up to three lines of induction therapy were permitted for
analysis. Maintenance therapy was defined as monotherapy
with either lenalidomide or bortezomib and started
2–4 months post-AHCT. Lenalidomide maintenance was
administered at a starting dose of 10 mg/day and increased
to 15 mg/day as tolerated. Bortezomib maintenance was
administered as 1.3 mg/m2 subcutaneous every 2 weeks.
Choice of maintenance therapy between lenalidomide and
bortezomib was determined by physician and patient preference based on cytogenetics, anticipated tolerance and
drug cost in some cases. Institutionally, patients received
maintenance for a minimum of 2 years if progression did
not occur prior to that time point. Thereafter, patients and
provider discussed the risks and benefits of continuing
maintenance therapy. If the decision was made to stop
maintenance at this time it was considered completion of
maintenance therapy.
J. Huang et al.
progression was defined as time from day 30 after AHCT to
first documentation of progressive disease.
Patient- and disease-related variables and outcomes of
interest were summarized using descriptive statistics. The
primary objective of this study was to evaluate PFS between
patients receiving post-AHCT lenalidomide maintenance
compared with bortezomib maintenance. Other variables
considered included age, gender, myeloma subtype (IgG vs.
IgA vs. light chain only), stage by International Staging
System (ISS) (stage III vs. I/II), cytogenetic abnormality
risk (high/intermediate risk vs. standard risk), disease status
at time of maintenance initiation (stringent complete
remission (sCR)/complete remission (CR)/very good partial
response (VGPR) vs. partial response (PR)/stable disease
(SD)/progressive disease (PD)) and duration of maintenance
therapy (< 2 years vs. ≥ 2 years).
Continuous variables were analyzed using Wilcoxon
rank sum test and categorical variables were compared
using Pearson’s chi-squared test. The Kaplan–Meier
method was used to analyze time to disease progression in
each group with stratified log-rank test. A Cox proportional
hazards regression model was used to estimate the hazard
ratio (HR) and 95% confidence intervals (CIs) for PFS and
OS. Variables considered in the multivariable analysis were
selected a priori and included cytogenetic abnormality risk
(high/intermediate risk vs. standard risk), ISS stage (III vs.
I/II), maintenance therapy option (bortezomib vs. lenalidomide), and treatment response prior to maintenance initiation (PR/SD/PD vs. sCR/CR/VGPR). This study was
underpowered to analyze duration of maintenance therapy.
An α level of 5% was used to determine significance.
Analyses were performed with R version 3.2.3 (2015-1210) [30].
Results
Definitions
High-risk myeloma was defined as chromosomal abnormalities detected by conventional cytogenetics or fluorescence in situ hybridization (FISH) consisting of t(14;16), t
(14;20), and deletion 17p [26]. Intermediate-risk myeloma
was defined as t(4;14), monosomy 13, hypodiploidy and
gain of 1q [28]. Response to therapy and disease progression was defined according to response criteria determined
by the International Myeloma Working Group [29].
