YAEL SHOVAL-ZUCKERMAN ET AL.
The Effectiveness of Early Group Intervention
for Military Reserves Soldiers: The Role of the
Repressive Coping Style
Yael Shoval-Zuckerman, MSW,1, 2 Rachel Dekel, PhD,2 Zahava Solomon, PhD,3 and Ofir Levi, PhD 1, 3, 4
Combat Stress Reaction Unit, Mental Health Division, Medical Corps, IDF, Ramat Gan, Israel
School of Social Work, Bar-Ilan University, Ramat Gan, Israel
3
School of Social Work, Tel Aviv University, Ramat Aviv, Israel
4
School of Social Work, Ruppin Academic Center Emek Hefer, Israel
1
2
ABSTRACT
This study had two aims: 1. To examine whether soldiers
who participated in Early Group Intervention (EGI) would
show less distress and better functioning and physical
health than soldiers who did not participate in EGI, and
2. To examine the contribution of the intervention to
participants with repressive coping style. The sample
comprised 166 male reserve soldiers who fought in the
Second Lebanon War. The intervention was conducted
three months after the traumatic event, was based on
military protocol, and took place over the course of
one day. Data were collected at two points in time (four
months apart). The findings indicated that after EGI,
the intervention group experienced less post-traumatic
distress than did the control group. In addition, four
months after the intervention, the functioning and physical
health of the intervention group was significantly better
than that of the control group. Notably, the intensity of
post-traumatic distress before the intervention was
lower among repressors and low-anxious soldiers than
among soldiers in the other two groups (high-anxious
and defensive). No significant differences were found
after the intervention with regard to the various styles
of coping with post-traumatic distress. Future clinical
implications of the findings are discussed.
INTRODUCTION
The most widespread chronic psychiatric illness following soldiers’ participation in war is Post-traumatic Stress
Disorder (PTSD). It has been found that, cross-culturally,
13%-20% of soldiers who have fought in wars will develop
PTSD during their lifetime (1, 2). PTSD is classified as an
anxiety disorder and is typically defined by the coexistence
of three clusters of symptoms: namely re-experiencing
(intrusive thoughts and images), avoidance and hyperarousal symptoms. PTSD is frequently accompanied by
functional difficulties in various domains such as work/
school, intimate relationships, and sexual functioning
(3). In addition, veteran soldiers with PTSD have many
physical health complaints, make intensive use of health
services, and have a high rate of morbidity in comparison
to veterans without PTSD (4-7).
In recent years, concerted efforts have been invested
in developing psychological interventions to minimize
both the risks of long-term psychological morbidity
in general and PTSD in particular following exposure
to combat. Some interventions have been conducted
in the acute phase of combat situations, such as Front
Line Treatment (8, 9) or psychological debriefing (10),
which is the most commonly used crisis intervention.
Debriefing techniques are conducted mostly during
the acute phase of combat situations rather than during subsequent phases when these techniques might
be more suitable. In fact, therapy conducted during
acute phases is controversial. There are those who claim
that the mental reaction immediately after exposure to
a traumatic event is natural, and that instead of direct
intervention, professionals should simply “be with” the
victims as soon as the combat situation ends, in order
to help them “reconnect” with their natural strengths
and regain their mental/emotional balance (11, 12).
Raphael (13) suggests performing the intervention only
Address for Correspondence: Mrs. Yael Shoval-Zuckerman, Combat Stress Reaction Unit, Mental Health Division, Medical Corps, IDF 4 Simtat
Asaf Street, Ramat Hasharon 47275, Israel
Yshovalzuckerman@gmail.com
49
�EARLY GROUP INTERVENTION FOR RESERVE SOLDIERS
after a certain amount of time has passed, during which
time the event can be digested and processed. A similar
opinion is expressed by Mitchell (10), who emphasizes
the need for psychological readiness for intervention; this
readiness is enabled, according to him, only a significant
time after the event has happened.
Although the term psychological debriefing has
become controversial, researchers who have assessed
the efficacy of this technique with military personnel
(14) have found it to be effective with intact groups;
this effectiveness may be due to the fact that intragroup
processes are known to influence individual well-being
and because group debriefing is consistent with the
military tradition of after-action reviews (15). Other
interventions, such as Cognitive Behavioral Therapy (16,
17) and Exposure Therapy (18), have been conducted
in the second early phase (i.e., from one to six months
following the traumatic event).
It is critical for intervention to be based on the most
validated empirical findings. However, to date, noevidence-based consensus has been reached to support
a clear set of recommendations for intervention in the
acute and early phases that follow mass trauma (19).
Although many studies have found that acute and early
intervention following combat are effective, there are only
a few studies on the effect of interventions in subsequent
phases (from one month to several months after combat)
(6, 15). Moreover, critics of early interventions have
argued that these interventions cannot be conducted
among a wide variety of populations without taking
into account the differential effect (20) brought about
by interpersonal differences and differences in coping
styles among potential participants.
The current study had two aims: The first was to
examine the general efficacy of Early Group Intervention
(EGI) – an intervention conducted three months after
soldiers’ participation in a war. We sought to examine
whether soldiers who took part in the EGI would show
less distress after a traumatic incident, as well as more
improvement in functioning and physical health, than
the soldiers in the control group, who did not take part
in the EGI or in any other intervention. Second, in an
attempt to shed light on interpersonal differences, we
examined the contribution that EGI made to soldiers,
based on their coping styles.
REPRESSIVE COPING STYLE
A repressive coping style has been defined as the distancing of one’s self from anxiety-provoking threats through
50
diverting one’s attention away from the threat (21).
