The document provides details of a nursing care plan for a patient with acute gouty arthritis including diagnoses, needs, desired outcomes, nursing interventions and rationales. The care plan addresses the patient's pain, activity intolerance and self-care deficits related to musculoskeletal impairment. Nursing interventions include medication administration, range of motion exercises, mobility assistance, and teaching about diet and lifestyle modifications. The goal is to relieve pain, increase activity tolerance and promote independence in self-care activities.
Copyright:
Attribution Non-Commercial (BY-NC)
Available Formats
Download as DOCX, PDF, TXT or read online from Scribd
The document provides details of a nursing care plan for a patient with acute gouty arthritis including diagnoses, needs, desired outcomes, nursing interventions and rationales. The care plan addresses the patient's pain, activity intolerance and self-care deficits related to musculoskeletal impairment. Nursing interventions include medication administration, range of motion exercises, mobility assistance, and teaching about diet and lifestyle modifications. The goal is to relieve pain, increase activity tolerance and promote independence in self-care activities.
The document provides details of a nursing care plan for a patient with acute gouty arthritis including diagnoses, needs, desired outcomes, nursing interventions and rationales. The care plan addresses the patient's pain, activity intolerance and self-care deficits related to musculoskeletal impairment. Nursing interventions include medication administration, range of motion exercises, mobility assistance, and teaching about diet and lifestyle modifications. The goal is to relieve pain, increase activity tolerance and promote independence in self-care activities.
Copyright:
Attribution Non-Commercial (BY-NC)
Available Formats
Download as DOCX, PDF, TXT or read online from Scribd
The document provides details of a nursing care plan for a patient with acute gouty arthritis including diagnoses, needs, desired outcomes, nursing interventions and rationales. The care plan addresses the patient's pain, activity intolerance and self-care deficits related to musculoskeletal impairment. Nursing interventions include medication administration, range of motion exercises, mobility assistance, and teaching about diet and lifestyle modifications. The goal is to relieve pain, increase activity tolerance and promote independence in self-care activities.
Copyright:
Attribution Non-Commercial (BY-NC)
Available Formats
Download as DOCX, PDF, TXT or read online from Scribd
Download as docx, pdf, or txt
You are on page 1/ 10
Chapter IX Nursing Care Plan
Nursing Care Plan 1 DIAGNOSIS NEED DESIRED OUTCOMES INTERVENTION RATIONALE EVALUATION MODIFIED INTERVENTI ON RATION ALE
Acute Pain r/t disease process secondary to Acute Gouty Arthritis Subjective cue: Sakit lang gid maghulag. Indi ko makalakat kay masakit, as verbalized by the patient. -With Pain Scale of 7 where 10 is the highest pain perceived and 1 is the lowest. Objective cues: Facial grimace elicited, pale. Skin warm to touch Irritability noted due to discomfort from pain.
P H Y S I O L O G I C N E E D
After 8 hours of nursing intervention: General Objective: Report pain is relieved or controlled and promote wellness Specific: a. Express understanding of situation and individual treatment regimen and safety measures. b. Decrease Pain Scale from 7 to 5 where 10 is
INDEPENDENT: Goal Met: a. Able to cooperate with the procedures done but still has limited ability to express feelings and perception because of Aphasia.
a. Urge the client to drink 2 to 3 L of fluid daily and to report any decrease in urine output. b. Asses level of pain felt.
To monitor any abnormaliti es in input and output.
To determine how intense the pain felt.
c. Provide measure to promote comfort and reduce pain.
b. Pain Scale decreased from 7 to 5 where 10 is the highest pain perceived and 1 is the To alleviate lowest. pain when present. Nonpharmacol
VS: T: 37.5C CR:80 bpm R:27cpm BP:120/70 mmHg Background knowledge: Formation of tophus deposits in soft tissues
the highest pain perceived and 1 is the lowest. c. Maintain or increase strength and function of affected and/or compensatory body part. d. Assess patient in performing deep breathing measures to promote relaxation
ogic therapies can also lessen any pain felt. d. Teach the client about dietary modifications to limit foods high in purine (e.g. organ meats, anchovies, sardines, shellfish, chocolate, meat extracts).
Avoiding food that may trigger disease may lessen d. Able to relax by performing the chance deep breathing of measures recurrence.
c. Able to control or alleviate pain of affected incised part through resting and acquiring therapeutic regimen.
Affects joints in the knees and ankles Pain occurs Gouty arthritis is a metabolic disease marked by urate crystal deposits in the joints throughout the body, causing local irritation and inflammatory responses.
e. Maintain strict bed rest for 24 hours after an attack.
Providing comfort may lessen chance of re occurrence of pain.
Source: Nursing Care Plans (Nursing Diagnosis and Intervention 6th Edition by: Gulanick/ Myers
DEPENDENT: Administer prescribed medications, which may include nonsteroidal antiinflammatory drugs, uric acid synthesis inhibitors, and uricosuric agents. Carry out new orders during rounds of physician Medication is the most important thing to be performed, to reduce or eliminate pain felt by the patient.
