M3L2
M3L2
Download as pdf or txt
You might also like
- Private Car Insurance PolicyDocument3 pagesPrivate Car Insurance PolicySharma General Insurance AdvisorNo ratings yet
- Renewal of Your Easy Health Individual Standard Insurance PolicyDocument5 pagesRenewal of Your Easy Health Individual Standard Insurance PolicyHeena BhatNo ratings yet
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Thank You For Choosing ICICI Lombard General Insurance Company Limited (ICICI Lombard) As Your Preferred Service ProviderDocument3 pagesThank You For Choosing ICICI Lombard General Insurance Company Limited (ICICI Lombard) As Your Preferred Service ProviderSavita Bhabhi100% (2)
- Icici PolicyDocument2 pagesIcici Policydeepak7837No ratings yet
- Audit Walkthrough QuestionnaireDocument3 pagesAudit Walkthrough QuestionnaireRey Sabado100% (1)
- Bank StatementDocument3 pagesBank StatementNeha Pradeep SainiNo ratings yet
- 4128i HSRN 192700105 04 000Document18 pages4128i HSRN 192700105 04 000Padma ShivanandaNo ratings yet
- 4168 O-Tmcas 298685243 00 000Document8 pages4168 O-Tmcas 298685243 00 000insurancekatariaNo ratings yet
- Sub: Risk Assumption Letter: Insured & Vehicle DetailsDocument3 pagesSub: Risk Assumption Letter: Insured & Vehicle DetailsHIMANSHU MEHTANo ratings yet
- Thank You For Choosing ICICI Lombard General Insurance Company Limited (ICICI Lombard) As Your Preferred Service ProviderDocument2 pagesThank You For Choosing ICICI Lombard General Insurance Company Limited (ICICI Lombard) As Your Preferred Service Providerpasupuletikalapriya112No ratings yet
- PolicySchedule POPMCAR00100537049 628902242Document7 pagesPolicySchedule POPMCAR00100537049 628902242patwaryene.voltasNo ratings yet
- 3008 160520960 00 000Document3 pages3008 160520960 00 000Om prakashNo ratings yet
- Self Health Insurance 80 DDocument3 pagesSelf Health Insurance 80 Dinstatest3580No ratings yet
- Sub: Risk Assumption Letter: Insured & Vehicle DetailsDocument2 pagesSub: Risk Assumption Letter: Insured & Vehicle DetailsSUJEET KUMARNo ratings yet
- Komanduri Anantha CharyuluDocument1 pageKomanduri Anantha CharyuluAnanth KomanduriNo ratings yet
- Two Wheeler Package Policy Product Code: 3005 UIN:IRDAN115P0015V02200708 Certificate Cum Policy ScheduleDocument1 pageTwo Wheeler Package Policy Product Code: 3005 UIN:IRDAN115P0015V02200708 Certificate Cum Policy ScheduleMital PatelNo ratings yet
- Com - Icicilombard TWIPC P040000300518481431600000Document3 pagesCom - Icicilombard TWIPC P040000300518481431600000Shrirang KadamNo ratings yet
- Rjo2ba2549 PDFDocument2 pagesRjo2ba2549 PDFtalvinder singhNo ratings yet
- Cvi MW970852Document4 pagesCvi MW970852pe.pancardNo ratings yet
- Car Policy 2023-24Document1 pageCar Policy 2023-24jamunapariiNo ratings yet
- Personal Accident Insurance - POLMBKBA82EFIJBDocument3 pagesPersonal Accident Insurance - POLMBKBA82EFIJBGiridharan VenkateshNo ratings yet
- Digit Two-Wheeler Liability Only Policy: IRDAN158P0003V01201718Document2 pagesDigit Two-Wheeler Liability Only Policy: IRDAN158P0003V01201718PiyushNo ratings yet
- Enfield InsurencePolicy No 3005/132811383/00/000Document2 pagesEnfield InsurencePolicy No 3005/132811383/00/000Manne Venkata RangamNo ratings yet
- HDFC ERGO General Insurance Company Limited: Policy No. 2312 1005 0512 8700 000Document3 pagesHDFC ERGO General Insurance Company Limited: Policy No. 2312 1005 0512 8700 000rajkumargiritekarNo ratings yet
- 3001 A 184552264 00 B00 PyDocument2 pages3001 A 184552264 00 B00 PyRaghu DsNo ratings yet
- Miny Raj Modi PolicyDocument3 pagesMiny Raj Modi PolicySamaNo ratings yet
- Policy Copy (5) - UnlockedDocument6 pagesPolicy Copy (5) - UnlockedVignesh PNo ratings yet
- HDFC Car Latest (1) - RemovedDocument2 pagesHDFC Car Latest (1) - Removedsarath potnuriNo ratings yet
- New India Ashok Layland DostDocument3 pagesNew India Ashok Layland Dostsarath potnuriNo ratings yet
