10 Peri Arrest Arrhythmias
10 Peri Arrest Arrhythmias
Download as pdf or txt
You might also like
- 640aebf9db70b Test Bank For Applied Pathophysiology A Conceptual Approach 4th Edition by Judi Nath Carie Braun-14Document1 page640aebf9db70b Test Bank For Applied Pathophysiology A Conceptual Approach 4th Edition by Judi Nath Carie Braun-14splashnet42No ratings yet
- Sim LabDocument4 pagesSim Laballycat2390% (10)
- Med Surg Notes 3Document6 pagesMed Surg Notes 3Ivy NguyenNo ratings yet
- 100 ECG For AKP - With AnswersDocument102 pages100 ECG For AKP - With AnswersaeyousefNo ratings yet
- Test Questions From Barbara K. TimbyDocument5 pagesTest Questions From Barbara K. Timbysuperrhengc0% (1)
- OT6 - Valsalva ManeuverDocument7 pagesOT6 - Valsalva ManeuverAnnbe BarteNo ratings yet
- Ati PN Maternal Newborn Proctored ExamDocument6 pagesAti PN Maternal Newborn Proctored ExamkapedispursNo ratings yet
- Arrhythmia (Irregular Heartbeats) Symptoms, Types, and TreatmentDocument5 pagesArrhythmia (Irregular Heartbeats) Symptoms, Types, and TreatmentCyberMeow100% (1)
- Chest Tubes: From Indication To RemovalDocument49 pagesChest Tubes: From Indication To Removaldara octavianiNo ratings yet
- Multi SistemDocument19 pagesMulti SistemciptaarynNo ratings yet
- 150+ Cases in Chest XrayDocument21 pages150+ Cases in Chest XrayMuntadher KareemNo ratings yet
- NCLEX Pregnancy NotesDocument3 pagesNCLEX Pregnancy NotesrustiejadeNo ratings yet
- Carotid Sinus MassageDocument4 pagesCarotid Sinus MassageChalikias GeorgeNo ratings yet
- 56: Neurological System: Practice QuestionsDocument36 pages56: Neurological System: Practice Questionsjutah2013No ratings yet
- Pathophysiology Practice QuestionsDocument4 pagesPathophysiology Practice QuestionsMuhammad AdilNo ratings yet
- Chess Program Operation MastermindDocument4 pagesChess Program Operation MastermindDoneil JonesNo ratings yet
- Agents Used in Cardiac ArrhythmiasDocument4 pagesAgents Used in Cardiac ArrhythmiasKaye PatriaNo ratings yet
- Lowdermilk: Maternity & Women's Health Care, 10th EditionDocument12 pagesLowdermilk: Maternity & Women's Health Care, 10th Editionvanassa johnson100% (1)
- Peds Med Math ReviewDocument20 pagesPeds Med Math ReviewStephania VlachosNo ratings yet
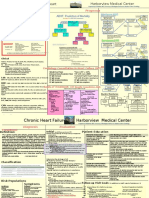
- Heart Failure Express Card HMCDocument2 pagesHeart Failure Express Card HMCalexNo ratings yet
- Dimensional Analysis (08.14.19 Draft)Document6 pagesDimensional Analysis (08.14.19 Draft)TheresaNo ratings yet
- S2 Retake Practice Exam PDFDocument3 pagesS2 Retake Practice Exam PDFWinnie MeiNo ratings yet
- Chapter 011Document13 pagesChapter 011dtheart2821100% (2)
- 1804Document29 pages1804insan fitriyaniNo ratings yet
- Pediatric Medication Math Review Jan 2011Document7 pagesPediatric Medication Math Review Jan 2011Tyrone Kent HalogNo ratings yet
- PDF Health Promotion Throughout The Life Span 9th Edition Edelman Test Bank DownloadDocument34 pagesPDF Health Promotion Throughout The Life Span 9th Edition Edelman Test Bank Downloadkeanenplewa100% (3)
- Ch5 Integumentary SystemDocument31 pagesCh5 Integumentary Systemİsmail ŞimşekNo ratings yet
- NCLEX Categories Study GuideDocument9 pagesNCLEX Categories Study GuideTanya ViarsNo ratings yet
- Pharmacology NCLEX QuestionsDocument26 pagesPharmacology NCLEX QuestionsbenasmwangiNo ratings yet
- Test Bank For Saunders Comprehensive Review For The NCLEX-RN Examination, 7th Edition, Linda Anne Silvestri, All Chapter Instant DownloadDocument45 pagesTest Bank For Saunders Comprehensive Review For The NCLEX-RN Examination, 7th Edition, Linda Anne Silvestri, All Chapter Instant Downloadruzanekrukar100% (6)
- Master Player ReflectionDocument9 pagesMaster Player ReflectionEddie Resurreccion Jr.No ratings yet
