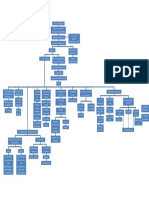
Liver Cirrhosis: A Case Study On
Liver Cirrhosis: A Case Study On
Download as docx, pdf, or txt
You might also like
- Peptic Ulcer Nursing Case StudyDocument50 pagesPeptic Ulcer Nursing Case Studygideon A. owusu100% (1)
- Case Study Liver CirrhosisDocument6 pagesCase Study Liver CirrhosisAngelica Barcelona Yumang67% (3)
- Case Study Liver CirrhosisDocument30 pagesCase Study Liver CirrhosisMarielle Soriano100% (3)
- A Case Study On Chronic Kidney DiseaseDocument103 pagesA Case Study On Chronic Kidney DiseaseLouella Mae CoraldeNo ratings yet
- 12v DC To220v Ac Inverter ReportDocument35 pages12v DC To220v Ac Inverter Reportabhishek kalshetti100% (5)
- Liver Cirrhosis Case PresentationDocument146 pagesLiver Cirrhosis Case Presentationjennachristy0395% (21)
- Case Study 10 Renal FailureDocument19 pagesCase Study 10 Renal FailureAriadne Cordelette100% (2)
- Case Study On Chronic Kidney DiseaseDocument101 pagesCase Study On Chronic Kidney DiseaseZNEROL100% (7)
- Case Study - DM II NewDocument77 pagesCase Study - DM II NewCraig MacaraigNo ratings yet
- End - Stage Renal DiseaseDocument59 pagesEnd - Stage Renal DiseaseJonathan Diaz93% (15)
- Cholecystitis Case PresDocument103 pagesCholecystitis Case PresAnton LaurencianaNo ratings yet
- Accounts Outsourcing, Outsourced Accounting and Bookkeeping ServicesDocument16 pagesAccounts Outsourcing, Outsourced Accounting and Bookkeeping ServicespoortiNo ratings yet
- My Case Study of Liver CirrhosisDocument13 pagesMy Case Study of Liver Cirrhosisdysphile100% (1)
- Chronic Kidney Disease Case PresDocument32 pagesChronic Kidney Disease Case Presnnaesor_1091No ratings yet
- LIVER CirrhosisDocument45 pagesLIVER CirrhosisBeRnAlie50% (4)
- Liver CirrhosisDocument31 pagesLiver CirrhosisAsniah Hadjiadatu Abdullah100% (1)
- Case Liver CirrhosisDocument73 pagesCase Liver CirrhosisJesus Orita-Delima100% (1)
- Case Study On Alcoholic Liver DiseaseDocument24 pagesCase Study On Alcoholic Liver DiseaseKristine Alejandro100% (5)
- Liver Cirrhosis CaseDocument8 pagesLiver Cirrhosis Casemarlx5No ratings yet
- Acute Renal FailureDocument54 pagesAcute Renal FailureNiala Almario100% (1)
- Case Study CholelithiasisDocument14 pagesCase Study Cholelithiasisb_faye20No ratings yet
- Liver CirrhosisDocument76 pagesLiver Cirrhosiskathy100% (2)
- Pathophysiology in Liver CirrhosisDocument4 pagesPathophysiology in Liver CirrhosisCyrus Ortalla RobinNo ratings yet
- Liver CirrhosisDocument5 pagesLiver CirrhosisRLLTNo ratings yet
- Hypertension CP FinaleeDocument76 pagesHypertension CP FinaleeIsabella Marie PanNo ratings yet
- Case Study Liver CirrhosisDocument20 pagesCase Study Liver CirrhosisFate ZephyrNo ratings yet
- Liver Cirrhosis: Review HepatologyDocument71 pagesLiver Cirrhosis: Review HepatologyAstri Arri FebriantiNo ratings yet
- Group Final CP - Liver AbscessDocument41 pagesGroup Final CP - Liver AbscessMaricel Sangual Dubal100% (1)
- Chronic Kidney Disease Case PresentationDocument14 pagesChronic Kidney Disease Case Presentationnnaesor_109150% (2)
- Nursing Upper Gi BleedingDocument23 pagesNursing Upper Gi BleedingLord Pozak Miller100% (3)
- Chronic Renal FailureDocument37 pagesChronic Renal Failuredorkiebaby100% (10)
- A Case Study On Chronic Renal DiseaseDocument17 pagesA Case Study On Chronic Renal Diseasematucojulio100% (1)
- Case Study - Septic ShockDocument16 pagesCase Study - Septic ShockIrene Mae Villanueva Ariola100% (2)
- Chronic Kidney Disease CompilationDocument33 pagesChronic Kidney Disease CompilationGwen Stefanie Lagrimas ValloyasNo ratings yet
- GlomerulonephritisDocument8 pagesGlomerulonephritisMatthew Ryan100% (1)
