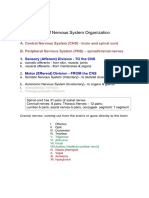
Anatomy of Peripheral Nerves: (Click On Pictures To Enlarge - Click "Back" To Close)
Anatomy of Peripheral Nerves: (Click On Pictures To Enlarge - Click "Back" To Close)
Download as pdf or txt
You might also like
- Akil Palanisamy MD The TIGER Protocol An Integrative 5 Step Program To Treat and Heal Your AutoimmDocument457 pagesAkil Palanisamy MD The TIGER Protocol An Integrative 5 Step Program To Treat and Heal Your Autoimmharabor madalina100% (1)
- CH 06 Nervous System (MS)Document63 pagesCH 06 Nervous System (MS)alyssa bananNo ratings yet
- AnaPhy - Nervous TissueDocument73 pagesAnaPhy - Nervous TissuesoraruNo ratings yet
- Cohen - B7.5 - MSK - Central - and - Peripheral - Nervous - System - Histology - 19-20Document80 pagesCohen - B7.5 - MSK - Central - and - Peripheral - Nervous - System - Histology - 19-20Monica Hitomi MekaruNo ratings yet
- NERVOUS TISSUE-4-MYELINATION_240818_175441Document70 pagesNERVOUS TISSUE-4-MYELINATION_240818_175441hemNo ratings yet
- Nerve TissueDocument5 pagesNerve TissueSuccessfactors TrainerNo ratings yet
- Lewis Neuro EndDocument274 pagesLewis Neuro Endrmoyle98No ratings yet
- Nervous TissueDocument42 pagesNervous Tissuekirabogift774No ratings yet
- SEER 2023 NerveTissueDocument2 pagesSEER 2023 NerveTissueShweta KhannaNo ratings yet
- Overview of Nervous Tissue Along With Related StructureDocument50 pagesOverview of Nervous Tissue Along With Related StructureNarayan GhimireNo ratings yet
- Macroglia+Neuron ASG 16-01-2023 PDFDocument9 pagesMacroglia+Neuron ASG 16-01-2023 PDFRajat AgrawalNo ratings yet
- Histologyofthenervoussystem 140905044427 Phpapp02 200729202123Document27 pagesHistologyofthenervoussystem 140905044427 Phpapp02 200729202123aishwarya1101999No ratings yet
- Nervous System: Alianza Paras Casue Darjani Fojas Tan Zebaradami MassoudiDocument76 pagesNervous System: Alianza Paras Casue Darjani Fojas Tan Zebaradami MassoudiLionell CastilloNo ratings yet
- Nervous TissueDocument25 pagesNervous TissueSumayya KabeerNo ratings yet
- Nervous Tissue PDFDocument4 pagesNervous Tissue PDFFadhil Hussam AhmedNo ratings yet
- 2. Nervous System - HistologyDocument25 pages2. Nervous System - HistologyManya SharmaNo ratings yet
- FINALS 2 5-Nervoustissue-161014172642Document56 pagesFINALS 2 5-Nervoustissue-161014172642Maika Ysabelle RavaloNo ratings yet
- Made Up of Neurons and Neuroglia Cells: Anatomical Subdivisions of NSDocument18 pagesMade Up of Neurons and Neuroglia Cells: Anatomical Subdivisions of NSJavorko PNo ratings yet
- Nervous System 1Document8 pagesNervous System 1Diana Joyce PerezNo ratings yet
- Overview of Nervous SystemDocument63 pagesOverview of Nervous SystemMAHARANI100% (1)
- 4.histology of the nervous systemDocument125 pages4.histology of the nervous systemabdikalik6666No ratings yet
- Nervous Tissue 1Document30 pagesNervous Tissue 1OtencianoNo ratings yet
- pathology of the nervous system (1)(1)Document53 pagespathology of the nervous system (1)(1)chebichiimercy64No ratings yet
- (Oct 1) Nervous-SystemDocument78 pages(Oct 1) Nervous-SystemBea Gualberto100% (1)
- 20_ CNS Demyelinating Disease - Version 1Document15 pages20_ CNS Demyelinating Disease - Version 1ZullyNo ratings yet
- Nervous TissueDocument12 pagesNervous TissueTanveesh BajajNo ratings yet
- Wk6 Nervous SystemDocument4 pagesWk6 Nervous SystemLindenScholesNo ratings yet
- chap 10Document6 pageschap 10jordainemiah374No ratings yet
- Unit 2 - Nervous SystemDocument39 pagesUnit 2 - Nervous SystemzulieyanaNo ratings yet
- PSY Chapter 12Document12 pagesPSY Chapter 12Preethu RNo ratings yet
- Anaphy Reviewer (Semi Finals)Document28 pagesAnaphy Reviewer (Semi Finals)Sophia Mae ClavecillaNo ratings yet
- Anaphy Reviewer (Semi Finals)Document5 pagesAnaphy Reviewer (Semi Finals)Sophia Mae ClavecillaNo ratings yet
- Nerve AnatomyDocument7 pagesNerve AnatomyvkumaranNo ratings yet