Statistical analysis
PFS was defined as survival without myeloma progression
or relapse from disease response. OS was defined as death
by any cause. Patients alive and without progression or
relapse were censored at last follow-up. Time to relapse or
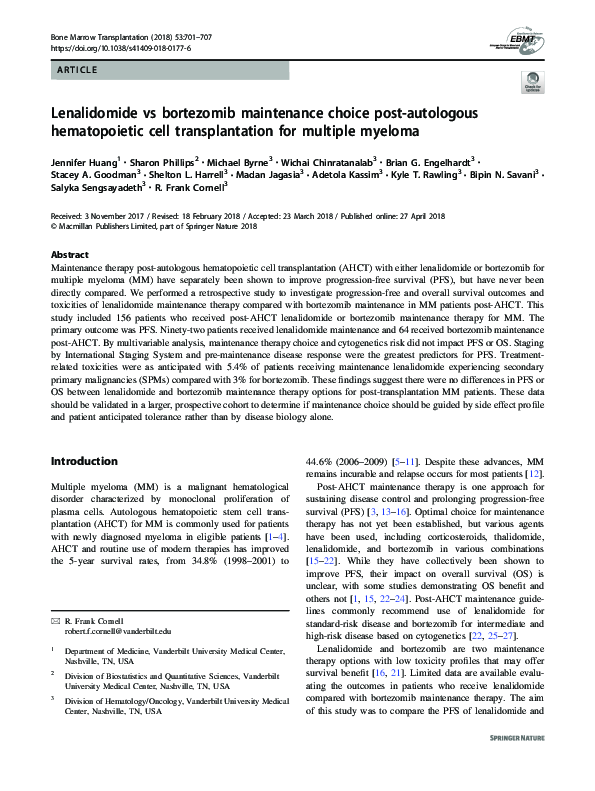
A total of 156 patients were included in the study, 92
patients received lenalidomide, whereas 64 received bortezomib maintenance post-AHCT. The median follow-up
time post-AHCT for survivors was 33.7 months (range
8–119.2 months). At baseline, there were no differences in
ISS stage, Durie–Salmon (DS) stage, or cytogenetic risk
between maintenance cohorts (Table 1). Both cohorts
received a median of one line of induction therapy (range
1–3). At the time of analysis, 47% (n = 43) of patients
receiving lenalidomide maintenance and 52% (n = 33) on
bortezomib maintenance experienced disease progression
(Fig. 1). Of these patients, 29 (67%) experienced disease
progression while on lenalidomide maintenance and 14
(42%) progressed while on bortezomib maintenance
(Table 2).
�Lenalidomide vs bortezomib maintenance choice post-autologous hematopoietic cell transplantation for. . .
Table 1 Baseline characteristics of patients receiving lenalidomide or
bortezomib maintenance therapy post-AHCT
Variable
Lenalidomide
(n = 92)
Bortezomib
(n = 64)
p-Value
Median age, years
(range)
63.0 (57.0–68.0)
60.5
(54.0–66.0)
0.08
Male gender
52 (57)
36 (56)
0.97
White/Caucasian
73 (79)
52 (81)
Black/African
American
18 (20)
12 (19)
Hispanic
1 (1)
0 (0)
IgG subtype
55 (59)
33 (52)
IgA subtype
21 (23)
10 (16)
Light chain only
10 (11)
15 (23)
Race
156 MM patients
on post-AHCT
maintenance
92 lenalidomide
maintenance
64 bortezomib
maintenance
0.70
43 progressed
MM type
Other
703
0.14
6 (7)
6 (9)
Durie–Salmon,
stage 3
45 (50)
31 (48)
ISS, stage 3
18 (21)
18 (29)
Disease risk
0.85
0.61
0.26
Standard risk
60 (65)
38 (59)
Intermediate/high
riska
32 (35)
26 (41)
0.11
Post-AHCT disease
response
sCR
35 (38)
17 (27)
CR
7 (8)
8 (12)
VGPR
43 (47)
29 (45)
PR
5 (5)
10 (16)
SD
2 (2)
0 (0)
Data presented are n (%) unless otherwise indicated
MM multiple myeloma, IgG immunoglobulin, ISS International
Staging System, AHCT autologous hematopoietic cell transplantation,
sCR stringent complete remission, CR complete remission, VGPR very
good partial response, PR partial response, SD stable disease
a
Data were obtained using conventional cytogenetics and fluorescence
in situ hybridization (FISH). High risk was defined as myeloma with
chromosomal abnormalities detected by conventional cytogenetics or
FISH consisting of t(14;16), t(14;20), and deletion 17p [21].
Intermediate risk was defined as t(4;14), monosomy 13, hypodiploidy
and gain of 1q
Sixty-three patients (68.5%) stopped maintenance therapy in the lenalidomide cohort and 41 patients (64.1%)
stopped maintenance in the bortezomib cohort. The reasons
for stopping maintenance therapy included disease progression (lenalidomide: n = 22, 34.9%, bortezomib: n = 12,
29.2%), completed therapy and changed to observation
alone (lenalidomide: n = 27, 42.8%, bortezomib: n = 16,
39.0%), maintenance intolerance (lenalidomide: n = 11,
17.5%, bortezomib: n = 8, 19.5%), switch to different
maintenance therapy option (lenalidomide: n = 2, 3.2%,
bortezomib: n = 1, 2.4%), and other logistical/financial
49 no progression
33 progressed
31 no progression
Fig. 1 CONSORT flow diagram
reasons (lenalidomide: n = 1, 1.6%, bortezomib: n = 4,
9.8%). Fourteen percent (n = 9) of patients receiving bortezomib maintenance and 24% (n = 22) of those receiving
lenalidomide maintenance required dose reductions.