- United India Insurance Company Limited: WWW - Uiic.co - inDocument2 pagesUnited India Insurance Company Limited: WWW - Uiic.co - injaikrishnaa Maruti Driving SchoolNo ratings yet
- Sub: Risk Assumption Letter: Insured & Vehicle DetailsDocument3 pagesSub: Risk Assumption Letter: Insured & Vehicle DetailsNELLORE SATHYAMURTHY dilip kumarNo ratings yet
- Reliance General Insurance Company Limited: Reliance Two Wheeler Package Policy - ScheduleDocument6 pagesReliance General Insurance Company Limited: Reliance Two Wheeler Package Policy - Scheduleraj2364uNo ratings yet
- The New India Assurance Co. Ltd. Registered & Head Office:87, Mahatma Gandhi Road, Mumbai 400001Document4 pagesThe New India Assurance Co. Ltd. Registered & Head Office:87, Mahatma Gandhi Road, Mumbai 400001Nitesh KherdekarNo ratings yet
- Wego InsuranceDocument1 pageWego Insuranceuttam patraNo ratings yet
- Schedule Cum Certificate Bundled Private Car Insurance PolicyDocument8 pagesSchedule Cum Certificate Bundled Private Car Insurance PolicyAKSHIT GUPTANo ratings yet
- Policy CertificateDocument5 pagesPolicy CertificateRahulpatel25No ratings yet
- Bajaj Allianz General Insurance Company LTDDocument2 pagesBajaj Allianz General Insurance Company LTDMahesh H ANo ratings yet
- Cvi MX329537Document3 pagesCvi MX329537akrambasha095No ratings yet
- Iffco-Tokio General Co - LTD: Signature Not VerifiedDocument3 pagesIffco-Tokio General Co - LTD: Signature Not VerifiedDMustNeed mvrNo ratings yet
- Passion Pro Insurance 2019 20Document2 pagesPassion Pro Insurance 2019 20Santosh SNo ratings yet
- Bajaj InsuranceDocument3 pagesBajaj InsuranceAnil SharmaNo ratings yet
- PolicySoftCopy 509109346Document1 pagePolicySoftCopy 509109346Zishan100% (2)
- Reliance General Insurance Company Limited: "A" Policy For Act Liability Insurance (Private Car) - Policy ScheduleDocument6 pagesReliance General Insurance Company Limited: "A" Policy For Act Liability Insurance (Private Car) - Policy ScheduleRavi KantNo ratings yet
- ICICILombard General Insurance LTDDocument3 pagesICICILombard General Insurance LTDchotu.agrawal181No ratings yet
- Car InsuranceDocument3 pagesCar InsurancesmgkinduriNo ratings yet
- The Oriental Insurance Company Limited: Particulars of Insured VehicleDocument3 pagesThe Oriental Insurance Company Limited: Particulars of Insured VehicleAshok GothwalNo ratings yet
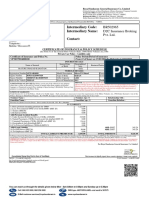
- Intermediary Code: Intermediary Name: Contact:: BR502965 D2C Insurance Broking Pvt. Ltd.Document2 pagesIntermediary Code: Intermediary Name: Contact:: BR502965 D2C Insurance Broking Pvt. Ltd.Zakir SzaNo ratings yet
- Car InsuranceDocument5 pagesCar InsuranceGokulNath AravindNo ratings yet
- Sub: Risk Assumption Letter: Insured & Vehicle DetailsDocument3 pagesSub: Risk Assumption Letter: Insured & Vehicle DetailsJaswant SinghNo ratings yet
- Insurance CertificateDocument3 pagesInsurance Certificatesameer143waghNo ratings yet
- PolicyDocument7 pagesPolicyranganadhNo ratings yet
- Car Insurance 2019Document3 pagesCar Insurance 2019Bhavin GamiNo ratings yet
- HDFC Two Wheeler PolicyDocument3 pagesHDFC Two Wheeler PolicybalaNo ratings yet
- Welcome To Transport Department Government of Telangana - IndiaDocument1 pageWelcome To Transport Department Government of Telangana - Indiashiva kumarNo ratings yet
- ICICI Health Policy 2022Document6 pagesICICI Health Policy 2022HuddarNo ratings yet
- 4168 O-Tmcas 298685240 00 000Document8 pages4168 O-Tmcas 298685240 00 000insurancekatariaNo ratings yet
- Insured & Vehicle Details: Product Code: 3001 UIN: IRDAN115P0017V01200102Document3 pagesInsured & Vehicle Details: Product Code: 3001 UIN: IRDAN115P0017V01200102patelsandip1989No ratings yet
- PDFDocument4 pagesPDFJwalant J AntaniNo ratings yet
- 31 2020 1571 PDFDocument2 pages31 2020 1571 PDFNandakishor AjNo ratings yet
- Harbir 0382 PypDocument1 pageHarbir 0382 Pypcommission sompoNo ratings yet