- NERVEDocument18 pagesNERVEDua EimanNo ratings yet
- Chap8 Nervous Transes-1-1Document8 pagesChap8 Nervous Transes-1-1y30ny30nNo ratings yet
- NeuropathologyDocument66 pagesNeuropathologyKaramsi Gopinath NaikNo ratings yet
- Botan's Cns and The Brain 2023Document115 pagesBotan's Cns and The Brain 2023Caamir Dek HaybeNo ratings yet
- Anatomy and Physiology of The NerveDocument18 pagesAnatomy and Physiology of The NervejudssalangsangNo ratings yet
- UpikDocument21 pagesUpikaldybebikaNo ratings yet
- Nerve and Its Function PDFDocument26 pagesNerve and Its Function PDFJose albert MauanayNo ratings yet
- The Nervous SystemDocument18 pagesThe Nervous SystemSheyn Mahru ConomanNo ratings yet
- محاضره الجهاز العصبي 2025Document33 pagesمحاضره الجهاز العصبي 2025misoga233No ratings yet
- 15.09.14. Pro. Nerve Fiber TypesDocument33 pages15.09.14. Pro. Nerve Fiber Typesashok_solanki_23No ratings yet
- Anatomy and Physiology of Nervous SystemDocument26 pagesAnatomy and Physiology of Nervous SystemDR. KUMARASWAMI HEALTH CENTRE COLLEGE OF NURSING KANYAKUMARINo ratings yet
- Nerve RegenerationDocument2 pagesNerve RegenerationHajar BakiNo ratings yet
- NervusDocument8 pagesNervusAndika Anjani AgustinNo ratings yet
- Neural Control and Coordination Notes For NEET Download PDF - pdf-20Document7 pagesNeural Control and Coordination Notes For NEET Download PDF - pdf-20Legendary KingNo ratings yet
- NeuroradiologyCurrent and Future Imaging of The Peripheral NervoussystemDocument10 pagesNeuroradiologyCurrent and Future Imaging of The Peripheral NervoussystemRyanNo ratings yet
- 1 Part I Central Nervous System 4zaDocument32 pages1 Part I Central Nervous System 4zaapi-302883249No ratings yet
- Mylein SheathDocument5 pagesMylein Sheathأحمد الزهيرىNo ratings yet
- Nervous System - NeuronDocument30 pagesNervous System - Neuronvanshikhatrivedi1205No ratings yet
- NERVOUS SYSTEM _Document84 pagesNERVOUS SYSTEM _Lowell FollanteNo ratings yet
- Lab 9 Nervous TissueDocument28 pagesLab 9 Nervous TissueSarwar JafarNo ratings yet
- Nervous Tissue-6-Nerve Fibre Regeneration_240827_181534Document59 pagesNervous Tissue-6-Nerve Fibre Regeneration_240827_181534hemNo ratings yet
- Konsep Dasar Ilmu Biokimia Dan Biologi Molekuler Untuk Sistem SarafDocument31 pagesKonsep Dasar Ilmu Biokimia Dan Biologi Molekuler Untuk Sistem SarafdiandraNo ratings yet
- Nervous System HistologyDocument4 pagesNervous System HistologyShelly Stephanie Bintoro100% (1)
- 6. Biomechanics of Peripheral and Spinal NervesDocument41 pages6. Biomechanics of Peripheral and Spinal Nervespradeep6288No ratings yet
- Neurodegeneration Solutions in the Arab World: A Fusion of Tradition and TechnologyFrom EverandNeurodegeneration Solutions in the Arab World: A Fusion of Tradition and TechnologyNo ratings yet
- Nerve Cell, Functions, Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandNerve Cell, Functions, Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- IAC Valve SilencersDocument16 pagesIAC Valve SilencersvkumaranNo ratings yet
- Training On Process Piping: DescriptionDocument2 pagesTraining On Process Piping: DescriptionvkumaranNo ratings yet
- V2C - Centrifugal Pump (For PM)Document2 pagesV2C - Centrifugal Pump (For PM)vkumaranNo ratings yet
- V2C - Centrifugal Compressor (For PM)Document2 pagesV2C - Centrifugal Compressor (For PM)vkumaranNo ratings yet
- Thai Vegetable Soup (Healthy Soups and Salads Recipe) Recipe - by Tarla Dalal - Tarladalal - Com - #4621Document5 pagesThai Vegetable Soup (Healthy Soups and Salads Recipe) Recipe - by Tarla Dalal - Tarladalal - Com - #4621vkumaranNo ratings yet
- Effect of Viscosity On Pump Performance: Public Courses In-House Courses Operator TrainingDocument3 pagesEffect of Viscosity On Pump Performance: Public Courses In-House Courses Operator TrainingvkumaranNo ratings yet