Patients who completed therapy and changed to observation
alone completed a minimum of 2 years of therapy regardless of depth of response. Among these patients, there was
no difference in maintenance duration between cohorts with
a median lenalidomide duration of 25.4 months (range
12.6–44.7 months) and 22.9 months with bortezomib (range
11.1–29.5 months; p = 0.09). For patients who ended
maintenance therapy for other reasons, patients remained on
lenalidomide maintenance for a longer duration (median
24.8 months, range 6.0–54.3 months) than on bortezomib
maintenance (median 17.7 months, range 7.7–42.8 months;
p = 0.01), with the difference predominately due to earlier
cessation of bortezomib from intolerance.
Median time to progression was 27.5 months (range
9.8–58.1 months) in the lenalidomide cohort and
24.3 months (range 9.8–66.6 months) in the bortezomib
cohort (p = 0.52) (Table 2). Patients with standard-risk
myeloma had a median time to progression of 26.9 months
(range 10.8–54.3 months) with lenalidomide and
25.7 months (range 10.9–66.6 months) with bortezomib
(p = 0.80). For intermediate- and high-risk disease, median
time to progression was 27.5 months (range
9.8–58.1 months) with lenalidomide and 24.1 months
(range 9.8–48.0 months) with bortezomib (p = 0.47)
(Table 3).
Disease response improved while on maintenance in
34% (n = 32) with lenalidomide and 38% (n = 23) with
bortezomib (Table 2). Median time to best response after
maintenance initiation was 11.3 months (range
5.7–34.8 months) for the lenalidomide cohort and
9.7 months (range 6.4–19.0 months) for the bortezomib
cohort (p = 0.79) (Table 2).
Mortality occurred in 19 patients (21%) in the lenalidomide cohort and 6 patients (9%) in the bortezomib cohort
�704
J. Huang et al.
Table 2 Patient outcomes from time of maintenance initiation
Variable
Lenalidomide (n = 92)
Improved response on maintenance
CR → sCR
Bortezomib (n = 64)
p-Value
32 (34)
23 (38)
0.40
4 (13)
5 (22)
VGPR → sCR
19 (59)
10 (43)
PR → sCR
1 (3)
0 (0)
VGPR → CR
5 (16)
2 (9)
PR → VGPR
2 (6)
6 (26)
PD → VGPR
1 (3)
0 (0)
43 (47)
33 (52)
Disease progression while on maintenance
29 (32)
14 (22)
Disease progression on surveillance alone
14 (15)
20 (31)
Overall disease progression
0.55
Disease progression < 2 years post-AHCT
23 (25)
15 (23)
0.82
Median time to best response after maintenance
initiation, months (range)
11.3 (5.7–34.8)
9.7 (6.4–19.0)
0.79
Median time to death, months (range)
62.7 (31.8–91.0)
69.2 (34.4–119.2)
0.47
Median time to progression, months (range)
27.5 (9.8–58.1)
24.3 (9.8–66.6)
0.52
Deceased
19 (21)
6 (9)
0.06
Data presented are n (%) unless otherwise indicated
CR complete remission, sCR stringent complete remission, VGPR very good partial response, PR partial response, PD progressive disease, AHCT
autologous hematopoietic cell transplantation
Table 3 Median time to progression by cytogenetic risk
FISH risk
Lenalidomide
Bortezomib
p-Value
Standard, months
26.9 (10.8–54.3)
(n = 24)
25.7 (10.9–66.6)
(n = 18)
0.80
Intermediate/
high, months
27.5 (9.8–58.1)
(n = 13)
24.1 (9.8–48.0)
(n = 15)
0.47
FISH fluorescence in situ hybridization
(p = 0.06) (Table 2). Median time to death from any cause
was 62.7 months (range 31.8–91.0 months) for the lenalidomide maintenance group and 69.2 months (range
34.4–119.2 months) for the bortezomib maintenance group
(p = 0.47) (Table 2).
