HAEC Europe
HAEC Europe
Download as pdf or txt
You might also like
- Back Pain - Finding Solutions For Your Aching Back - Harvard UniversityDocument7 pagesBack Pain - Finding Solutions For Your Aching Back - Harvard UniversityPradeep KumarNo ratings yet
- CPHQ Exam PracticeDocument65 pagesCPHQ Exam PracticeNazir AhmadNo ratings yet
- NHS FPX 6008 Assessment 2 Needs Analysis For ChangeDocument7 pagesNHS FPX 6008 Assessment 2 Needs Analysis For ChangeEmma WatsonNo ratings yet
- Manipal Manual of Clinical Book PDFDocument2 pagesManipal Manual of Clinical Book PDFMonisha Gunasekaran20% (5)
- Cuneyt Alper MD, Charles Bluestone MD, Margaretha Casselbrant, Joseph Dohar MD, Ellen Mandel MD - Advanced Therapy of Otitis Media (2003, PMPH Usa)Document576 pagesCuneyt Alper MD, Charles Bluestone MD, Margaretha Casselbrant, Joseph Dohar MD, Ellen Mandel MD - Advanced Therapy of Otitis Media (2003, PMPH Usa)Carmen-BadeaNo ratings yet
- Guideline No. 426: Hypertensive Disorders of Pregnancy: Diagnosis, Prediction, Prevention, and ManagementDocument26 pagesGuideline No. 426: Hypertensive Disorders of Pregnancy: Diagnosis, Prediction, Prevention, and ManagementYo Me100% (1)
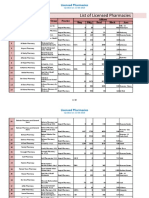
- PPR - LIST - Licensed Pharmacies - 20190613Document40 pagesPPR - LIST - Licensed Pharmacies - 20190613Muhammad RehanNo ratings yet
- How To Write Reflective Log EntryDocument14 pagesHow To Write Reflective Log EntryjamoNo ratings yet
- Ethics Paper 1Document9 pagesEthics Paper 1api-314968337No ratings yet
- Guidelines For The Diagnosis and Management of Hirschsprung-Associated EnterocolitisDocument5 pagesGuidelines For The Diagnosis and Management of Hirschsprung-Associated EnterocolitisNasrudin EfendiNo ratings yet
- Nihms-1901603 Esofago 5Document63 pagesNihms-1901603 Esofago 5pucegastroiessNo ratings yet
- HUS-consensus BaggaDocument18 pagesHUS-consensus Baggarakesh raushanNo ratings yet
- Efek Steroid HSPDocument16 pagesEfek Steroid HSPFarida UlfaNo ratings yet
- State of The Art Bowel Management For Pediatric Colorectal Problems Hirschsprung DiseaseDocument18 pagesState of The Art Bowel Management For Pediatric Colorectal Problems Hirschsprung Diseasehb62cmms9kNo ratings yet
- Hirsch Pung SDocument10 pagesHirsch Pung Sotto naftariNo ratings yet
- Helicobacter Pylori World Gastroenterology Organization Global Guideline 2023Document16 pagesHelicobacter Pylori World Gastroenterology Organization Global Guideline 2023Pann EiNo ratings yet
- Hiv 1 PDFDocument13 pagesHiv 1 PDFmaridaNo ratings yet
- Infantile Hypertrophic Pyloric Stenosis at A TertiDocument7 pagesInfantile Hypertrophic Pyloric Stenosis at A TertiVașadi Razvan CristianNo ratings yet
- Liptzin 2020Document19 pagesLiptzin 2020danniwebbNo ratings yet
- Norton 2015Document13 pagesNorton 2015Tifanny TantosoNo ratings yet
- 2024 Nofi Adennop CronicheDocument10 pages2024 Nofi Adennop CronicheLO RENo ratings yet
- 2023 - Li Et Al - Update of The Pathogenesis of Hirschsprung-Associated EnterocolitisDocument19 pages2023 - Li Et Al - Update of The Pathogenesis of Hirschsprung-Associated EnterocolitisDimas Bintoro KyhNo ratings yet
- NASPGHAN Clinical Practice Guideline For The Diagnosis and Treatment of Nonalcoholic Fatty Liver Disease in Children PDFDocument39 pagesNASPGHAN Clinical Practice Guideline For The Diagnosis and Treatment of Nonalcoholic Fatty Liver Disease in Children PDFLUIS ALBERTO FLORES NECIOSUPNo ratings yet
- Role of Fiberoptic Endoscopic Evaluation of Swallowing (FEES) in Children With Suspected DysphagiaDocument7 pagesRole of Fiberoptic Endoscopic Evaluation of Swallowing (FEES) in Children With Suspected Dysphagiababy kaiNo ratings yet