- HESI List Fro Pharmacology TestDocument1 pageHESI List Fro Pharmacology TestnanaNo ratings yet
- ATI Mastery ReviewDocument8 pagesATI Mastery ReviewJohn MixerNo ratings yet
- Icu 1Document3 pagesIcu 1Jillian EsquivelNo ratings yet
- Pharmacology Drug Dosage CalculationsDocument54 pagesPharmacology Drug Dosage CalculationsMichelle FigueroaNo ratings yet
- Care of Patients With Cardiac DisordersDocument4 pagesCare of Patients With Cardiac Disordersbugoff700No ratings yet
- Nclex Review PointersDocument4 pagesNclex Review PointersFaith VaughnNo ratings yet
- Exam ReviewDocument4 pagesExam ReviewMya Thomas100% (1)
- Myocardial Infarction NCLEX AnswersDocument4 pagesMyocardial Infarction NCLEX AnswersKariza VillarNo ratings yet
- NCLEX Review Cardiovascular QuizDocument17 pagesNCLEX Review Cardiovascular Quizdany tesemaNo ratings yet
- IV A.medical ManagementDocument9 pagesIV A.medical ManagementbeingfiredNo ratings yet
- Burns: TEST I - Foundation of Professional Nursing PracticeDocument9 pagesBurns: TEST I - Foundation of Professional Nursing PracticeMc SuanNo ratings yet
- NURS 460 Nursing Licensure Examination Course: Jv7@hawaii - EduDocument5 pagesNURS 460 Nursing Licensure Examination Course: Jv7@hawaii - EduJeffrey ViernesNo ratings yet
- Chess Mentor 3Document4 pagesChess Mentor 3Koki Mostafa0% (1)
- ATI Bible 1Document205 pagesATI Bible 1surviving nursing school100% (1)
- UntitledDocument41 pagesUntitledvioletdeocaresNo ratings yet
- Community Health AtiDocument4 pagesCommunity Health Atiapi-243590841No ratings yet
- Peds ?Document51 pagesPeds ?gissy0522No ratings yet
- Unlike False LaborDocument29 pagesUnlike False LaborMEi .. ÜNo ratings yet
- Care of The Patient With A Cardiac Mechanical DisorderDocument8 pagesCare of The Patient With A Cardiac Mechanical DisorderthubtendrolmaNo ratings yet
- Test For Autonomic NeuropathyDocument31 pagesTest For Autonomic NeuropathysrinidhiNo ratings yet
- Correct Answer: 4. Premedicate The Client With An Analgesic Before AmbulatingDocument49 pagesCorrect Answer: 4. Premedicate The Client With An Analgesic Before AmbulatingPortage ExamsNo ratings yet
- Unit 1 Definitions/key Terms Varcarolis Mental Health NursingDocument6 pagesUnit 1 Definitions/key Terms Varcarolis Mental Health Nursingatl_nurse_studentNo ratings yet
- Q&a 1Document19 pagesQ&a 1api-3818438No ratings yet
- Infection Control For NclexDocument9 pagesInfection Control For NclexMadora SamuelNo ratings yet
- Answers, Rationales, and Test Taking Strategies: Managing Care Quality and SafetyDocument14 pagesAnswers, Rationales, and Test Taking Strategies: Managing Care Quality and SafetyNursyNurseNo ratings yet
- Philosophy of NursingDocument8 pagesPhilosophy of Nursingapi-430575435No ratings yet
- 160 Chess Puzzles in Two Moves, Part 5: Winning Chess ExerciseFrom Everand160 Chess Puzzles in Two Moves, Part 5: Winning Chess ExerciseNo ratings yet
- 160 Chess Puzzles in Two Moves, Part 4: Winning Chess ExerciseFrom Everand160 Chess Puzzles in Two Moves, Part 4: Winning Chess ExerciseNo ratings yet
- U.M.F. "Gr. T. Popa" Ia Ş IDocument37 pagesU.M.F. "Gr. T. Popa" Ia Ş Ij.doe.hex_87No ratings yet
- Megacode 4Document4 pagesMegacode 4JILL ANGELESNo ratings yet
- Raminder Nirula - High-Yield Internal Medicine (High-Yield Series) - Lippincott Williams and Wilkins (2006)Document228 pagesRaminder Nirula - High-Yield Internal Medicine (High-Yield Series) - Lippincott Williams and Wilkins (2006)Isah Mohammed100% (1)
- Logbook Ecg Dokter Mudafakultas Kedokteran Universitas Hang Tuah KSM Jantung Rsud Dr. Mohamad Soewandhie PERIODE: - NAMA: Atinul Kulsum (20190420059)Document3 pagesLogbook Ecg Dokter Mudafakultas Kedokteran Universitas Hang Tuah KSM Jantung Rsud Dr. Mohamad Soewandhie PERIODE: - NAMA: Atinul Kulsum (20190420059)Atinul KulsumNo ratings yet
