Pharmacologic Treatment of
Pharmacologic Treatment of
Download as pdf or txt
You might also like
- Psychiatry Under the Influence: Institutional Corruption, Social Injury, and Prescriptions for ReformFrom EverandPsychiatry Under the Influence: Institutional Corruption, Social Injury, and Prescriptions for ReformRating: 2 out of 5 stars2/5 (1)
- Family Nursing With Childbearing FamiliesDocument16 pagesFamily Nursing With Childbearing FamiliesIndra Siahaan100% (1)
- The Complete List of NANDA Nursing Diagnosis For 2012Document4 pagesThe Complete List of NANDA Nursing Diagnosis For 2012annNo ratings yet
- Self-Help Groups. Are They EffectiveDocument4 pagesSelf-Help Groups. Are They EffectiveMeiko Mey-Rin100% (1)
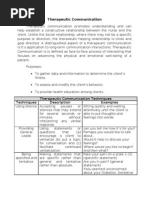
- Therapeutic CommunicationDocument4 pagesTherapeutic CommunicationLloyd Rafael Estabillo100% (1)
- Therapeutic Communication - Doc 12345Document8 pagesTherapeutic Communication - Doc 12345KBSNo ratings yet
- Birthing Beliefs in The PhilippinesDocument2 pagesBirthing Beliefs in The PhilippinesJeeyan DelgadoNo ratings yet
- Binge EatingDocument10 pagesBinge Eatingapi-298326412No ratings yet
- Therapeutic CommunicationDocument7 pagesTherapeutic CommunicationJoseph Rommel Castro CortezNo ratings yet
- All About Bulimia Nervosa A Booklet For Those Wanting To Know More UK 2000 PDFDocument20 pagesAll About Bulimia Nervosa A Booklet For Those Wanting To Know More UK 2000 PDFEasy MoneyNo ratings yet
- Post Partum Depression-NSDDocument7 pagesPost Partum Depression-NSDkat_tupaz100% (1)
- Canubas Laly RoseDocument20 pagesCanubas Laly RoseLaly Rose CanubasNo ratings yet
- Postpartum DepressionDocument50 pagesPostpartum DepressionwarnerNo ratings yet
- Behavioral Models of Binge-Type EatingDocument8 pagesBehavioral Models of Binge-Type Eatingpechy83No ratings yet
- Psychiatric and Mental Health NursingDocument10 pagesPsychiatric and Mental Health NursingGlaiza Claire Am-amlan OlayanNo ratings yet
- Neuropsychology of An Addictive MindDocument45 pagesNeuropsychology of An Addictive MindDr Nader KorhaniNo ratings yet
- SchizophreniaDocument22 pagesSchizophreniaalfauzi syamsudinNo ratings yet
- Obsessive Compulsive DisorderDocument14 pagesObsessive Compulsive Disorderfrancis00090100% (1)
- CH34 Child Health AssessmentDocument6 pagesCH34 Child Health AssessmentJharaNo ratings yet
- Adjustment Disorders - Medscape 2016Document8 pagesAdjustment Disorders - Medscape 2016manuelNo ratings yet
- Systematic DesensitisationDocument20 pagesSystematic Desensitisationstu_aroNo ratings yet
- Pubh 1005: Sleeps, Eats & Exercises Sleep Log Assignment Name: Date Complete in The MorningDocument3 pagesPubh 1005: Sleeps, Eats & Exercises Sleep Log Assignment Name: Date Complete in The Morningtpark101No ratings yet
- Hildegard Peplau's Interpersonal Relations 101Document88 pagesHildegard Peplau's Interpersonal Relations 101Ynaffit Alteza UntalNo ratings yet
- Graves DiseaseDocument8 pagesGraves Diseasenini07No ratings yet
- The Health Belief Model - Pdfevan BurkeDocument3 pagesThe Health Belief Model - Pdfevan BurkeAKbarNo ratings yet
- Depression and Psychodynamic PsychotherapyDocument5 pagesDepression and Psychodynamic PsychotherapyRija ChoudhryNo ratings yet
- Professional Nursing Case Study TemplateDocument3 pagesProfessional Nursing Case Study TemplateShane Aileen AngelesNo ratings yet
- Geneva Mccloud-Hw410-Unit 9 Final ProjectDocument36 pagesGeneva Mccloud-Hw410-Unit 9 Final Projectapi-324792741100% (1)
- Bulimia Nervosa: Signs and SymptomsDocument4 pagesBulimia Nervosa: Signs and Symptomseneg4530No ratings yet
- Problems With Psyche Factors HandwrittenDocument2 pagesProblems With Psyche Factors HandwrittenRussel Kate SulangNo ratings yet
- PSYCH REPORT - Parenting StyleDocument53 pagesPSYCH REPORT - Parenting StyleMark ReyesNo ratings yet
- Nausea and VomitingDocument9 pagesNausea and VomitingHusaifah BaliwanNo ratings yet
- Mood Disorder (Mania)Document11 pagesMood Disorder (Mania)Sheetal PundirNo ratings yet
- Psychiatric Mental Health Comprehensive Case StudyDocument10 pagesPsychiatric Mental Health Comprehensive Case Studyapi-526815418No ratings yet
- Eating DisordersDocument46 pagesEating Disordersedrinsne100% (1)
- Understanding Pku 2014Document5 pagesUnderstanding Pku 2014reriti2008No ratings yet
- Mental State ExaminationDocument26 pagesMental State ExaminationChristopher Skinner86% (7)
