1 s2.0 S0264410X1501470X Main
1 s2.0 S0264410X1501470X Main
Download as pdf or txt
You might also like
- WHO-PPL-Short Summary 25Feb-ET NM WHO PDFDocument7 pagesWHO-PPL-Short Summary 25Feb-ET NM WHO PDFRichard Caceda VizcondeNo ratings yet
- Nursing DelegationDocument4 pagesNursing Delegationarielsinco100% (1)
- Pathogens 11 01248Document13 pagesPathogens 11 01248Ngọc Minh Anh NguyễnNo ratings yet
- 2009guzman BlancoDocument5 pages2009guzman BlancoLuís Flávio Cozza VazNo ratings yet
- September CDC HAISDocument11 pagesSeptember CDC HAISnoval firdausNo ratings yet
- CDC Activities Initiatives For COVID 19 ResponseDocument60 pagesCDC Activities Initiatives For COVID 19 ResponseCNBC.com87% (23)
- J Rheumatol 2021 Jun 15 Fernandez-Avila DGDocument7 pagesJ Rheumatol 2021 Jun 15 Fernandez-Avila DGFernando SousaNo ratings yet
- WHO Policy Development Processes For A New Vaccine: Case Study of Malaria VaccinesDocument11 pagesWHO Policy Development Processes For A New Vaccine: Case Study of Malaria VaccinesAndi Dirhan TNo ratings yet
- Overview of Public Health Microbiology LaboratoryDocument10 pagesOverview of Public Health Microbiology LaboratoryedwineiouNo ratings yet
- Prevention of Gastric CancerDocument2 pagesPrevention of Gastric CancerAndhika Bintang MahardhikaNo ratings yet
- Antimicrobial UseDocument6 pagesAntimicrobial Usemaddy.nestebyNo ratings yet
- Current Issue DiseasesDocument14 pagesCurrent Issue Diseaseshye jinNo ratings yet
- 7057 24972 1 PBDocument133 pages7057 24972 1 PBDen NisNo ratings yet
- MN Zava 2014Document5 pagesMN Zava 2014ibrahima1968No ratings yet
- Standard Operating Procedure For ControlDocument31 pagesStandard Operating Procedure For ControlRizky PrakasaNo ratings yet
- CXG_096eDocument20 pagesCXG_096epphat8585No ratings yet
- Importance Surveillance and DetectionDocument6 pagesImportance Surveillance and Detectionsherog ahmedNo ratings yet
- Malaria Control ProgramDocument74 pagesMalaria Control ProgramMary Ruth Aujero Sanchez-Benzon100% (1)
- cdc_100571_DS1Document8 pagescdc_100571_DS15prwfqfqbmNo ratings yet
- Vaccines 12 00184Document10 pagesVaccines 12 00184Sabrina DescalzotaNo ratings yet
- Ch6 19rareDocument4 pagesCh6 19rareArmin BiparvaNo ratings yet
- 1-Introduction To PH EpidemiologyDocument33 pages1-Introduction To PH Epidemiologyrabiashoukat7888No ratings yet
- Analysis of Potential Impact of COVID-19 On Molecular Testing For Infectious Diseases MarketDocument3 pagesAnalysis of Potential Impact of COVID-19 On Molecular Testing For Infectious Diseases MarketPavan GongaleNo ratings yet
- Biological DiseasesDocument3 pagesBiological DiseasesWZ HakimNo ratings yet
- JCT 2013102511342874Document8 pagesJCT 2013102511342874RiestaKierantiNo ratings yet
- Risk of Tuberculosis Infection Among Community Health AgentsDocument6 pagesRisk of Tuberculosis Infection Among Community Health AgentsLuciana SaundersNo ratings yet
- Centers For Disease Control and Prevention's Sexually Transmitted Diseases Infection GuidelinesDocument6 pagesCenters For Disease Control and Prevention's Sexually Transmitted Diseases Infection GuidelinesabhinavrautNo ratings yet
- Propsal on Knowledge and Attitude on Hepatitis B Among Market Women in Gomoa Fetteh.Document5 pagesPropsal on Knowledge and Attitude on Hepatitis B Among Market Women in Gomoa Fetteh.emmanuelkwesizodiac1No ratings yet
- Machine Learning Model For Predicting Malaria Using Clinical Information.Document14 pagesMachine Learning Model For Predicting Malaria Using Clinical Information.xiongmao2389No ratings yet
- Developing The Next Generation of VaccinologistsDocument2 pagesDeveloping The Next Generation of VaccinologistsSukma DewiNo ratings yet
- vaccines-09-00084Document15 pagesvaccines-09-00084v2104161No ratings yet
- rr6202 PDFDocument32 pagesrr6202 PDFssami670No ratings yet
- Application of Traditional Vaccine Development Strategies To Sars-Cov-2Document41 pagesApplication of Traditional Vaccine Development Strategies To Sars-Cov-2DheerajNo ratings yet