Other studies have suggested that the repressive coping style is an unconscious intra-psychic defense (22),
and that substantial and persistent use of this defense
mechanism turns it into a basic dimension of the personality (23) which is reflected in various cognitive and
behavioral processes (24). The most widely used definition
was introduced by Weinberger, Schwartz and Davidson
(25), who conceptualized repressive coping as a specific
combination of anxiety and defensiveness. Postulating
four combinations of responses to threat, Weinberger
defined repressors as individuals who express low anxiety
and high defensiveness.
Recent research has suggested that the repressive coping style can be a pragmatic form of coping that helps
people deal effectively with extremely aversive events
(26). It has been suggested that in certain circumstances,
repressing and avoiding thoughts, memories, and other
cues related to the traumatic event may in fact be adaptive
(27, 28).Ginzburg et al. (24) found that this coping style
might promote both short- and long-term adjustment to
traumatic events such as myocardial infarction. Similarly,
Palyo and Beck (29) found that after motor vehicle accidents, repressors reported fewer post-traumatic symptoms, anxiety, depression, and health problems than did
those who employed other coping styles.
The current study examined whether the efficacy of
EGI would differ according to individuals’ coping styles.
In light of the knowledge we currently have, we hypothesized that soldiers who were characterized by a regressive
coping style would have lower levels of distress following
participation in combat than would non-repressors. In
addition, we hypothesized that EGI would reduce posttraumatic distress among non-repressors, whereas no
change or even a worsening of symptoms would be found
among repressors. We assumed that EGI, which is based
on the principles of debriefing, might expose repressors
to threats and elicit a flood of thoughts and unpleasant
memories that they would try to divert. Consistent with
this view, it has been argued that interventions such as
debriefing disrupt the natural process of recovery from
trauma, especially for individuals who tend to use coping
strategies such as repression and avoidance (30, 31).
THE CURRENT INTERVENTION
The EGI model (32) was formulated after targeting the
special needs of the reserve soldiers, and in an attempt to
help them process the separation from their fellow unit
members and the return to their families and workplaces
�YAEL SHOVAL-ZUCKERMAN ET AL.
after the war. In addition to providing an outlet for the
articulation of thoughts and feelings, and to help foster
the development of coping mechanisms, this intervention conveyed the expectation that participants would
continue normative functioning in the future. This model
could also be used to identify soldiers who need further
treatment.
EGI is based on the assumption that the military group
provides a significant support network and source of
strength, enabling participants to overcome difficult
situations. In our case, the existing connection among
the soldiers provided social support that was crucial
for the success of the intervention (12). The staff of the
battalion and the professional workers from the Combat
Reaction Unit held a preparatory meeting, which included
familiarization with the EGI protocol, getting acquainted
with the group mediators (an officer and a professional
worker), coordination of the approach to the intervention, and the division of tasks during the intervention.
EGI emphasizes the transition from combat to home
and recognizes that this transition is a critical socialpsychological task.
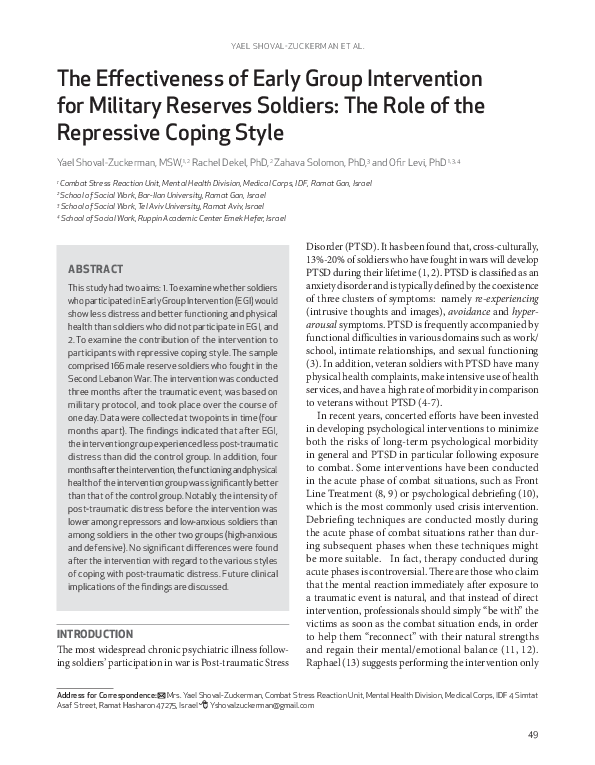
The intervention was based on a military stress debriefing protocol (33)(see Appendix 1) and was conducted by
the Combat Reaction Unit of the Israel Defense Forces
among soldiers who fought in the Second Lebanon War.
It was held over the course of one day. The intervention
consisted of three parts (see Figure 1): In the first part,
the soldiers reviewed the sequence of events that occurred
from the time of their release from army reserve duty
until the present. In the second part, they articulated
their thoughts and feelings at the present time (three
months after the war). In this way, they were given an
opportunity to relate to the losses they had experienced
in the war, and they were able to express feelings of guilt
and anger. In the third part of the intervention, the soldiers discussed their ability to continue functioning as
individuals and as a group (a platoon). The discussion
focused on the need to continue living, and the expectation that participation in the group would enable them
to resume regular functioning. Common symptoms and
difficulties in coping with daily living – e.g., relating to
spouses, family members or co-workers – were discussed
in the intervention.
Emphasis was placed on the strength of the group
and the positive and functional coping mechanisms that
the soldiers used. The intervention was conducted by a
professional practitioner (mental health officer) and the
commander of the relevant military unit.
Figure 1: Flowchart of Intervention
51
�EARLY GROUP INTERVENTION FOR RESERVE SOLDIERS
METHOD
PARTICIPANTS AND PROCEDURES
Participants in the study were 166 male reserve soldiers
and officers in the Israel Defense Forces, who belonged to a
battalion which sustained numerous casualties in the Second
Lebanon War (2006). Data was collected in two stages.