To perform nursing procedures that allay needs of patients
COLLABORATIVE: Maintain a safe and clean environment To promote fast recovery and comfort of patient through
rehydration and use of therapeutic regimen to uphold healing
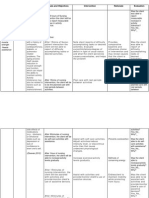
DIAGNOSIS Activity intolerance related to generalized weakness as evidenced by: Subjective Cues: Indi ko ka tarong tindog kag maghulag sing tarong kay luya akong lawas, Objective Cues: With limited ROM Unable to ambulate Body weakness noted Unable to flex and extend knees freely Decreased lower extremity strength
NEED P H Y S I O L O G I C N E E D S
DESIRED OUTCOME After 8 hours of nursing intervention, the patient will be able to:
NURSING INTERVENTIONS Independent: Assess presence of factors contributing to fatigue
RATIONALE
EVALUATION
MODIFICATION
To assess factors affecting current situation
GENERAL: Increase in activity tolerance SPECIFIC:
Assess if assistance is needed from another person Encourage active
ROM exercises
To prevent injury to patient to maintain muscle
strength and joint range of motion
Goal partially met. After 8 hours of nursing intervention, the patient was able to increase activity tolerance but still needs assistance when doing a certain task.
Body Weakness, imbalance & uncoordinated movements
assess nutritional status
adequate energy reserves
are required for activity
Ascertain ability to - Use identified stand and move techniques to enhance about and degree activity tolerance of assistance necessary
To determine current status and needs associated with participation in desired activities
Decreased activity tolerance
Assist with activities To protect patient from and injury provide/monitor clients use of assistive devices such as crutches, walker, or wheelchair
Activity Intolerance
- Report measurable increase in activity tolerance
Activity intolerance means there is insufficient physiological or psychological energy to endure or complete required or
Promote wellness To indicate the need to - Instruct client/ SO alter activity level in monitoring response to activity
- Assist patient in learning and demonstrating appropriate safety measures
To prevent injuries
desired daily activities (NANDA, 2008).
- Encourage patient to maintain positive attitude
To enhance sense of well-being
DIAGNOSIS
NEED
DESIRED OUTCOMES
INTERVENTION Independent:
RATIONALE
EVALUATION
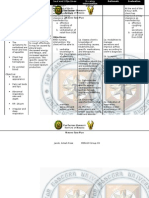
Diagnosis: Self-care deficit RT musculoskeletal impairment secondary to gouty arthritis. Subjective cues: Akong anak pa og asawa ang nagapaligo og nagabihis sa akua as verbalized by the patient.
P H Y S I O L O G I C N E E D
After 8 hours of nursing intervention: General: Provide relief and promote wellness e. Express understanding of situation and individual treatment regimen and safety measures. f. Perform PROM by flexing arms and legs and turn to sides with assistance from folks and SN. Assessed the clients activity to bathe self via direct observation using physical performance tests for ADLs
Observation of bathing performed in an atypical bathing setting may result in false date for which use of a physical performance test compensates to provide more accurate ability data. Support physical/ emotional independence.
Goal Partially Met:
e. Able to flex arms and legs as well as turn to sides with assistance from folks and SN f. Able to increase strength of affected body part through resting and acquiring therapeutic regimen.
Objective data: Inability to feed self independently Inability to dress self independently Inability to bathe and groom self independently Inability to perform toileting tasks
Maintain mobility, pain control, and exercise program. Assess barriers to participation in self-care. Identify/ plan for environmental modifications. Allow client sufficient time to complete tasks
g. Maintain or increase strength and function of affected and/or compensatory body part.
Prepares for increased independence, which enhances self-esteem. May need more time to complete tasks by self but provides an
g. Able to relax by performing deep breathing measures
independently Inability to ambulate independently
to fullest extent of ability. Capitalize on individual strengths. Taught use of adaptive bathing equipment and follow up in home. Collaborative:
opportunity for greater sense of self-confidence and self-worth. Adaptive devices extend the clients reach, increases speed and safety, and decrease exertion and reduce caregiver burden.
VS: T: 37.5C P:70 bpm R:27cpm BP:120/70 mmHg
Background knowledge: Musculoskeletal impairment Decreased strength Pain on movement Self-care deficit
Consult with rehabilitation specialists; e.g., occupational therapist.
Arrange homehealth evaluation before discharge, with follow-up afterward.
Helpful in determining assistive devices to meet individual needs; e.g., button hooks, longhandled shoehorn, reacher, hand-held shower head. Identifies problems that may be encountered because of current level of disability. Provides for more successful team efforts with others who are involved in care; e.g.,
Circumstances where individuals have failed to implement or complete
ability bathing / hygiene activities. SOURCE: Nursing Care Plans (Nursing Diagnosis and Intervention 6th Edition by: Gulanick/ Myers Arrange for consult with other agencies; e.g., Meals on wheels, home care services, nutritionist.
occupational therapist. May need additional kinds of assistance to continue in home setting.
NCLEX-RN Physiological Integrity Exam Prep :300 Practice Questions with Detailed Answers and Explanation to Master Your Exam: NCLEX-RN EXAM PREP:PRACTICE QUESTIONS AND ANSWERS, #4
1993 S C M R 603 -Competent Authority is Conferred With Discretion to Decide Whether a Departmental Inquiry Through an Inquiry Officer Was Not Necessary Such Decision is Not Controlled by Any Prerequisite or Guidelines
NCLEX-RN Physiological Integrity Exam Prep :300 Practice Questions with Detailed Answers and Explanation to Master Your Exam: NCLEX-RN EXAM PREP:PRACTICE QUESTIONS AND ANSWERS, #4
1993 S C M R 603 -Competent Authority is Conferred With Discretion to Decide Whether a Departmental Inquiry Through an Inquiry Officer Was Not Necessary Such Decision is Not Controlled by Any Prerequisite or Guidelines