- Enhancing Global Security Through Infectious Disease Threat ReductionDocument15 pagesEnhancing Global Security Through Infectious Disease Threat ReductionWai AbrahamNo ratings yet
- Staffing - Overview of Infection Prevention Programs - Table of Contents - APICDocument27 pagesStaffing - Overview of Infection Prevention Programs - Table of Contents - APICBassem DanielNo ratings yet
- Importance of Research Public HealthDocument12 pagesImportance of Research Public HealthConcepcion MpsNo ratings yet
- ICMR COVID 19 Call For Proposals V1Document5 pagesICMR COVID 19 Call For Proposals V1Rishabh AgarwalNo ratings yet
- 参考文献-宋老师推荐的作图风格3Document9 pages参考文献-宋老师推荐的作图风格315035689055liuhaiyangNo ratings yet
- MMWR HiB PDFDocument20 pagesMMWR HiB PDFworksheetbookNo ratings yet
- Prevention and Containment of Antimicrobial Resistance: Sixty-Third Session Bangkok, Thailand 7-10 September 2010Document17 pagesPrevention and Containment of Antimicrobial Resistance: Sixty-Third Session Bangkok, Thailand 7-10 September 2010gabriela_mariangela5929No ratings yet
- Roush Vaccine 2007Document9 pagesRoush Vaccine 2007YLNZNo ratings yet
- Gloves for COVID-19_ a Living Systematic ReviewDocument14 pagesGloves for COVID-19_ a Living Systematic ReviewAzucena Santillán GarcíaNo ratings yet
- Artigo Sobre AidsDocument7 pagesArtigo Sobre AidscamilatututNo ratings yet
- Patient Centred Surveillance of Drug Resistant PathogensDocument19 pagesPatient Centred Surveillance of Drug Resistant PathogensHanna alexanderNo ratings yet
- 2 SchistoDocument3 pages2 Schistoapi-281306164No ratings yet
- Healthcare: A Systematic Review of Healthcare-Associated Infectious Organisms in Medical Radiation Science DepartmentsDocument14 pagesHealthcare: A Systematic Review of Healthcare-Associated Infectious Organisms in Medical Radiation Science DepartmentsArina Al-KhaqNo ratings yet
- Med 1Document1 pageMed 1Roy Vincent OtienoNo ratings yet
- Standardization of Minimally Invasive Tissue Sampling Specimen Collection and Pathology Training For The Child Health and Mortality Prevention Surveillance NetworkDocument13 pagesStandardization of Minimally Invasive Tissue Sampling Specimen Collection and Pathology Training For The Child Health and Mortality Prevention Surveillance NetworkgranasamsaNo ratings yet
- A2 ModelosCOVID19Mariel22 Lerma12314Document8 pagesA2 ModelosCOVID19Mariel22 Lerma12314ALETA44No ratings yet
- World Health Organization: WHO/EMC/BAC/98.6Document5 pagesWorld Health Organization: WHO/EMC/BAC/98.6gabriela_mariangela5929No ratings yet
- SurvDocument17 pagesSurvligech195No ratings yet
- DownloadDocument14 pagesDownloadRenan de LimaNo ratings yet
- Chelsey (Chapter 2 RRL) LocalDocument3 pagesChelsey (Chapter 2 RRL) LocalChester ArenasNo ratings yet
- Cost Effectiveness of A Care Program For HIV AIDS Patients - 2016 - Value in HeDocument8 pagesCost Effectiveness of A Care Program For HIV AIDS Patients - 2016 - Value in HeSansa LauraNo ratings yet
- Uk Views On Priority Programmes For Promoting Capacity Building For Surveillance, Detection, Diagnosis and Containment of Infectious DiseasesDocument7 pagesUk Views On Priority Programmes For Promoting Capacity Building For Surveillance, Detection, Diagnosis and Containment of Infectious DiseasesDante DamiánNo ratings yet
- The Vaccine Handbook: A Practical Guide for Clinicians, Twelfth EditionFrom EverandThe Vaccine Handbook: A Practical Guide for Clinicians, Twelfth EditionNo ratings yet
- Hepatocellular Carcinoma: Translational Precision Medicine ApproachesFrom EverandHepatocellular Carcinoma: Translational Precision Medicine ApproachesYujin HoshidaNo ratings yet
- Understanding Multiple Myeloma: Recent Findings and Laboratory Investigation Updates for Biomedical Scientists: Continuing Professional Development in Pathology For Medical Laboratory ProfessionalsFrom EverandUnderstanding Multiple Myeloma: Recent Findings and Laboratory Investigation Updates for Biomedical Scientists: Continuing Professional Development in Pathology For Medical Laboratory ProfessionalsNo ratings yet