Stage 1. The whole battalion was called for a oneday intervention during reserve duty (three months
after the war). The intervention followed a structured
protocol, and each group comprised an original organic
unit. The intervention was facilitated by a professional
worker (mental health officer) and a commander of the
relevant military unit. Randomization was not feasible
due to military constraints. A partial solution to the
randomization problem was to form an internal control
group consisting of soldiers who did not participate in
the intervention for various reasons: (28% were studying,
25% were abroad, 23.5% had work obligations, 16% were
unintentionally not invited, and 7.4% had injuries).
The soldiers who participated in the intervention
completed the questionnaires before it started. The control
group filled out questionnaires at home during the week
following the intervention.
Stage 2. Four months after the intervention, the members of the battalion were called again for reserve duty. At
that time, the members of the Combat Reaction Unit distributed a second questionnaire to the soldiers. Of those
who filled out the questionnaires during this stage, 98 had
participated in the intervention, and 68 had not (the control group). No participants in the study had dropped out
between the two stages of data collection. No significant
differences were found between the participants in the two
research groups with regard to combat exposure except for
proximity to fire: Both groups of soldiers reported high
levels of exposure (Χ2=3.52, df=3,p=.32), such as exposure
to injury and death (Χ2=.0.10, df=1, p=.75), evacuation of
the wounded or dead (Χ2=0.34, df=1, p=.56), proximity
to the range of fire (control=91.2%, intervention=98.0%,
Χ2=4.03, df=1,p=.05), and risk of injury or death (Χ2=1.52,
df=3,p=.68). In addition, no differences were found in
background characteristics: 90% were born in Israel,
70% were single, 64.5% were employed, and 32% were
students. Most of the participants were reserve soldiers
(86.1% reserve soldiers, and 13.9% officers). A significant
difference was found between the groups regarding years
of education (M=14.37 SD=2.23 for the intervention
group, and M=13.70, SD=1.77 for the control group,
t=2.08, df=164, p=.04). Differences were also found in
52
the recent significant event (control=22.1%, intervention=10.2%, Χ2=4.41, df=1, p=.04), and these differences
were controlled for during the data analysis.
MEASURES
1. Socio-demographic and military information (stages
1+2): This measure included information on the participants’ marital status, age, number of children, country
of origin, year of immigration, education, occupational
status, and military rank.
2. Combat exposure (stage 1): The measure was
developed by Schwarzwald, Solomon, Weisenberg and
Mikulincer(34)te> and consisted of six items that examined the soldiers’ exposure to combat: complexity of
the battle, proximity to the range of fire, exposure to
injury and death, evacuation of the wounded and dead
, and risk of injury or death. A factor score was derived
from a factor analysis (M=0, SD=1, percent variance
explained=.51.5).
3. PTSD Inventory (stages 1+2): PTSD was measured by the PTSD Inventory, a self-report scale based
on the DSM-IV (35). The scale consisted of 17 items that
describe intrusive, avoidant and hyper-arousal symptoms.
Participants were asked to indicate how often they had
experienced each symptom during the previous month
on a scale ranging from 1 (not at all) to 4 (very often). The
severity of PTSD was calculated as the mean severity of
symptoms. The Cronbach’s alpha internal consistency of
the questionnaire used in the current study was high (.93),
and the scale was found to have high convergent validity
compared with diagnoses made by experienced clinicians
on the basis of structured clinical interviews (34).
4. Functioning: This dimension was measured on
the basis of two questionnaires. Questionnaire stage 1.
This questionnaire consisted of one item relating to the
participant’s level of functioning over the previous two
weeks. Responses were based on a scale ranging from 0
(very bad) to 5 (very good). Questionnaire stage 2. This
questionnaire assessed general psychological functioning
over the previous two weeks using the Psychotherapy
Outcome Assessment and Monitoring System-Trauma
Version (POAMS-TV)(36). Responses were based on a
5-point Likert-type scale ranging from 0 (extreme distress
or dissatisfaction) to 4 (optimal functioning or satisfaction). In this study, one score for functioning (e.g., work/
school performance/attendance) was calculated for the
mean of the scores on the 10 items. The Cronbach’s alpha
of the questionnaire used in this study was high (.90).
5. Self-rated health (stages 1+2): Based on a question-
�YAEL SHOVAL-ZUCKERMAN ET AL.
naire developed by Benyamini and Idler (37), participants
were asked to assess their current physical health on a scale
comprised of three levels (1, 2, 3): bad, moderate, and good.
6. Repressive Coping Scale (stages 1+2): This selfreport measure consisted of 58 items, which combined
two scales: Manifest Anxiety (Taylor Manifest Anxiety
Scale)(38), and Defensiveness (the Marlow-Crowne Social
Desirability Scale)(39). Participants were asked to indicate
whether or not each item described them, on a dichotomous scale – 0 (no) 1 (yes). The repressive coping style
was determined by the median scores on the two scales.
Participants with anxiety scores below the median and
defensiveness scores above the median were classified as
repressors. In addition, three categories of non-repressors
were identified: low-anxious individuals (anxiety and
defensiveness scores below the median); high-anxious
individuals (anxiety score above the median, and defensiveness score below the median); and defensive individuals
(anxiety and defensiveness scores both above the median).
The analyses reflected both the dichotomous distinction
(repressors vs. non-repressors) and the four-category
classification (repressors, low-anxious, high-anxious and
defensive). The combination of anxiety and defensiveness
as reflecting a repressive coping style has been validated in
previous studies (24). The Cronbach’s alpha for the current
sample was high, both for the Taylor Manifest Anxiety
Scale (.85) and the Marlow-Crowne Social Desirability
Scale (.78).