- Motor Insurance - Two Wheeler Liability Only: Certificate of Insurance Cum Policy ScheduleDocument3 pagesMotor Insurance - Two Wheeler Liability Only: Certificate of Insurance Cum Policy ScheduleKCitylink InternetNo ratings yet
- 4128i - HP - 99635250 - 02 - 000 - Aashish - Upto 20210314Document4 pages4128i - HP - 99635250 - 02 - 000 - Aashish - Upto 20210314adarshxl1No ratings yet
- DSDVDocument31 pagesDSDVajayroy12No ratings yet
- VLSM and Cidr: Routing Protocols and Concepts - Chapter 6Document23 pagesVLSM and Cidr: Routing Protocols and Concepts - Chapter 6ajayroy12No ratings yet
- Physical Layer: Solutions For In-Class and Practice ProblemsDocument2 pagesPhysical Layer: Solutions For In-Class and Practice Problemsajayroy12No ratings yet
- Ec2051 QBDocument5 pagesEc2051 QBajayroy12No ratings yet
- Noe 072Document1 pageNoe 072ajayroy12No ratings yet
- Analog Communication Ha3Document1 pageAnalog Communication Ha3ajayroy12No ratings yet
- 5 - Optimum Receivers For The AWGN Channel - Test - MODIFIED PDFDocument45 pages5 - Optimum Receivers For The AWGN Channel - Test - MODIFIED PDFajayroy12No ratings yet
- C411 L07 Pass Tran LogicDocument28 pagesC411 L07 Pass Tran Logicajayroy12No ratings yet
- Lec 22Document19 pagesLec 22ajayroy12No ratings yet
- Task 3Document2 pagesTask 3Wira KafryawanNo ratings yet
- Network Rules and SOPDocument6 pagesNetwork Rules and SOP陈奇No ratings yet
- HCP Lan Apm Fact Sheet 2017Document2 pagesHCP Lan Apm Fact Sheet 2017iggybauNo ratings yet
- Foreign Trade DocumentationDocument13 pagesForeign Trade DocumentationsonicstageNo ratings yet
- 202 Ways To Supplement Your Retirement Income PDFDocument344 pages202 Ways To Supplement Your Retirement Income PDFMauricio LustosaNo ratings yet
- Tekalg Assignment SwotDocument3 pagesTekalg Assignment Swotnatan manNo ratings yet
- Purchase ReceiptDocument3 pagesPurchase Receiptwindsorgarcia00No ratings yet
- Acct Statement XX8505 15122023Document6 pagesAcct Statement XX8505 15122023mohdfazal4545No ratings yet
- Datasheet: The 3NW WillDocument1 pageDatasheet: The 3NW WillEnzo DiviziaNo ratings yet
- Intern Report FinalDocument48 pagesIntern Report Finalmyothiriaung.mmNo ratings yet
- NIFOG Ver 2.0 508 Version FINAL 9-23-2021 (Signed)Document192 pagesNIFOG Ver 2.0 508 Version FINAL 9-23-2021 (Signed)maruka33No ratings yet
- Weekly Report 929 18-06-2021Document51 pagesWeekly Report 929 18-06-2021cpasl123No ratings yet
- Inter-Frequency Load BalancingDocument57 pagesInter-Frequency Load BalancingA AulakhNo ratings yet
- The Future of Money: A Cash-Free World?Document2 pagesThe Future of Money: A Cash-Free World?9325 김윤슬 Kim Yoon SeulNo ratings yet
- Dear Provider Relations RepresentativeDocument2 pagesDear Provider Relations RepresentativeDzenanStrujicNo ratings yet
- Tamara RLC Master v20 DIGITALDocument25 pagesTamara RLC Master v20 DIGITALanwar187No ratings yet
- TOA QuizletDocument13 pagesTOA QuizletJehugem BayawaNo ratings yet
- I To Communication SystemDocument46 pagesI To Communication SystemTariku TesfayeNo ratings yet
- Alcohol and Drug Abuse Flow ChartDocument1 pageAlcohol and Drug Abuse Flow Chartboen jaymeNo ratings yet
- SAP FICO Zero LevelDocument44 pagesSAP FICO Zero LevelAmit Shinde100% (1)
- Accounting CycleDocument17 pagesAccounting CycleAnonymous 1P4Me8680% (1)
- Inv 000429Document2 pagesInv 000429mdalamingoodboyokNo ratings yet
- Customer Relationship Management of Birla Sun LifeDocument72 pagesCustomer Relationship Management of Birla Sun LifepraveenworlNo ratings yet
- Notes Introduction To Logistics & Procurement 2023Document106 pagesNotes Introduction To Logistics & Procurement 2023Salmaan duraan CaliNo ratings yet
- IMS TrainingDocument96 pagesIMS Trainingomar ahmed100% (1)
- A Digital Business in 2024Document12 pagesA Digital Business in 2024rasalsheikhmNo ratings yet
- StudentDocument34 pagesStudentKevin CheNo ratings yet
- TCQTTTDocument32 pagesTCQTTTdohongvinh40No ratings yet