By multivariable analysis, there was no difference in PFS
or OS based on choice of maintenance therapy (Table 4).
Patients with ISS stage III had significantly reduced PFS
and OS compared with those with ISS stage I/II (HR 2.22;
95% CI 1.28–3.84; p < 0.01) and (HR 4.59; 95% CI
1.75–12.06; p < 0.01), respectively. Patients without deep
disease response prior to maintenance initiation (PR/SD/
PD) were more likely to experience disease progression
compared with those with deeper response (sCR/CR/
VGPR) (HR 2.19; 95% CI 1.19–4.00; p = 0.01). Cytogenetic risk did not impact PFS or OS between cohorts.
Toxicities attributable to maintenance therapy are listed
in Table 5. Nine patients in the lenalidomide group (9.8%)
and 8 patients in the bortezomib group (12.5%) had adverse
events severe enough to necessitate early discontinuation of
maintenance therapy. New or worsening peripheral
neuropathy was the most common toxicity for the bortezomib cohort (10.9%; n = 7). Cytopenias were the most
common adverse events in the lenalidomide cohort (30%; n
= 28). Five patients (5.4%) receiving lenalidomide maintenance experienced secondary primary malignancies
(SPMs), including anaplastic astrocytoma, intracranial
meningioma, endometrial carcinoma, breast adenocarcinoma and one case of Philadelphia chromosome-negative
B-cell acute lymphoblastic leukemia (ALL). Two patients
(3%) receiving bortezomib maintenance developed prostate
adenocarcinoma. No hematological malignancies occurred
in the bortezomib cohort (Table 5). The median time from
initiation of maintenance therapy to development of SPM in
the lenalidomide cohort was 29.2 months (range
5.0–67.4 months) compared with 30.6 months (range
25.5–35.7 months) in the bortezomib cohort. The incidence
rate of SPM for patients on maintenance therapy was 3.2
new cancers per 100 person-years of observation (95% CI
1.6–11.7) in the lenalidomide cohort compared with 2.8
new cancers per 100 person-years of observation (95% CI
0.2–7.2) in the bortezomib cohort.
Discussion
We conducted a single center retrospective study of 156
MM patients who received maintenance lenalidomide or
bortezomib post-AHCT. By multivariable analysis, choice
of maintenance therapy between bortezomib or
�Lenalidomide vs bortezomib maintenance choice post-autologous hematopoietic cell transplantation for. . .
705
Table 4 Multivariable analysis of post-AHCT outcomes in patients with MM receiving maintenance therapy
Effect
Progressive disease
Maintenance therapy bortezomib vs
lenalidomide
Overall mortality
HR (95% CI)
p-Value
HR (95% CI)
p-Value
1.20 (0.72–2.01)
0.48
0.54 (0.18–1.57)
0.26
ISS stage Stage III vs I/II
2.22 (1.28–3.84)
<0.01
4.59 (1.75–12.06)
<0.01
Response to prior therapy PR/SD/PD vs sCR/
CR/VGPR
2.19 (1.19–4.00)
0.01
0.59 (0.12–2.87)
0.51
Cytogenetic riska High/intermediate vs.