RESULTS
DIFFERENCES IN LEVELS OF PTSD, PHYSICAL HEALTH, AND
FUNCTIONING BEFORE AND AFTER THE INTERVENTION
To examine the hypothesis relating to the relationships
between participation in the intervention and reduc-
tion of PTSD symptoms, ANCOVAs for PTSD, Physical
Health, and Functioning were performed with repeated
measures for each stage of data collection, with groups
(intervention and control) as the independent variable
and education, proximity to combat, and the significant
event as covariates. The analysis revealed significant
group and interaction effects.
The results of Bonferroni tests presented in Table 1
reveal that participants in the control group reported
higher post-traumatic distress symptoms than did participants in the intervention group both before and after
intervention. Contrary to the hypothesis, there was no
improvement among soldiers in the intervention group.
However, while PTSD symptoms remained stable among
participants in the intervention group, the symptoms
increased among participants in the control group.
Physical Health. Significant differences were found
between participants in the two groups with regard to
self-assessed health: F(1, 161)=3.98, p<.05. Levels of
physical health among participants in the control group
were lower than among those in the intervention group
(M=2.53, and M=2.70, respectively, with a lower score
representing a greater negative change).
Functioning. Due to the use of different measures
before and after the intervention, comparisons of the two
groups were performed separately at each time point,
and no significant change was found. Comparisons of
the groups before the intervention revealed no significant
differences – F(1, 161)=0.12, p>.05) – although the levels
of functioning at that time were lower among participants
in the intervention group than among participants in the
control group (M=2.54, SD=1.12; and M= 2.60, SD=.88,
respectively). After the intervention, the levels of functioning among participants in the intervention group
were significantly better than among the participants
in the control group (M=3.18, SD=0.53; and M=2.94,
Table 1: Means and Standard Deviations of Outcome Measures, by Group and Timing: controlling for education, proximity to
combat, and significant event
Variable
Total PTSD
Physical Health
Intervention group (n=98)
Control group (n=68)
Before
Before
After
After
F values
Ƞ2
F(1,161)
F(1,161)
F(1,161)
Group
Time
Group x Time
Means
1.52
1.47
1.63
1.77
5.97*
1.08
12.53**
SD
0.45
0.43
0.65
0.69
.03
.01
.07
Means
2.56
2.85
2.46
2.60
3.98*
0.00
2.27
SD
0.61
0.42
0.74
0.7
.02
.00
.01
*p<.05. **p<.01.
53
�EARLY GROUP INTERVENTION FOR RESERVE SOLDIERS
SD=0.77, respectively: F(1, 161)=5.52, p<.01).
THE ASSOCIATION BETWEEN COPING STYLE AND LEVELS
OF DISTRESS
First, we examined whether there were differences
between the two groups with regard to the distribution
of different repressive styles. Table 2 presents the joint
distribution of coping style and group. As can be seen in
the table, the percentage of soldiers in each coping style
category was similar for both groups, and no significant
differences between the groups were found: X2(3)=.86,
p>.05. In addition, Cohen’s Kappa was calculated to
determine style consistency over time, revealing a high
level of agreement over time (Kappa=.75, p<.001), while
no difference in style between groups was observed.
In order to examine the hypothesis that after participation in combat, soldiers who have a repressive coping style
will have lower levels of distress than non-repressors, a
one-way ANOVA was conducted, with PTSD symptoms
as the dependent variable and the four coping styles as the
independent variable (F=18.07, df=3,162, p<.001). The
Bonferroni post-hoc analysis supports this hypothesis:
soldiers who were characterized by low anxiety or by being
repressors reported lower levels of PTSD symptoms following combat than did soldiers who were characterized
by high anxiety or defensiveness (see Table 3).
To examine the hypothesis that levels of PTSD would
decrease among non-repressive participants as a result
of the intervention, whereas there would be no change
or even an increase in the levels of PTSD symptoms
among repressors, a two-way ANOVA was conducted
in regard to change in the level of PTSD symptoms (preintervention level minus post-intervention level) x group
and coping style. Only the group effect was found to be
significant – F(1, 157)=14.96, p<.001 – a finding which
fails to support this hypothesis, and replicates the first
hypothesis. Moreover, there was no change in levels of
PTSD among participants in the intervention group,
whereas levels of PTSD increased among participants in
the control group. Neither coping style nor interaction
effects were significant: F (3, 157)=0.50, p>.05, and F(3,
157)=1.88, p>.05, respectively.
DISCUSSION
The first aim of the research was to examine whether
soldiers who had participated in EGI would show less
post-traumatic stress than those who had not participated
in the intervention. The findings indicated that after EGI
participants in the control group experienced more posttraumatic stress than did the participants in the intervention group. However, contrary to the research hypothesis,
there was no improvement in PTSD symptoms among
the soldiers in the intervention group. Nevertheless,
four months after the intervention,
Table 2: Combined Distribution of Coping Style, by Group
the levels of functioning and physiControl
Intervention
Total
cal health among the participants
Coping style
Frequency
%
Frequency
%
Frequency %
in the intervention group were
Low-anxious
17
25.0
29
29.6
46
27.7
significantly better than among the
Repressors
17
25.0
27
27.6
44
26.5
participants in the control group.
High-anxious
15
22.1
18
18.4
33
19.9
And four months after the intervention, the soldiers in the control
Defensiveness
19
27.9
27
24.5
43
25.9
group assessed their own physical
Total
68
100
98
100
166
100
health as worse than it had been a
year earlier.