- Peds 2022060420Document20 pagesPeds 2022060420Hen CollectionNo ratings yet
- Significant Inconsistency Among Pediatric Oncologists in The Use of The Neutropenic DietDocument5 pagesSignificant Inconsistency Among Pediatric Oncologists in The Use of The Neutropenic Dietocampo silvinaNo ratings yet
- Awareness of Patients With Symptomatic Gallstones Regarding Their Own DiseaseDocument3 pagesAwareness of Patients With Symptomatic Gallstones Regarding Their Own DiseaseHelenCandyNo ratings yet
- JURNALLLLLLLLLLLLLLDocument13 pagesJURNALLLLLLLLLLLLLLbambangNo ratings yet
- Out 3Document15 pagesOut 3FanialiahsaniNo ratings yet
- ISJ-10575+RDocument5 pagesISJ-10575+RIffah Putri AndiniNo ratings yet
- Pediatrics 2015Document14 pagesPediatrics 2015Diana NunesNo ratings yet
- Nihms 737785Document78 pagesNihms 737785afg_19No ratings yet
- Desmarais 2015Document4 pagesDesmarais 2015Jesica DiazNo ratings yet
- Prader WilliDocument15 pagesPrader WilliGVHHNo ratings yet
- ESPEN Guideline On Clinical Nutrition in Inflammatory Bowel DiseaseDocument28 pagesESPEN Guideline On Clinical Nutrition in Inflammatory Bowel DiseaseAi NurfaiziyahNo ratings yet
- Blood Culture With CAPDocument10 pagesBlood Culture With CAPKaye Antonette AntioquiaNo ratings yet
- Glass 2016Document6 pagesGlass 2016Sʌɭɱʌŋ KʜʌŋNo ratings yet
- Acute Hematogenous Osteomyelitis in Children: Pathogenesis, Diagnosis, and TreatmentDocument10 pagesAcute Hematogenous Osteomyelitis in Children: Pathogenesis, Diagnosis, and TreatmentMerlin MuktialiNo ratings yet
- Diagnosis of Hirschsprung Disease: Lusine Ambartsumyan, Caitlin Smith, and Raj P KapurDocument15 pagesDiagnosis of Hirschsprung Disease: Lusine Ambartsumyan, Caitlin Smith, and Raj P KapurGhina Mauizha WulandariNo ratings yet
- Lactobacillus Rhamnosus GG Versus Placebo For Acute Gastroenteritis in ChildrenDocument21 pagesLactobacillus Rhamnosus GG Versus Placebo For Acute Gastroenteritis in ChildrenMarsella Epifania SuwignyoNo ratings yet
- Pediatric Hydrocephalus: Systematic Literature Review and Evidence-Based Guidelines. Part 1: Introduction and MethodologyDocument5 pagesPediatric Hydrocephalus: Systematic Literature Review and Evidence-Based Guidelines. Part 1: Introduction and MethodologyagusNo ratings yet
- Association Between Diarrhea Duration and Severity and Probiotic Efficacy in Children With Acute GastroenteritisDocument19 pagesAssociation Between Diarrhea Duration and Severity and Probiotic Efficacy in Children With Acute Gastroenteritis0019 Azhar WicaksonoNo ratings yet
- PIIS0923753422021767Document1 pagePIIS0923753422021767feriorrennaNo ratings yet
- Martin Harris Et Al 2021 The Modified Barium Swallow Study For Oropharyngeal Dysphagia Recommendations From AnDocument10 pagesMartin Harris Et Al 2021 The Modified Barium Swallow Study For Oropharyngeal Dysphagia Recommendations From AnCARLA ARACELI GÓMEZNo ratings yet
- Nihms 1688237Document20 pagesNihms 1688237Mohammed KhalidNo ratings yet
- Creamer Et Al-2016-British Journal of DermatologyDocument34 pagesCreamer Et Al-2016-British Journal of DermatologyAtika Indah SariNo ratings yet
- Hospitalization For Community-AcquiredDocument10 pagesHospitalization For Community-AcquiredJuwita PratiwiNo ratings yet
- Guideline No. 426: Hypertensive Disorders of Pregnancy: Diagnosis, Prediction, Prevention, and ManagementDocument26 pagesGuideline No. 426: Hypertensive Disorders of Pregnancy: Diagnosis, Prediction, Prevention, and Managementamelie.pubNo ratings yet