- Virologic Failure in HIV: An Updated Clinician’s Guide to Assessment and ManagementFrom EverandVirologic Failure in HIV: An Updated Clinician’s Guide to Assessment and ManagementNo ratings yet
- MJDF October 2017 New Questions & FeedbackDocument2 pagesMJDF October 2017 New Questions & Feedbacksajna1980No ratings yet
- English Asi PDFDocument3 pagesEnglish Asi PDFrujaklutisNo ratings yet
- 2018 Biotech Primer WEEKLY CompendiumDocument120 pages2018 Biotech Primer WEEKLY CompendiumAxelNo ratings yet
- Medicines in Health Systems Working Toward UHC: Presentation ScriptDocument21 pagesMedicines in Health Systems Working Toward UHC: Presentation ScriptHananAhmedNo ratings yet
- DME Assam Recruitment NoticeDocument2 pagesDME Assam Recruitment NoticekusharypragyaNo ratings yet
- STD TestsDocument1 pageSTD TestsSTDTestingNo ratings yet
- Foreword: A World-Class ICU OpensDocument6 pagesForeword: A World-Class ICU OpensAsiimwe ColinNo ratings yet
- MUNICIPALITY OF BUENAVISTABohol, PhilippinesSituational Analysis and SWOT AnalysisStakeholder Analysis With Strategic PlanCase Study With Preventive Action PlanDocument36 pagesMUNICIPALITY OF BUENAVISTABohol, PhilippinesSituational Analysis and SWOT AnalysisStakeholder Analysis With Strategic PlanCase Study With Preventive Action PlanMark Johnuel Duavis100% (1)
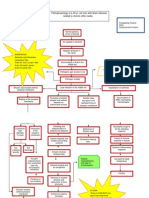
- Pathophysiology of Brain Abscess Secondary To Chronic Otitis MediaDocument5 pagesPathophysiology of Brain Abscess Secondary To Chronic Otitis Mediafufulabrador100% (1)
- RPM Employee Benefitguide 2023Document16 pagesRPM Employee Benefitguide 2023kcrow.bizNo ratings yet
- Data-Driven Wound Care A Business and Clinical OpportunityDocument18 pagesData-Driven Wound Care A Business and Clinical OpportunityBob RiouxNo ratings yet
- Heinert CVDocument9 pagesHeinert CVapi-608513468No ratings yet
- Form FDocument2 pagesForm FAnand Chiney100% (2)
- Godavari College of Nursing, Jalgaon: Daily Clinical Dairy ReportDocument6 pagesGodavari College of Nursing, Jalgaon: Daily Clinical Dairy ReportbuntyNo ratings yet
- Lecture 19 - AnticoagulantsDocument43 pagesLecture 19 - Anticoagulantsapi-3703352100% (1)
- Help With Health Costs: Can You Get Help With The Cost ofDocument42 pagesHelp With Health Costs: Can You Get Help With The Cost ofkhlodiaNo ratings yet
- 3864 11520 1 PBDocument22 pages3864 11520 1 PBaulia maharaniNo ratings yet
- Dissertation Topics in Rajiv Gandhi University of Health SciencesDocument7 pagesDissertation Topics in Rajiv Gandhi University of Health SciencesWhereCanIFindSomeoneToWriteMyPaperNewarkNo ratings yet
- MDV 161Document12 pagesMDV 161rasika bhatNo ratings yet
- Kajian Hukum Peran "Apoteker" Dalam Saintifikasi JamuDocument6 pagesKajian Hukum Peran "Apoteker" Dalam Saintifikasi JamuPetrisyia ReyvhonniNo ratings yet
- Week 10 - PHAR1006 Calculations - 2024 - wANSWERSDocument23 pagesWeek 10 - PHAR1006 Calculations - 2024 - wANSWERSvicrobalmarieNo ratings yet
- Collection of Soiled Contaminated &transporting Handling of EqupmentDocument3 pagesCollection of Soiled Contaminated &transporting Handling of EqupmentRAZNAS ASLAM A KNo ratings yet
- AntiBiotic Medicine by AdEel-SaiMDocument21 pagesAntiBiotic Medicine by AdEel-SaiMAdeel ur RahmanNo ratings yet
- Full Download Fuhrman & Zimmerman's Pediatric Critical Care 6th Edition Jerry J. Zimmerman PDFDocument64 pagesFull Download Fuhrman & Zimmerman's Pediatric Critical Care 6th Edition Jerry J. Zimmerman PDFdmalexuquete100% (4)
- Chicken Pox - NCPDocument2 pagesChicken Pox - NCPMaria Kyla VicenteNo ratings yet
- Shivanee Sathia ResumeDocument3 pagesShivanee Sathia Resumeapi-456295176No ratings yet
- Manifestasi Klinis, Pencegahan, PengendalianDocument34 pagesManifestasi Klinis, Pencegahan, PengendalianSelly LiLyNo ratings yet
- Wounds, Tissue Repair and ScarsDocument28 pagesWounds, Tissue Repair and ScarsShahid HameedNo ratings yet
- A Case Report of Femoral Neck Fracture in An ElderDocument7 pagesA Case Report of Femoral Neck Fracture in An ElderALIANo ratings yet