standard
1.00 (0.6–1.68)
0.85
1.35 (0.6–3.59)
0.82
AHCT autologous hematopoietic cell transplantation, ISS International Staging System
a
Data were obtained using conventional cytogenetics and fluorescence in situ hybridization. High risk was defined as myeloma with chromosomal
abnormalities detected by conventional cytogenetics or fluorescence in situ hybridization (FISH) consisting of t(14;16), t(14;20), and deletion 17p
[26]. Intermediate risk was defined as t(4;14), monosomy 13, hypodiploidy and gain of 1q
Table 5 Toxicities attributable to maintenance
Lenalidomide (n = 92)
Bortezomib (n = 64)
Adverse event
Grade 1/2
Grade 3/4
Grade 1/2
Grade 3/4
Peripheral
neuropathy
6 (6.5)
2 (0.2)
5 (7.8)
2 (3.1)
Cytopenia
28 (30.4)
0 (0)
2 (3.1)
0 (0)
Secondary
malignancy
0 (0)
5 (5.4)
0 (0)
2 (3.1)
Rash
10 (10.9)
0 (0)
1 (1.6)
0 (0)
Fatigue
16 (17.4)
0 (0)
2 (3.1)
0 (0)
Diarrhea
6 (6.5)
0 (0)
2 (3.1)
0 (0)
Other toxicitya
6 (6.5)
0 (0)
1 (1.6)
0 (0)
Data presented are n (%) unless otherwise indicated
a
Other toxicities included bortezomib: myalgia; lenalidomide: lower
extremity edema, fever, cramping, and dizziness, loss of appetite, and
dry skin with lenalidomide
lenalidomide did not impact the PFS or OS in this population. Comparatively, pre-maintenance disease response
and ISS stage had greatest impact on PFS. Many studies
have demonstrated an improvement in PFS with use of
maintenance therapy with some studies indicating an
improvement in OS compared with placebo [15, 16, 21, 22].
To our knowledge, there are no published reports directly
comparing lenalidomide and bortezomib maintenance. In
addition, in our study, no differences in outcomes were
detected based on cytogenetic profile. This may be because
despite high-risk cytogenetics, choice of maintenance therapy was often driven by physician and patient preference,
based on other factors, including anticipated tolerance,
secondary malignancy risk, and drug cost in some cases.
The relatively short follow-up time of 33.7 months for the
study may further explain the reason that no difference in
PFS was observed based on cytogenetics. With longer follow-up, a difference may have been seen between the two
groups that is not yet identifiable. Standard of care
guidelines for MM commonly recommend the use of postAHCT lenalidomide maintenance for standard-risk patients
and bortezomib maintenance for intermediate and high-risk
patients [25–27]. These data underscore the need for a larger, prospective study in order to validate these findings and
determine if maintenance choice should be guided by side
effect profile and patient anticipated tolerance rather than by
disease biology alone.
The median PFS for patients receiving lenalidomide
maintenance was 27.5 and 24.3 months with bortezomib
maintenance. The Intergroupe Francophone du Myelome
(IFM) [15] and Cancer and Leukemia Group B (CALGB)
[16] trials report median PFS of 41 and 46 months with
lenalidomide maintenance, respectively. HOVON-65/
GMMG-HD4 trial [21] found high-risk patients with creatinine > 2 mg/dL experienced a median PFS of 30 months
with bortezomib. This discrepancy in PFS between our
analysis and these clinical trials is possibly explained by
clinical trial patient selection and pre-maintenance therapeutic choice. Patients in our analysis were permitted to
receive up to three lines of induction therapy and prior
progression with induction was permitted. These patients
would have been excluded from the clinical trials listed
above. In addition, in our study all patients received
induction therapy with either lenalidomide or bortezomib,
whereas many patients in the aforementioned studies
received thalidomide induction therapy. The precise impact
of this is unclear but may have impacted differences
observed in PFS and highlights the point that different
populations are being evaluated. Overall, this study represents a more “real-world” population compared with a
clinical trial population in which patients would have been
excluded per eligibility criteria.
There was no difference in median time to progression
for patients with intermediate- or high-risk myeloma by
cytogenetics receiving lenalidomide compared with those
receiving bortezomib. Sonneveld et al. [21] evaluated use of
�706
thalidomide and bortezomib maintenance and demonstrated
a significant improvement in PFS and OS for high-risk
myeloma with bortezomib-based therapy. One reason for
this difference may be that in the HOVON-65/GMMG-HD4
trial, patients were randomized into two cohorts. Cohort A
received induction therapy with vincristine, doxorubicin,
and dexamethasone followed by AHCT and then postAHCT thalidomide maintenance. Cohort B received bortezomib, doxorubicin, and dexamethasone followed by
AHCT and then bortezomib maintenance. Thus, the
observed improvement in outcomes may stem from the
effect of differential induction therapy rather than that of
maintenance choice alone. In addition, lenalidomide was
not used in this study.