- Potato and Spring Onion Soup, Thai Soup Recipe - Thai Recipes - by Tarla Dalal - Tarladalal - Com - #432Document4 pagesPotato and Spring Onion Soup, Thai Soup Recipe - Thai Recipes - by Tarla Dalal - Tarladalal - Com - #432vkumaranNo ratings yet
- HEMP MethodDocument10 pagesHEMP MethodvkumaranNo ratings yet
- DailySafetyMessages PDFDocument3 pagesDailySafetyMessages PDFvkumaranNo ratings yet
- Silencer PDFDocument4 pagesSilencer PDFvkumaranNo ratings yet
- UOP291 Chloride Test MethodDocument11 pagesUOP291 Chloride Test Methodvkumaran100% (2)
- Acute Manifestations of Neuromuscular DiseaseDocument10 pagesAcute Manifestations of Neuromuscular DiseasetsyrahmaniNo ratings yet
- Malignant Breast DiseasesDocument28 pagesMalignant Breast DiseasesLily Margaret CharlotteNo ratings yet
- Decompensated Cirrhosis: Clinical Practice GuidelinesDocument96 pagesDecompensated Cirrhosis: Clinical Practice GuidelinesJULIANo ratings yet
- Inborn: Unit 5 Nursing Care of Children With Endocrine and Metabolic DisordersDocument22 pagesInborn: Unit 5 Nursing Care of Children With Endocrine and Metabolic DisorderswelahiNo ratings yet
- Guide To Indian Health and Beauty EnchantessDocument32 pagesGuide To Indian Health and Beauty EnchantessSuruchi Chopra100% (1)
- Intracellular Accumulation: Presenter Amon Facilitator Prof Amos MwakigonjaDocument23 pagesIntracellular Accumulation: Presenter Amon Facilitator Prof Amos MwakigonjaNtobi ThomasNo ratings yet
- The 5:2 Fast Diet: An Ayurvedic Review: by Nadia MarshallDocument4 pagesThe 5:2 Fast Diet: An Ayurvedic Review: by Nadia MarshallLemonNo ratings yet
- Review of Related Literature and StudiesDocument5 pagesReview of Related Literature and StudiesYrrem UbaganNo ratings yet
- Epidemiology of Diabetes MellitusDocument5 pagesEpidemiology of Diabetes Mellitusarkanthos77100% (1)
- Sympathy and AntipathyDocument2 pagesSympathy and AntipathytusharNo ratings yet
- Guidance To Seasonal Community - EnglishDocument2 pagesGuidance To Seasonal Community - EnglishCape Cod Times33% (3)
- Hiperemesis GravidarumDocument8 pagesHiperemesis GravidarumIntan PermataNo ratings yet
- Health Assessment-Finals: Assessing Musculoskeletal SystemDocument12 pagesHealth Assessment-Finals: Assessing Musculoskeletal Systemelena ampatinNo ratings yet
- A List of Psychological DisordersDocument2 pagesA List of Psychological DisordersJillian100% (2)
- ReadingAndWriting W4 (GMaulit)Document1 pageReadingAndWriting W4 (GMaulit)Glydel AlyannaNo ratings yet
- Heart RhythmsDocument68 pagesHeart Rhythmsyasahswi91No ratings yet
- Diseases." (Aphorism No 71)Document44 pagesDiseases." (Aphorism No 71)Jasim SalimNo ratings yet
- Streptokinase in The Treatment of Pleural Controlled Trial of IntrapleuralDocument7 pagesStreptokinase in The Treatment of Pleural Controlled Trial of IntrapleuraltomgasoneNo ratings yet
- General Education 8Document6 pagesGeneral Education 8Tingson Patricia MaeNo ratings yet
- Rakowski DetDocument2 pagesRakowski DethohogreenNo ratings yet
- Excerpt From Ebook 1: Chronic Illness Trauma StudiesDocument20 pagesExcerpt From Ebook 1: Chronic Illness Trauma StudiesAnghel TeodoraNo ratings yet
- FertiQoL ScoringDocument2 pagesFertiQoL ScoringGaoudam Natarajan100% (1)
- Pathology of NoaDocument164 pagesPathology of NoaAnonymous milwFDXNo ratings yet
- What Is HypothyroidismDocument4 pagesWhat Is HypothyroidismKevin ScottNo ratings yet
- Renal or Urinary Tract DisorderDocument6 pagesRenal or Urinary Tract DisorderMarcel Quario OrinaNo ratings yet
- Nervous ShockDocument18 pagesNervous ShocksfreigaNo ratings yet
- Abnormal Psychology ReviewerDocument14 pagesAbnormal Psychology ReviewerLadee KharryleNo ratings yet
- Research Journal of Pharmaceutical, Biological and Chemical SciencesDocument12 pagesResearch Journal of Pharmaceutical, Biological and Chemical Sciencesrr48843No ratings yet
- What Is Covid 19Document2 pagesWhat Is Covid 19Estela RodríguezNo ratings yet