- Liver Cirrhosis PathophysiologyDocument1 pageLiver Cirrhosis PathophysiologyCaren ReyesNo ratings yet
- Final CholelithiasisDocument36 pagesFinal CholelithiasisRalph Pelegrino100% (2)
- ESRD Secondary To Diabetic Nephropathy CASE STUDY Docx 2Document42 pagesESRD Secondary To Diabetic Nephropathy CASE STUDY Docx 2Eyerusalem100% (1)
- CHOLELITHIASISDocument46 pagesCHOLELITHIASIShttp_ugly88% (8)
- Case Analysis FinalDocument29 pagesCase Analysis FinalVeyNo ratings yet
- Pa Tho Physiology of Liver Cirrhosis - MercyDocument7 pagesPa Tho Physiology of Liver Cirrhosis - Mercymersenie_TheovercomerNo ratings yet
- CASE STUDY ON ACUTE Renal FailureDocument38 pagesCASE STUDY ON ACUTE Renal FailureOdey Godwin100% (1)
- Case Study On AppendicitisDocument15 pagesCase Study On AppendicitisKristelle BonitaNo ratings yet
- CP - Liver CirrhosisDocument161 pagesCP - Liver CirrhosisRomeo ReyesNo ratings yet
- Case Study StrokeDocument40 pagesCase Study Strokeymonn100% (1)
- Case Study On Alcoholic Liver DiseaseDocument20 pagesCase Study On Alcoholic Liver DiseaseHomework PingNo ratings yet
- A Review: Nutrition in Chronic Kidney Disease PatientsDocument13 pagesA Review: Nutrition in Chronic Kidney Disease Patientsscience worldNo ratings yet
- Acute Glomerulonephritis Case StudyDocument12 pagesAcute Glomerulonephritis Case Study19lyon92100% (6)
- Case StudyDocument7 pagesCase StudyMicah Jonah ElicañoNo ratings yet
- Alcoholic Liver DiseaseDocument70 pagesAlcoholic Liver Diseaseaannaass nNo ratings yet
- Laennecs Cirrhosis PathophysiologyDocument2 pagesLaennecs Cirrhosis PathophysiologyTrixie Al Marie100% (3)
- Complete Care Study, AppendicitisDocument50 pagesComplete Care Study, AppendicitisOjo Paul Adesina100% (1)
- Case StudyDocument18 pagesCase StudyJerome GonezNo ratings yet
- Cholelithiasis: - Other Names: - Gallbladder Attack - Biliary Colic - Gallstone Attack - Bile Calculus - Biliary CalculusDocument101 pagesCholelithiasis: - Other Names: - Gallbladder Attack - Biliary Colic - Gallstone Attack - Bile Calculus - Biliary CalculusYvonne100% (1)
- Chronic Kidney Disease Case StudyDocument96 pagesChronic Kidney Disease Case StudyJUDE ARIZALA100% (1)
- Cirrhosis of LiverDocument7 pagesCirrhosis of LivermOHAN.S100% (3)
- Liver Cirrhosis - NCPDocument18 pagesLiver Cirrhosis - NCPIshmael Solamillo83% (6)
- Cholelithiasis Case PresentationDocument25 pagesCholelithiasis Case PresentationMarcos AquinoNo ratings yet
- Community Acquired Pneumonia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandCommunity Acquired Pneumonia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Brief Background of The Disease: Liver CirrhosisDocument7 pagesBrief Background of The Disease: Liver CirrhosisLyra Lustre RNNo ratings yet
- Cirrhosis Description Highlights Causes of CirrhosisDocument18 pagesCirrhosis Description Highlights Causes of Cirrhosisen-oleNo ratings yet
- Metabolism and EndocrineDocument156 pagesMetabolism and EndocrineGren May Angeli MagsakayNo ratings yet
- Discharge PlanDocument2 pagesDischarge PlanCharmaine del Rosario100% (1)
- Patient'S Profile Patient's Initials: Age: Birth Date: Gender: Civil Status: Religion: AddressDocument8 pagesPatient'S Profile Patient's Initials: Age: Birth Date: Gender: Civil Status: Religion: AddressCharmaine del RosarioNo ratings yet
- An Inflammation Anywhere Along The ALIMETARY TRACT in All Layers, Intestinal Wall, Lymph Nodes and MesenteryDocument23 pagesAn Inflammation Anywhere Along The ALIMETARY TRACT in All Layers, Intestinal Wall, Lymph Nodes and MesenteryCharmaine del RosarioNo ratings yet