SPM occurred in 5.4% with lenalidomide and 3% with
bortezomib. These are consistent with other published
reports, which indicate a SPM incidence of about 7–8%
with lenalidomide maintenance [15, 16, 31]. In these
reports, patients had a higher propensity for myeloid
malignancies. Interestingly, no patients in our study developed a myeloid malignancy, although one patient receiving
lenalidomide
maintenance
developed
Philadelphia
chromosome-negative B-cell ALL. There are many potential factors that may impact the risk of SPM, including
effects from previous cancer treatment, host factors, and
genetic predisposition [32, 33]. An individual risk–benefit
analysis for continued therapy should be conducted for each
myeloma patient [34–36], and physicians and patients
should make an informed decision together.
Other possible considerations for choice of maintenance
therapy that may affect physician and/or patient preference
include ease of administration and cost efficacy. Lenalidomide has the advantage of daily oral administration but
comes at higher expense. There are limited data evaluating
the impact of maintenance therapy on quality of life.
However, Teitelbaum et al. [37] demonstrated similar rates
of ambulatory visits for myeloma patients treated with
lenalidomide or thalidomide compared with those treated
with bortezomib or other therapies. Regarding expense, a
study in the Canadian healthcare system found the total
annual per patient cost for lenalidomide maintenance therapy was $131,765 compared with $33,967 for bortezomib
maintenance, with the differences between the two maintenance therapies mainly due to acquisition costs of the
drugs rather than management of adverse effects and SPM
[38]. Studies evaluating maintenance choice quality of life
and pharmacoeconomics may provide guidance on other
reasons for choosing one maintenance therapy over another.
Limitations of this research include being a single institutional study and retrospective analysis with relatively
small sample size. The median follow-up time of
33.7 months is also relatively short. Mian et al. [39]
demonstrated improved PFS and OS for patients on
J. Huang et al.
lenalidomide maintenance for > 2 years vs. those on maintenance for ≤ 2 years. After adjusting for patients with disease progression prior to 2 years from the analysis, our
study was underpowered to analyze duration of maintenance therapy. The 2-year time point was selected based
on our institutional practice for minimum planned maintenance duration. In addition, although all patients received
induction therapy with either bortezomib and/or
lenalidomide-based therapies, there was variability in the
frequency and dosing of these agents during induction.
Conclusion
Our study further supports the use of lenalidomide and
bortezomib as maintenance therapy options for MM patients
post-transplantation to improve PFS. Choice of maintenance therapy does not significantly impact PFS or OS
after controlling for other disease-modifying factors,
including ISS stage and disease response to induction
therapy. These findings should be validated to determine if
maintenance therapy choice should be guided by side effect
profile and patient-specific anticipated tolerance rather than
disease biology alone. Further, the decision to remain on
maintenance therapy should be discussed with patients
while considering the risks and benefits of continued
maintenance therapy.
Compliance with ethical standards
Conflict of interest The authors declare that they have no conflict of
interest.
References
1. Palumbo A, Cavallo F, Gay F, Di Raimondo F, Ben Yehuda D,
Petrucci MT, et al. Autologous transplantation and maintenance
therapy in multiple myeloma. N Engl J Med. 2014;371:895–905.
2. Child JA, Morgan GJ, Davies FE, Owen RG, Bell SE, Hawkins K,
et al. High-dose chemotherapy with hematopoietic stem-cell rescue for multiple myeloma. N Engl J Med. 2003;348:1875–83.
3. Attal M, Lauwers-Cances V, Hulin C, Leleu X, Caillot D,
Escoffre M, et al. Lenalidomide, bortezomib, and dexamethasone
with transplantation for myeloma. N Engl J Med.
2017;376:1311–20.
4. Jacobs RW, Saliba RM, Sasaki K, Farhan S, Armas A, Shah ND,
et al. Outcome of patients with nonsecretory multiple myeloma
after autologous hematopoietic stem cell transplantation. Clin
Lymphoma Myeloma Leuk. 2016;16:36–42.
5. Djulbegovic B, Kumar A. Multiple myeloma: detecting the effects
of new treatments. Lancet. 2008;371:1642–4.