- Congenital Diaphragmatic Hernia Defect Size and Infant Morbidity at DischargeDocument10 pagesCongenital Diaphragmatic Hernia Defect Size and Infant Morbidity at DischargeResidencia Cirugía Pediátrica San JustoNo ratings yet
- Gastroesophageal Reflux Disease (Gastroenterology and Hepatology) PDFDocument408 pagesGastroesophageal Reflux Disease (Gastroenterology and Hepatology) PDFaab 1007No ratings yet
- Clinical Decision Making in The ICU Dysphagia Screening Assesment and TreatmentDocument18 pagesClinical Decision Making in The ICU Dysphagia Screening Assesment and TreatmentΜαρία ΧανιωτάκηNo ratings yet
- Nihms 932853Document83 pagesNihms 932853Ernesto BorgeNo ratings yet
- Liver Disease PDFDocument6 pagesLiver Disease PDFhpkrsigmpsaNo ratings yet
- Steroids in Treatment of RPA and PPADocument9 pagesSteroids in Treatment of RPA and PPAteu.yamNo ratings yet
- Polycystic Ovary SyndromeDocument13 pagesPolycystic Ovary SyndromeNAYSHA YANET CHAVEZ RONDINELNo ratings yet
- A Kap Study of Hepatitis Among Hepatitis Positive Patients Presenting To A Tertiary Care Hospital in Southern Punjab, PakistanDocument4 pagesA Kap Study of Hepatitis Among Hepatitis Positive Patients Presenting To A Tertiary Care Hospital in Southern Punjab, Pakistanارسلان علیNo ratings yet
- Diarrea en QuimioterapiaDocument6 pagesDiarrea en QuimioterapiaPaola DiazNo ratings yet
- Amsterdam Placental WorkshopDocument16 pagesAmsterdam Placental WorkshopCarlos Andrés Sánchez RuedaNo ratings yet
- Knowledge Level and Determinants of Neonatal Jaundice A Cross-Sectional Study in The Effutu Municipality of GhanaDocument10 pagesKnowledge Level and Determinants of Neonatal Jaundice A Cross-Sectional Study in The Effutu Municipality of GhananicloverNo ratings yet
- Evaluation and Management of Cholelithiasis in Children: A Hospital Based StudyDocument6 pagesEvaluation and Management of Cholelithiasis in Children: A Hospital Based StudyangelaanapakuNo ratings yet
- Quietes RenalesDocument13 pagesQuietes RenaleselresidenteNo ratings yet
- Revisiting The Refeeding SyndromeDocument29 pagesRevisiting The Refeeding SyndromeThếHuânNo ratings yet
- Distinct Clinical Phenotypes in Paediatric Cancer Patients With 2023 ECliniDocument9 pagesDistinct Clinical Phenotypes in Paediatric Cancer Patients With 2023 EClinironaldquezada038No ratings yet
- Guideline For The Evaluation of Cholestatic.23Document15 pagesGuideline For The Evaluation of Cholestatic.23Yuliawati HarunaNo ratings yet
- Henoch-Schönlein Purpura Corticosteroids May Improve Clinical Outcomes During Hospitalization ForDocument10 pagesHenoch-Schönlein Purpura Corticosteroids May Improve Clinical Outcomes During Hospitalization ForcalonghurstNo ratings yet
- Prospective Cohort StudyDocument6 pagesProspective Cohort StudyMãnoj MaheshwariNo ratings yet
- Evaluation and Management of Dysphagia: An Evidence-Based ApproachFrom EverandEvaluation and Management of Dysphagia: An Evidence-Based ApproachDhyanesh A. PatelNo ratings yet
- Inflammatory Bowel Disease: Pathogenesis, Diagnosis and ManagementFrom EverandInflammatory Bowel Disease: Pathogenesis, Diagnosis and ManagementRamona RajapakseNo ratings yet
- Osteomyelitis-Symptoms, Causes and Treatment: June 2018Document15 pagesOsteomyelitis-Symptoms, Causes and Treatment: June 2018raffellaNo ratings yet
- Diagnosis Treatment OsteoporosisDocument3 pagesDiagnosis Treatment OsteoporosisraffellaNo ratings yet
- HYDROTHERAPY and RA PDFDocument16 pagesHYDROTHERAPY and RA PDFraffellaNo ratings yet
- Screening, Diagnosis and Treatment of Osteoporosis: A Brief ReviewDocument7 pagesScreening, Diagnosis and Treatment of Osteoporosis: A Brief ReviewraffellaNo ratings yet