- Emonc Protocol (Philhealth-DOH)Document38 pagesEmonc Protocol (Philhealth-DOH)Sandra BaileyNo ratings yet
- Case Study HemodialysisDocument5 pagesCase Study HemodialysisCharmaine del RosarioNo ratings yet
- Polytechnic University of The Philippines 115 Founding Anniversary Academic Contests CommitteeDocument2 pagesPolytechnic University of The Philippines 115 Founding Anniversary Academic Contests CommitteeRomeo Castro De GuzmanNo ratings yet
- YatishDocument1 pageYatishSumanth Jm Sumanth JmNo ratings yet
- Cookery 9 Quarter 3Document33 pagesCookery 9 Quarter 3John Michael ItableNo ratings yet
- Garua - Partitura PDFDocument6 pagesGarua - Partitura PDFJavier Salnisky MusicoNo ratings yet
- Uthama VillainDocument3 pagesUthama Villainubabmar321No ratings yet
- Get Started: Jeff BezosDocument3 pagesGet Started: Jeff BezosVrutika Shah (207050592001)No ratings yet
- Unit Number: 1 Beach Road Traffic NightmareDocument1 pageUnit Number: 1 Beach Road Traffic NightmareSami Khan Kohati100% (1)
- Binomial and Poisson DistributionDocument26 pagesBinomial and Poisson Distributionmahnoorjamali853No ratings yet
- D4503Document4 pagesD4503EmilNo ratings yet
- BMW Installation Instructions - Rear Footrests - 02.2021Document7 pagesBMW Installation Instructions - Rear Footrests - 02.2021aviaqualNo ratings yet
- Topic 2 Financial Statements of Limited CompaniesDocument17 pagesTopic 2 Financial Statements of Limited CompaniesThorapioMayNo ratings yet
- Simulation and Dissimulation by Francis BaconDocument7 pagesSimulation and Dissimulation by Francis BaconAnum Mubashar100% (1)
- Information Technology BasicsDocument32 pagesInformation Technology BasicsM. O. Adan94% (18)
- Mir For Aluminium LadderDocument13 pagesMir For Aluminium LadderRoshan George PhilipNo ratings yet
- Materials Quiz and Properties WorksheetDocument4 pagesMaterials Quiz and Properties WorksheetSamantha AshmanNo ratings yet
- Marketing - Module 8 The Marketing Mix - PLACEDocument10 pagesMarketing - Module 8 The Marketing Mix - PLACEKJ JonesNo ratings yet
- Andrew Jackson Essay ThesisDocument8 pagesAndrew Jackson Essay Thesisggzgpeikd100% (1)
- 09 Sperre Pleat Coolers Technical DocumentationDocument18 pages09 Sperre Pleat Coolers Technical DocumentationJohanNo ratings yet
- List of Head Hunters and Job Website in VietnamDocument11 pagesList of Head Hunters and Job Website in VietnamNguyen Hoa0% (1)
- Project Word FileDocument63 pagesProject Word Fileanon_965191473No ratings yet
- Medical ManualDocument144 pagesMedical ManualDevinder Singh50% (2)
- Depresión 5Document24 pagesDepresión 5Luz Maria RojasNo ratings yet
- Borg-Laufs - 2013 - Basic Psychological Needs in Childhood and AdolescDocument11 pagesBorg-Laufs - 2013 - Basic Psychological Needs in Childhood and AdolescZynen BanielNo ratings yet
- CO MonstersDocument177 pagesCO MonstersMatthew McMillanNo ratings yet
- Deblurring Images, Matrices, Spectra, and Filtering (Fundamentals of Algorithms)Document145 pagesDeblurring Images, Matrices, Spectra, and Filtering (Fundamentals of Algorithms)Zengben HaoNo ratings yet
- Jesus Christ The Son of Mary: and His Most Blessed MotherDocument36 pagesJesus Christ The Son of Mary: and His Most Blessed MotherTyba314No ratings yet
- Drying of Malaysian Capsicum Annuum L. (Red Chili) Dried by Open and Solar DryingDocument11 pagesDrying of Malaysian Capsicum Annuum L. (Red Chili) Dried by Open and Solar DryingZulhambri ZulNo ratings yet
- Gender and Equality Towards Policy Enhancement A Phenomenological InquiryDocument8 pagesGender and Equality Towards Policy Enhancement A Phenomenological InquiryIOER International Multidisciplinary Research Journal ( IIMRJ)No ratings yet