Table 3: Means, Standard Deviations, and F Values of Stress Indices
The lack of improvement in
(Prior to EGI) by Coping Style
PTSD symptoms among participants
1
3
4
2
in the intervention group following
Low
Source of
High
Repressor Defensiveness
EGI does not necessarily indicate
anxious anxious
F=(3,162) Ƞ2 differences
that the intervention wasn’t effective.
N=46
N=33
N=44
N=43
Rather, this lack of improvement
Total M
1.30
1.72
1.34
1.94
18.07 ***
.25 1,3<2,4
might be attributed to the nature of
PTSD
the intervention, which focused on
a discussion of responses to trauma.
SD 24.
53.
34.
69.
As such, the EGI may have raised
*** p<.001
the participants’ awareness of their
54
�YAEL SHOVAL-ZUCKERMAN ET AL.
symptoms and, paradoxically, inhibited future improvement (40, 41).
The findings also revealed that following the intervention, the participants in the control group experienced
more post-traumatic distress than did the participants
in the intervention group. They also had poorer functioning and more physical health problems than did the
participants in the intervention group. As there was no
random allocation, one cannot discount the possibility
that there might have been differences between the two
groups: for instance, those who did not take part in the
intervention might have been more vulnerable to begin
with. As suggested previously, it may be that soldiers with
PTSD, who have a high awareness of their mental and
physical problems, tend to assess their situation as more
severe than soldiers without PTSD (42). This explanation
is also consistent with the approach of researchers who
argue that people who have experienced a traumatic
event tend to develop hypochondria, and that somatic
problems play a central role in their lives (43).
Two hypotheses regarding the repressive coping style
were examined in this research. The research findings
support the hypothesis that repressors will show higher
levels of adaptation following traumatic events than will
non-repressors. The repressors showed a lower intensity
of post-traumatic distress, as did the participants in the
low-anxious group versus the participants in the other
two groups (high-anxious and defensive). These findings
are consistent with the results of another study which
revealed that among people who had been in a motor
vehicle accident, there were no significant differences
between repressors and low-anxious individuals with
regard to levels of PTSD and depressive symptoms (29).
There are several explanations for the contribution of
repressive coping to adaptive behavior: First, repressors
are protected by their primary appraisal of stressful events
(44), that is, by their perceptions and interpretations
of threatening cues. Second, repressors seem to have
exceptional control over what they pay attention to in
the presence of threat, a process that may foster resilience
in the face of trauma (45). They also recall fewer details
of stressful experiences (46), and they remember fewer
negative events (21). These findings suggest that repressors may be less prone to develop PTSD because they
employ selective attention during and after a traumatic
event, and thus perceive the event as less threatening
than do non-repressors (47). Third, it has been argued
that a major motive for repressive coping is maintaining
a positive self-image (22). Various findings have indicated
that in comparison with non-repressors, repressors tend
to ascribe fewer negative and more positive attributes to
themselves (48).
The second hypothesis – i.e., that the intervention
would reduce post-traumatic distress among non-repressors whereas post-traumatic symptoms would remain
unchanged or even worsen among repressors – was not
supported. This hypothesis derived from our assumption
that EGI, which is based on the principles of debriefing,
would expose repressors to threats that might cause a
flood of thoughts and unpleasant memories that they
would try to divert. However, no significant differences
were found after the intervention with regard to the
various styles of coping with post-traumatic distress.
Several possible explanations can be offered for this finding. As mentioned, various researchers have indicated
that repressors have a more positive self-perception than
non-repressors (49), and that they pride themselves
on appearing self-controlled and unemotional (22).
Consistent with these arguments, it is possible that the
EGI allowed the repressors in the present study to maintain their positive self-perception since behaviors that
are generally perceived as failures were redefined in the
intervention as reactions that are reasonable to expect
following the return to civilian life (50).
Furthermore, EGI does not pose a threat to the selfimage of repressors. If they describe themselves as possessing effective coping skills, they receive encouragement from the group and from the facilitators. In that
context, they are not exposed to threatening feelings from
their peers or to feelings of failure and loss of control.
Consistent with the findings of Ginzburg et al. (24), in
this study the repressive coping style was a protective
factor, which contributed more to preventing mental
health symptoms than it did to promoting mental health
resilience and functioning.
LIMITATIONS OF THE RESEARCH
This study had several methodological limitations, as the
intervention was designed to meet military needs (i.e.,
minimizing risks for long-term psychological problems
and assisting soldiers in distress) and was not designed
for systematic research. Rather, the research was planned
after the intervention took place in order to address the
gap between the need for intervention in the military
and the lack of studies assessing its effectiveness.
The main limitation was that that there was no random
allocation to research groups. Moreover, because the EGI
was conducted by the military and aimed to mitigate
55
�EARLY GROUP INTERVENTION FOR RESERVE SOLDIERS
distress among all soldiers, a random sample could not
be attained. Nonetheless, no significant differences were
found between the two groups in the main background
variables, suggesting that in fact there was a basis for
comparing the two groups.
Another limitation of this study was that the control
group had significantly higher PTSD symptoms at Time
1 than did the intervention group, a drawback that might
be related to the non-random allocation to the research
groups.
The second stage of data collection occurred while the
soldiers were in reserve duty. Perhaps the renewed contact
with the army four months after the war influenced their
feelings and reawakened memories and thoughts that
biased their responses (i.e., reflecting more symptoms and
higher intensity of distress). In addition, some changes
were made in the questionnaires between the two stages
of data collection due to logistical constraints. Other
limitations include the lack of objective measures such
as performance on military tasks and other observations.
IMPLICATIONS FOR FUTURE RESEARCH AND PRACTICE
To better understand the contribution of each component
of EGI to preservation or improvement of behaviors
among participants in an intervention, there is a need
for additional long-term follow-up studies dealing with
each of the specific aspects of the intervention method.