- Nsaid GuidelineDocument62 pagesNsaid GuidelineraffellaNo ratings yet
- Advance Trauma Life SupportDocument67 pagesAdvance Trauma Life SupportraffellaNo ratings yet
- CoverDocument30 pagesCoverraffellaNo ratings yet
- Vascular Trauma: DR Marolop, SP - BTKVDocument37 pagesVascular Trauma: DR Marolop, SP - BTKVraffellaNo ratings yet
- 1.zaanse Schans 2.museumplein (Home To The Rijksmuseum, The Van Gogh Museum and The Stedelijk Museum of Modern Art)Document1 page1.zaanse Schans 2.museumplein (Home To The Rijksmuseum, The Van Gogh Museum and The Stedelijk Museum of Modern Art)raffellaNo ratings yet
- Entrikel Takikardi (VT) Tanpa NadiDocument3 pagesEntrikel Takikardi (VT) Tanpa NadiraffellaNo ratings yet
- Use of High-Normal Levels of Hemoglobin A1C and Fasting Plasma Glucose For Diabetes Screening and Prediction - A Meta-AnalysisDocument16 pagesUse of High-Normal Levels of Hemoglobin A1C and Fasting Plasma Glucose For Diabetes Screening and Prediction - A Meta-AnalysisraffellaNo ratings yet
- Research Methodology: Global Halal Logo StandardizationDocument35 pagesResearch Methodology: Global Halal Logo StandardizationraffellaNo ratings yet
- Research TittleDocument1 pageResearch TittleraffellaNo ratings yet
- COVID19 Management Algorithm 22042021 v1Document1 pageCOVID19 Management Algorithm 22042021 v1shivani shindeNo ratings yet
- ArtikelDocument9 pagesArtikelMurdock HannibalNo ratings yet
- FINAL-BOOKLET-DECEMBER-2024-GRADUATION (1)Document133 pagesFINAL-BOOKLET-DECEMBER-2024-GRADUATION (1)godarkmuneneNo ratings yet
- FIMNCI Facilitator Guide 2023Document96 pagesFIMNCI Facilitator Guide 2023ravikantNo ratings yet
- Euthanasia: Medical Point of View 1Document4 pagesEuthanasia: Medical Point of View 1Jesus VillanuevaNo ratings yet
- 5Document41 pages5myNo ratings yet
- Tugas Bhasa Inggris 1Document4 pagesTugas Bhasa Inggris 1indah tri setyowatiNo ratings yet
- What Doctors Dont Tell You - The Dental Handbook PDFDocument124 pagesWhat Doctors Dont Tell You - The Dental Handbook PDFpsychpostersNo ratings yet
- Group Capstone TusharDocument14 pagesGroup Capstone TusharTushar GNo ratings yet
- NURSING DIAGNOSIS On Pregnant WomanDocument2 pagesNURSING DIAGNOSIS On Pregnant Womananon_168410816No ratings yet
- Final Exam English 2Document3 pagesFinal Exam English 2Irma PutriNo ratings yet
- Perawatan Paliatif Pada OdhaDocument45 pagesPerawatan Paliatif Pada Odhaveni vebriantiNo ratings yet
- GI Bleed InpatientDocument17 pagesGI Bleed InpatientAnisaNo ratings yet
- L3 Apply-1Document1 pageL3 Apply-1Rachelle Mae MendezNo ratings yet
- B2 - WCET - INWOCNA 2017 by IrmaDocument37 pagesB2 - WCET - INWOCNA 2017 by Irmafajar adironiNo ratings yet
- Code Blue: The Growing Threat of Non-Communicable Diseases On Maternal HealthDocument4 pagesCode Blue: The Growing Threat of Non-Communicable Diseases On Maternal HealthThe Wilson Center100% (1)
- Tasya Fitri RamadantiDocument45 pagesTasya Fitri RamadantiadelacalistaaNo ratings yet
- Occlusal Considerations For Implant Restorations in The Partially Edentulous PatientDocument54 pagesOcclusal Considerations For Implant Restorations in The Partially Edentulous PatientmarwaNo ratings yet
- Canada - Medical Exam FormDocument1 pageCanada - Medical Exam FormEsykiel Nool MedranoNo ratings yet
- DO Letter ModelDocument2 pagesDO Letter ModelmylpalegalNo ratings yet
- Health Care Ethics 2024Document13 pagesHealth Care Ethics 2024celestineNo ratings yet
- General Interview GuidelinesDocument10 pagesGeneral Interview GuidelinesArjun NeupaneNo ratings yet