6. Pulte D, Redaniel MT, Brenner H, Jansen L, Jeffreys M. Recent
improvement in survival of patients with multiple myeloma:
variation by ethnicity. Leuk Lymphoma. 2014;55:1083–9.
7. Sonneveld P, Goldschmidt H, Rosiñol L, Bladé J, Lahuerta JJ,
Cavo M, et al. Bortezomib-based versus nonbortezomib-based
induction treatment before autologous stem-cell transplantation in
�Lenalidomide vs bortezomib maintenance choice post-autologous hematopoietic cell transplantation for. . .
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
patients with previously untreated multiple myeloma: a metaanalysis of phase III randomized, controlled trials. J Clin Oncol.
2013;31:3279–87.
Kumar SK, Lacy MQ, Dispenzieri A, Buadi FK, Hayman SR,
Dingli D, et al. Early versus delayed autologous transplantation
after immunomodulatory agents-based induction therapy in
patients with newly diagnosed multiple myeloma. Cancer.
2012;118:1585–92.
Gay F, Larocca A, Wijermans P, Cavallo F, Rossi D, Schaafsma
R, et al. Complete response correlates with long-term progressionfree and overall survival in elderly myeloma treated with novel
agents: analysis of 1175 patients. Blood. 2011;117:3025–31.
Cornell RF, Kassim AA. Evolving paradigms in the treatment of
relapsed/refractory multiple myeloma: increased options and
increased complexity. Bone Marrow Transplant. 2016;51:479–91.
Clark CA, Cornell RF, Scott EC, Chung J, Costa LJ. Management
of relapsed and refractory multiple myeloma in modern times:
incorporating new agents into decision-making. Am J Hematol.
2016;91:1044–51.
Barlogie B, Tricot GJ, Van Rhee F, Angtuaco E, Walker R,
Epstein J, et al. Long-term outcome results of the first tandem
autotransplant trial for multiple myeloma. Br J Haematol.
2006;135:158–64.
Palumbo A, Mina R, Cerrato C, Cavallo F. Role of consolidation/
maintenance therapy in multiple myeloma. Clin Lymphoma
Myeloma Leuk. 2013;13:S349–S54.
Facon T. Posttransplantation maintenance in patients with multiple myeloma. Clin Lymphoma Myeloma. 2009;9:S55–S6.
Attal M, Lauwers-Cances V, Marit G, Caillot D, Moreau P, Facon
T, et al. Lenalidomide maintenance after stem-cell transplantation
for multiple myeloma. N Engl J Med. 2012;366:
1782–91.
McCarthy PL, Owzar K, Hofmeister CC, Hurd DD, Hassoun H,
Richardson PG, et al. Lenalidomide after stem-cell transplantation
for multiple myeloma. N Engl J Med. 2012;366:1770–81.
Kagoya Y, Nannya Y, Kurokawa M. Thalidomide maintenance
therapy for patients with multiple myeloma: meta-analysis. Leuk
Res.2012;36:1016-21.
Attal M, Harousseau J-L, Leyvraz S, Doyen C, Hulin C, Benboubker L, et al. Maintenance therapy with thalidomide improves
survival in patients with multiple myeloma. Blood.
2006;108:3289–94.
Berenson JR, Crowley JJ, Grogan TM, Zangmeister J, Briggs AD,
Mills GM, et al. Maintenance therapy with alternate-day prednisone improves survival in multiple myeloma patients. Blood.
2002;99:3163–68.
Sahebi F, Spielberger R, Kogut NM, Fung H, Falk PM, Parker P,
et al. Maintenance thalidomide following single cycle autologous
peripheral blood stem cell transplant in patients with multiple
myeloma. Bone Marrow Transplant. 2006;37:825–9.
Sonneveld P, Schmidt-Wolf IG, van der Holt B, El Jarari L,
Bertsch U, Salwender H, et al. Bortezomib induction and maintenance treatment in patients with newly diagnosed multiple
myeloma: results of the randomized phase III HOVON-65/
GMMG-HD4 trial. J Clin Oncol. 2012;30:2946–55.
Palumbo A, Hajek R, Delforge M, Kropff M, Petrucci MT, Catalano J, et al. Continuous lenalidomide treatment for newly
diagnosed multiple myeloma. N Engl J Med. 2012;366:1759–69.