The clinical advantage of EGI is that it provides a basis
for identifying soldiers with PTSD while they are doing
reserve duty. Findings have revealed that at a later stage,
when the soldiers are at home, they need to take initiative
to continue treatment. As a result, those who are not proactive might not receive essential support. Furthermore,
if the soldiers at risk are identified immediately following
military service, treatment can be provided in closer
temporal proximity to the traumatic event. Another
significant advantage of the intervention for soldiers
who remain in their organic unit relates to the informal
interaction among the soldiers and their immediate
commanders, who constitute a significant support system
and a source of strength that helps them cope with the
situation.
The finding that repressors showed a lower intensity
of post-traumatic distress indicates that the repressive
coping style is a mechanism that can facilitate adaptation
after a traumatic event. Therefore, the clinical tendency
to encourage all soldiers who have been exposed to a
traumatic event to talk about their experience out of a
concern that repression of the event might worsen their
56
condition was not supported in the present study. Finally,
little is known about the development of repressive coping
and the ability to change that style. Hence, especially in
light of its protective function, it would be worthwhile
to conduct further research on the role of the repressive
style in the process of coping with traumatic events.
References
1. Cigrang JA, Peterson AL, Schobitz RP. Three American troops in Iraq:
Evaluation of a brief exposure therapy treatment for the secondary
prevention of combat related PTSD. PCSP 2005; 1: 1-25.
2. Solomon Z, Neria, Y, Ohry A, Waysman M, Ginzburg K. PTSD among
Israeli former prisoners of war and soldiers with combat stress reaction:
A longitudinal study. Am J Psychiatry 1994;151:554-559.
3. American Psychiatric Association. Diagnostic and Statistical Manual of
Mental Disorders. DSM-IV-TR. Washington, D.C.: American Psychiatric
Association, 2000.
4. Kutter CJ, Wolf E J, McKeever VM. Predictors of veteran’s participation
in cognitive-behavioral treatment for PTSD. J Trauma Stress 2004;17:157162.
5. Shalev AY. What is posttraumatic stress disorder? J Clin Psychiatry
2001;62:4-10.
6. Hourani LL, Council CL, Hubal RC, Strange LB. Approaches to the
primary prevention of posttraumatic stress disorder in the military:
A review of the stress control literature. Mil Med 2011;176:721-730.
7. Toblin RL, Riviere LA, Thomas JL, Adler AB, Kok BC, Hoge CW. Grief
and physical health outcomes in U.S. soldiers returning from combat.
J Affect Disord 2012;136:469-475.
8. Solomon Z, BenbenishtyR. The role of proximity, immediacy and
expectancy in front line treatment of combat stress reaction among
Israelis in the Lebanon War. Am J Psychiatry1986;143:613-617.
9. Solomon Z, Shklar R, Mikulincer M. Front line treatment of combat
stress reaction: A 20 year longitudinal evaluation. Am J Psychiatry
2005;162:2309-2314.
10. Mitchell JT. When disaster strikes: The critical incident stress debriefing
process. JEMS 1983;8:36-39.
11. Tuckey RM. Issues in the debriefing debate for the emergency services:
Moving research outcomes forward. Clin Psychol: Science and Practice
2007;14:106-116.
12. Wessely S, Deahl M. Psychological debriefing is a waste of time. Br J
Psychiatry2003;183:12-14.
13. Raphael B. Preventive intervention with the recently bereaved. Arch
Gen Psychiatry1977;34:1450-1454.
14. Lewis SJ. Combat stress control: Putting principle into practice. In: In
Adler AB, Castro CA, Britt TW, editors. Military life: The psychology
of serving in peace and combat: Operational Stress. Westport: Preager
Security International, 2006.
15. Adler AB, McGurk D, Bliese PD, Hoge CW, Castro CA. Battlemind
debriefing and battlemind training as early intervention with soldiers
returning from Iraq: Randomization by platoon. Sport, Exercise, and
Performance Psychology 2011;1:66-83.
16. Hembree EA, Foa EB. Posttraumatic stress disorder: Psychological
factors and psychosocial interventions. J Clin Psychiatry2000;61:33-39.
17. Meichenbaum D. Cognitive behavior modification. Morristown, New
Jersey: General Learning, 1974.
18. Foa EB, Rothbaum BO. Treating the trauma of rape: Cognitive- behavioral
therapy for PTSD. New York: Guilford,1998.
19. Hobfoll SE, Watson P, Bell CC, Bryan, RA, Brymer MJ, Friedman MJ,
Ursano R J. Five essential elements of immediate and mid-term mass
�YAEL SHOVAL-ZUCKERMAN ET AL.
trauma intervention: Empirical evidence. Psychiatry 2007;70:283-315.
20. Bisson JI, McFarlane AC, Rose S, Ruzek JI, Watson PJ. Psychological
debriefing for adults. In: Foa EB, Keane TM, Friedman MJ, Cohen
J, editors. Effective treatments for PTSD. New York: Guilford, 2009.
21. Langens TA, MorthS . Repressive coping and the use of passive and
active coping strategies. Pers Individ Dif 2003;35:461-473.
22. Weinberger DA. The construct validity of repressive coping style.
In: Singer JL, editor. Repression and dissociation: Implications for
personality theory, psychopathology, and health. Chicago: University
of Chicago, 1990.
23. Bonanno GA, Singer JL. Repressive personality style: Theoretical and
methodological implications for health and pathology In: Singer JL,
editor. Repression and dissociation: Implications for personality theory,
psychopathology, and health. Chicago: University of Chicago, 1990.
24. Ginzburg K, Solomon Z, Bleich A. Repressive coping style, acute stress
disorder, and posttraumatic stress disorder after myocardial infraction.
Psychosom Med 2002;64:748-757.