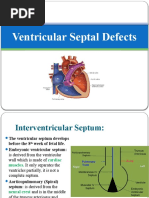
- Ventricular Septal DefectDocument43 pagesVentricular Septal DefectmalekNo ratings yet
- Chapter 33 - PalpitationDocument9 pagesChapter 33 - Palpitationjonalyn.mejellanoNo ratings yet
- Dyandev Patade HolterDocument20 pagesDyandev Patade HolterRunway CafeNo ratings yet
- Download Full The EHRA Book of Interventional Electrophysiology: Case-based learning with multiple choice questions 1st Edition Hein Heidbuchel PDF All ChaptersDocument62 pagesDownload Full The EHRA Book of Interventional Electrophysiology: Case-based learning with multiple choice questions 1st Edition Hein Heidbuchel PDF All Chapterstagangxhambo100% (4)
- STUDOCU Heart Failure-Internal-Medicine-Harrison-Edition-2019Document12 pagesSTUDOCU Heart Failure-Internal-Medicine-Harrison-Edition-2019ScribdTranslationsNo ratings yet
- Tetralogy of FallotDocument5 pagesTetralogy of FallotYusnida RahmawatiNo ratings yet
- Complete Download Simplified Interpretation of Pacemaker ECGs An Introduction 1st Edition Aaron B. Hesselson PDF All ChaptersDocument60 pagesComplete Download Simplified Interpretation of Pacemaker ECGs An Introduction 1st Edition Aaron B. Hesselson PDF All Chaptersendjohirsti100% (8)
- ESC Congress 2020: The Digital ExperienceDocument9 pagesESC Congress 2020: The Digital ExperienceMeatus AcusticusNo ratings yet
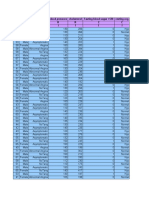
- Age Sex Chest Pain Type Blood Pressure Cholesterol Fasting Blood Sugar 120 Resting Ecg R C C R R C C I I I I I I IDocument14 pagesAge Sex Chest Pain Type Blood Pressure Cholesterol Fasting Blood Sugar 120 Resting Ecg R C C R R C C I I I I I I Isantu4_1111No ratings yet
- CVS 1700 Sush Unity PDFDocument158 pagesCVS 1700 Sush Unity PDFBio DataNo ratings yet
- Electrocardiogram NotesDocument13 pagesElectrocardiogram NotesRomeo Cordova Jr.No ratings yet
- Curofy Best ECG CasesDocument26 pagesCurofy Best ECG Casescnshariff@gmail.comNo ratings yet
- Cardiovascular Disorders: Prepared By: Wad-Ey, Rosie Glae, RNDocument49 pagesCardiovascular Disorders: Prepared By: Wad-Ey, Rosie Glae, RNrosieglaeNo ratings yet
- LA Cardiac Arythmia - 0Document61 pagesLA Cardiac Arythmia - 0Karthik SNo ratings yet
- Arrhythmias Types, Pathophysiology AtfDocument9 pagesArrhythmias Types, Pathophysiology AtfAmir mohammad moori MohammadiNo ratings yet
- Presentation, Symptoms and Signs of Heart Failure: What Will I Learn?Document5 pagesPresentation, Symptoms and Signs of Heart Failure: What Will I Learn?Vidini Kusuma AjiNo ratings yet
- Cardiac Dysrhythmias ExamDocument4 pagesCardiac Dysrhythmias Exambobtaguba100% (3)
- 3D Mapping Expert Consensus JoADocument34 pages3D Mapping Expert Consensus JoAFikriYTNo ratings yet
- NCM 118 - Lesson 11 (Arrhythmia)Document5 pagesNCM 118 - Lesson 11 (Arrhythmia)Bobby Christian DuronNo ratings yet
- Heart Failure With Preserved Ejection FractionDocument27 pagesHeart Failure With Preserved Ejection FractionMega Almira100% (1)
- Takotsubo Cardiomyopathy and The Hope of Specific Biomarker: EditorialDocument2 pagesTakotsubo Cardiomyopathy and The Hope of Specific Biomarker: Editorialyunita putriNo ratings yet
- Dilated CardiomyopathyDocument23 pagesDilated CardiomyopathyYanna Habib-MangotaraNo ratings yet
- Valvular Heart DiseaseDocument10 pagesValvular Heart DiseaseEzyan SyaminNo ratings yet
- Pathophysiology of Congestive Heart FailureDocument3 pagesPathophysiology of Congestive Heart FailureMel Izhra N. MargateNo ratings yet
- Fibrinolitik UnsratDocument7 pagesFibrinolitik UnsratOtherside OfmeNo ratings yet
- Sgarbossa CrtiteriaDocument4 pagesSgarbossa Crtiteriaanisah astiraniNo ratings yet