Lipe B, Vukas R, Mikhael J. The role of maintenance therapy in
multiple myeloma. Blood Cancer J. 2016;6:e485.
707
24. Cornell RF, D’Souza A, Kassim AA, Costa LJ, Innis-Shelton RD,
Zhang MJ, et al. Maintenance versus induction therapy choice on
outcomes after autologous transplantation for multiple myeloma.
Biol Blood Marrow Transplant. 2017;23:269–77.
25. Facon T. Maintenance therapy for multiple myeloma in the era of
novel agents. Hematol Am Soc Hematol Educ Program.
2015;2015:279–85.
26. Mikhael JR, Dingli D, Roy V, Reeder CB, Buadi FK, Hayman
SR, et al. Management of newly diagnosed symptomatic multiple
myeloma: updated Mayo Stratification of Myeloma and RiskAdapted Therapy (mSMART) consensus guidelines 2013. Mayo
Clin Proc. 2013;88:360–76.
27. Anderson KC, Alsina M, Atanackovic D, Biermann JS, Chandler
JC, Costello C, et al. Multiple myeloma, version 2.2016: clinical
practice guidelines in oncology. J Natl Compr Canc Netw.
2015;13:1398–435.
28. Rajkumar SV. Multiple myeloma: 2012 update on diagnosis, riskstratification, and management. Am J Hematol. 2012;87:78–88.
29. Kumar S, Paiva B, Anderson KC, Durie B, Landgren O, Moreau
P, et al. International Myeloma Working Group consensus criteria
for response and minimal residual disease assessment in multiple
myeloma. Lancet Oncol. 2016;17:e328–46.
30. Core Team R. R: a language and environment for statistical
computing. Vienna, Austria: R Core Team; 2015. Version 3.2.3.
31. Musto P, Anderson KC, Attal M, Richardson PG, Badros A, Hou
J, et al. Second primary malignancies in multiple myeloma: an
overview and IMWG consensus. Ann Oncol. 2017;28:228–45.
32. Areethamsirikul N, Reece DE. The risk of secondary primary
malignancies after therapy for multiple myeloma. Leuk Lymphoma. 2015;56:3012–21.
33. Schecter JM, Lentzsch S. Risk of secondary primary malignancies
in maintenance therapy for multiple myeloma. Int J Hematol
Oncol. 2013;2:339–47.
34. Jones JR, Cairns DA, Gregory WM, Collett C, Pawlyn C, Sigsworth R, et al. Second malignancies in the context of lenalidomide
treatment: an analysis of 2732 myeloma patients enrolled to the
Myeloma XI trial. Blood Cancer J. 2016;6:e506.
35. Moreau P, Pylypenko H, Grosicki S, Karamanesht I, Leleu X,
Grishunina M, et al. Subcutaneous versus intravenous administration of bortezomib in patients with relapsed multiple myeloma:
a randomised, phase 3, non-inferiority study. Lancet Oncol.
2011;12:431–40.
36. Ludwig H, Durie BGM, McCarthy P, Palumbo A, San Miguel J,
Barlogie B, et al. IMWG consensus on maintenance therapy in
multiple myeloma. Blood. 2012;119:3003–15.
37. Teitelbaum A, Ba-Mancini A, Huang H, Henk HJ. Health care
costs and resource utilization, including patient burden, associated
with novel-agent-based treatment versus other therapies for multiple myeloma: findings using real-world claims data. Oncologist.
2013;18:37–45.
38. LeBlanc R, Hollmann S, Tay J. Canadian cost analysis comparing
maintenance therapy with bortezomib versus lenalidomide for
patients with multiple myeloma post autologous stem cell transplant. J Popul Ther Clin Pharmacol. 2016;23:e103–13.
39. Mian I, Milton DR, Shah N, Nieto Y, Popat UR, Kebriaei P, et al.
Prolonged survival with a longer duration of maintenance lenalidomide after autologous hematopoietic stem cell transplantation
for multiple myeloma. Cancer. 2016;122:3831–37.
�
 Sharon Phillips
Sharon Phillips