25. Weinberger DA, Schwartz GE, Davidson R J. Low-anxious, high-anxious,
and repressive coping style: Psychometric patterns and behavioral and
physiological responses to stress. J Consult Clin Psychol 1979;63:361-368.
26. Bonanno GA. Resilience in the face of potential trauma. Current
Directions in Psychological Science 2005;14:135-138.
27. Erdelyi MH. Repression, reconstruction and defense: History and
integration of the psychoanalytic experimental frameworks. In: Singer JL,
editor. Repression and dissociation: Implications for personality theory,
psychopathology, and health Chicago: University of Chicago, 1990.
28. Kaminer H. Repression during sleep as an adaptive coping mechanism for
Holocaust survivors: A research stud. In: Malkinson R, Rubin SS,Witztum
E, editors. Loss and bereavement in Jewish society in Israel. Jerusalem:
Cana Publishing House, 1993.
29. Palyo SA, Beck JG. Is the concept of ‘‘repression’’ useful for the
understanding chronic PTSD? Behav Res Ther 2005;43:55-68.
30. Bisson JI, Jenkins P L, Alexander J, Bannister C. Randomized controlled
trial of psychological debriefing for victims of acute burn trauma. Br J
Psychiatry1997;171:78-81.
31. Raphael B, Meldrum L, McFarlane AC. Does debriefing after psychological
trauma work? Br J Med 1995;310:1479-1480.
32. Levi O, Shoval Y. Continous group intervention – A protocol for unique
intervention with combat reserve units. Sichot 2010;24:275-282.
33. Levi O. Long-term group therapy for chronic post trauma victims
[Internet]. www.sfareem.co.il .2006[cited Nov. 24, 2009].
34. Schwarzwald J, Solomon Z, Weisenberg M, Mikulincer M. Validation of
the impact of events scale for psychological sequels of combat. J Consult
Clin Psychol 1987;55:251-256.
35. Solomon Z, Benbenishty R, Neria Y, Abramowitz M, Ginzburg K, OhryA.
Assessment of PTSD: Validation of the revised PTSD Inventory. Isr J
Psychiatry Rel Sci 1993;30:110-115.
36. Green JL, LowryJL, Kopta S. M. College students versus college counseling
center clients: What are the differences? J College Stud Psychother
2003; 17:25-37.
37. Benyamini Y, Idler EL. Community studies reporting association between
self-rated health and mortality: Additional studies, 1995-1998. Res
Aging 1999;21:392-401.
38. Taylor JA. A personality scale of manifest anxiety. J Abnorm Soc Psychol
1953; 48 285-290.
39. Crowne DP, Marlow DA. The approval motive: Studies in evaluation
dependence. New York: Wiley,1964.
40. 40.Deahl M, Srinivasan M, Jones N, Thomas J, Neblett C, Jolly A.
Evaluating psychological debriefing: Are we measuring the right
outcomes? J Trauma Stress 2001; 14:527-529.
41. MacDonald CM. Evaluation of Stress debriefing interventions with
military populations. Mil Med 2003;168:961-968.
42. Elhai JD, Kashdan TB, Snyder JJ, North TC, HeaneyCJ, Frueh BC.
Symptom severity and lifetime and prospective health service use among
military veterans evaluated for PTSD. Depress Anxiety 2007;24:178-184.
43. Stretch RH. Post traumatic stress disorder among Vietnam-era veterans.
In: Figley CR, editor. Trauma and its wake: Traumatic stress theory,
research and intervention. New York: Brunner/Mazel,1986.
44. Lazarus RS, Folkman S. Stress, appraisal and coping. New York: Springer, 1984.
45. McNally RJ, Hatch JP, Cedillos EM, Luethcke CA, Baker MT, Peterson
AL, Litz BT. Does the repressor coping style predict lower posttraumatic
stress symptoms? Mil Med 2011; 176:752-756.
46. Sparks GG, Pellechia M, Irvine C. The repressive coping style and fright
reactions to mass media. Communic Res 1999;26:176-192.
47. Coifman KG, Bonanno GA, Ray RD, Gross JJ. Does repressivecoping
promote resilience? Affective–autonomic response discrepancy during
bereavement. J Pers Soc Psychol 2007;92:745-758.
48. Bybee J, Kramer A, Zigler E. Is repression adaptive? Relationships to
socioemotional adjustment, academic performance, and self-image.
Am J Orthopsychiatry 1997;67:59-69.
49. Furnham A, Petrides KV, Spencer-Bowdage S. The effects of different
types of social desirability on the identification of repressors. Pers
Individ Dif 2002;33:119-130.
50. Malcolm AS, Seaton J, Perera A, Sheehan DC, Van Hasselt VB. Critical
incident stress debriefing and law enforcement: An evaluative review.
Brief Treat Crisis Interv 2005;5:261-278.
57
�EARLY GROUP INTERVENTION FOR RESERVE SOLDIERS
APPENDIX 1 - THE OPENING STAGE
Commander. 1. Goal of the intervention: “We went
through harsh events (the commander should direct
towards events experienced during the war) during the
last reserve service, after which we returned to our life
routine. In our session today we will try to clarify what
our life routine looks like since we were discharged from
reserve duty, with emphasis on the emotional processes
that accompanied the process of our return to civilian
life. It is important that each of you will express himself.
We on our part will enable each of you to do so. In this
way we will learn how each person coped and is coping
with the return to civilian life on the background of the
war events we experienced and how we as a team need
to cope in preparation for our next reserve duty.”
2. Framework: “The session is divided into three
rounds. In the first round we will describe the sequence
of events that each of us experienced since his discharge
from reserve duty and will examine, at the facts level,
how each of you copes with the routine of his civilian life
with emphasis, as mentioned before, on the encounter
with “civilianship” after being discharged from reserve
duty – after the war. This second part will last about two
hours. After a break we will convene for a second round
that will last for about three hours, with a break in the
middle, in which we will deal with our feelings from a
distance of the time that has elapsed since the war events
and since our discharge from reserve duty. During the
third round we will summarize the discussion for about
one hour and will discuss the future and the expected
schedules. This entire day will be headed by (indicate
name) – a therapist at the Combat Reaction Unit.”
3. Rules: “In order to create an atmosphere that will
enable success of this session, I would like to ask you to
make sure of the following: do not talk on your mobile
phones because succession is important, and for mutual
respect, do not enter and leave during the talk, allow
each person to finish what he is saying, do not attack, do
not criticize (it must be emphasized that this is not an
operational debriefing), and finally, it is very important
that each of you will speak. If anyone has difficulty with
this, he should at least describe his position and role
during the event that took place in the war.”
Therapist. 4. Rationale: “‘The early group intervention’ is intended to prevent the development of effects
that belong to what we call the post-traumatic stress
disorder, which I will detail right away. This disorder
may develop among soldiers who, like you, experienced
combat events in which soldiers were killed and injured.
58
We know from studies and from reports of professionals who experienced such models of talks that the talk
within a group of people who know each other well and
who experienced the event together is very helpful for
emotional alleviation and for preventing post-trauma.
This talk is supposed to take place at a distance of about
three months from the previous talk you had, the ‘team
talk after the event’ during the last two days of your
reserve duty, because it is believed that it is possible
to prevent the development or exacerbation of effects
that belong to the post-traumatic stress disorder during
the first three months after exposure to an event. This
talk, of ‘early group intervention,’ is actually a continuation of the previous talk in which you participated, and
comprises another opportunity for all of you to describe
your experiences and emotions and to learn how each of
you is coping with civilian life on the background of the
event which you experienced during the war. It is also
supposed to increase the cohesion, sharing and mutual
care among you and will help us, the therapists and the
commanders, identify and suggest, to those for whom
these talks were not helpful, to receive individual therapy
at the Combat Reaction Unit.”
5. Psycho-education: “Chronic post-trauma develops,
according to the research literature, over three months and
is characterized by three groups of symptoms: ‘avoidance’
of thoughts about the event or contact in reality with
things that are reminiscent of the event, for example:
contact with the army or watching news that broadcasts
pictures from a war, ‘hyperarousal’ which is expressed
in alertness on a background of the tension created by
the feeling that another harsh event can happen, which
sometimes leads to panic from noises reminiscent of
the sound of explosives, and ‘intrusiveness,’ which is
expressed in nightmares and unceasing dreams and
thoughts about the event. All three of these symptoms
eventually impair functioning, since if one does not sleep
well because of dreams and nightmares one becomes
tense during the day, the level of attention decreases and
the ability to function well at work, as a parent or as a
partner, is impaired. Furthermore, think about the fact
that when a person who was exposed to a traumatic event
is busy avoiding thinking about the event or coming into
contact with things that are taking place in reality that are
reminiscent of that event during his waking hours, this
increases his difficulty to function even more. We would
like to prevent all of this or at least reduce the intensity
of the symptoms among those who are already suffering
from them, and as I mentioned already, the ‘window of
�YAEL SHOVAL-ZUCKERMAN ET AL.
opportunity’ for prevention is within this range of time,
i.e., in the early months after exposure.
It is important for me to indicate that even if symptoms
characteristic of post-trauma have developed among some
of the people sitting here, and even if after the session
today some of the symptoms will remain, there are still
things that can be done. First of all you must remember
that people who experienced such a harsh event react to
the event at the emotional level. We know from studies
that not less than 80% of the people who are exposed
suffer from at least one symptom of a stress reaction,
which is the first stage of post-trauma, but the symptoms
usually disappear. How? By talking with friends, partners,
family, etc. Thus, they recover without any help from a
professional by spontaneous talk. What is done here is
something more structured, but is based on the idea that
one must talk about things, because ‘talk’ apparently
helps. Of course, your belief that it is possible to feel
better and that it is possible to again function well as a
team is also very important. Finally, it is important to
stress that if there is no improvement among someone
who already suffers from symptoms, he can come to us
at the CRU for individual help. Such help is supposed,
in the end, to help reduce the intensity of the symptoms
and improve the quality of functioning.”
APPENDIX 2 - SECOND STAGE
Second Round
Therapist. Explanation of the different losses (friends,
relatives, worldview, self-trust, confidence, trust in commanders, trust in operational ability, loss of motivation)
as a result of exposure to traumatic events.
Commander. “Based on what (should mention
the name of the therapist with whom he is working)
described, it is important that we talk about each of our
losses. What did each of us lose during this event?”
After each participant referred to this question, the
therapist should ask: “What are the emotions that accompany the loss?” (The therapist should focus the talk on
anger and guilt by reflection, confrontation, leading
questions, etc.)
APPENDIX 3 - SECOND STAGE
Third Round
Commander. “Based on the talk today, what things do
you think need to be taken from here for the future at
the personal level and at the team level?”
Therapist. Stressing the positive forms of coping (for
example: reflection of the component of sharing and
receiving support from the partner).
Commander. “I would now like to ask each of you to
indicate at least one thing that he received from the group
today and what his message is to the group.” After the
discussion the commander summarizes the intervention
according to the following points: (1) Summarize the
session up to this point (major and positive components
that were prominent around the return to functioning
after the discharge, prominent feelings and prominent
recommendations for future coping). (2) Speak about
the moral and ethical (comradeship) commitment “to
go on.” (3) Speak about the importance of “to go on” for
the individual and for the team.
59
�
 rachel dekel
rachel dekel