- Smiley - Nursing Philosophy PaperDocument11 pagesSmiley - Nursing Philosophy Paperapi-526685362100% (1)
- Uterine CancerDocument20 pagesUterine CancerAjurs UrsabiaNo ratings yet
- Reactive Attachment Disorder & Trauma, A Powerpoint PresentationDocument23 pagesReactive Attachment Disorder & Trauma, A Powerpoint PresentationJane Gilgun100% (2)
- Polycystic Ovarian Syndrome and HomeopathyDocument3 pagesPolycystic Ovarian Syndrome and HomeopathyAnonymous dpxYTENo ratings yet
- Defense MechanismsDocument4 pagesDefense MechanismsEiziddeen IsmailNo ratings yet
- Drug Study For WorkbookDocument7 pagesDrug Study For WorkbookTrisha VergaraNo ratings yet
- Mental Status Exam in DepressionDocument2 pagesMental Status Exam in DepressionChris PenNo ratings yet
- Nursing Care PlanDocument25 pagesNursing Care PlanIndah MardianiNo ratings yet
- PsychopharmacologyDocument160 pagesPsychopharmacologyInah Sarita100% (1)
- BSN3 - PSYCHIA - Mood Disorders and Suicidal IdeationDocument7 pagesBSN3 - PSYCHIA - Mood Disorders and Suicidal IdeationADRIANNA NICOLE BAHALA GONZALEZ100% (2)
- Type 1 Diabetes OutlineDocument2 pagesType 1 Diabetes OutlineDominique PorterNo ratings yet
- HopelessnessDocument20 pagesHopelessnessSyed BuRhan Ud-DinNo ratings yet
- Diabetes MellitusDocument9 pagesDiabetes MellitusJulius Ceasar SincoNo ratings yet
- TPN CalculationsDocument4 pagesTPN Calculationsapi-293416259100% (1)
- Eating Disorders and Nursing CareDocument36 pagesEating Disorders and Nursing CareMuhammad Arsyad SubuNo ratings yet
- Anxiety Disorder: Student Name: Malinda SirueDocument9 pagesAnxiety Disorder: Student Name: Malinda SirueEsmareldah Henry SirueNo ratings yet
- Transforming the Legacy: Couple Therapy with Survivors of Childhood TraumaFrom EverandTransforming the Legacy: Couple Therapy with Survivors of Childhood TraumaNo ratings yet
- Overcoming Eating Disorders: A Simple Guide to Causes, Prevention and Treatments of Eating Disorders in AthletesFrom EverandOvercoming Eating Disorders: A Simple Guide to Causes, Prevention and Treatments of Eating Disorders in AthletesNo ratings yet
- Telling Ed No!: And Other Practical Tools to Conquer Your Eating Disorder and Find FreedomFrom EverandTelling Ed No!: And Other Practical Tools to Conquer Your Eating Disorder and Find FreedomNo ratings yet
- Integrative Dual Diagnosis Treatment Approach to an Individual with Alcoholism and Coexisting Endogenous DepressionFrom EverandIntegrative Dual Diagnosis Treatment Approach to an Individual with Alcoholism and Coexisting Endogenous DepressionRating: 2 out of 5 stars2/5 (1)
- A Simple Guide to Cholangitis, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Cholangitis, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Psychotropic MedicationDocument28 pagesPsychotropic Medicationrmconvidhya sri2015No ratings yet
- Using Transference-Focused Psychotherapy 2018Document11 pagesUsing Transference-Focused Psychotherapy 2018Dhino Armand Quispe SánchezNo ratings yet
- Hearingloss: The Silent Risk For Psychiatric Disorders in Late LifeDocument9 pagesHearingloss: The Silent Risk For Psychiatric Disorders in Late LifeDhino Armand Quispe SánchezNo ratings yet
- The Neurobiology of 2018Document18 pagesThe Neurobiology of 2018Dhino Armand Quispe SánchezNo ratings yet
- Entomology - 1 - David - S1-6 Insecticide Resistance in Insect VectorsDocument9 pagesEntomology - 1 - David - S1-6 Insecticide Resistance in Insect VectorsDhino Armand Quispe SánchezNo ratings yet
- Differential Diagnosis of 2018Document8 pagesDifferential Diagnosis of 2018Dhino Armand Quispe SánchezNo ratings yet
- Manualized Psychotherapies 2018Document11 pagesManualized Psychotherapies 2018Dhino Armand Quispe SánchezNo ratings yet
- The Longitudinal Course of 018Document10 pagesThe Longitudinal Course of 018Dhino Armand Quispe SánchezNo ratings yet
- Personality Variables and 2018Document15 pagesPersonality Variables and 2018Dhino Armand Quispe SánchezNo ratings yet
- Contemporary Psychiatry 2018 PDFDocument9 pagesContemporary Psychiatry 2018 PDFDhino Armand Quispe SánchezNo ratings yet
- Individualized Metacognitive Training (MCT+)Document10 pagesIndividualized Metacognitive Training (MCT+)Dhino Armand Quispe SánchezNo ratings yet
- Deep Brain Stimulation in 2018Document11 pagesDeep Brain Stimulation in 2018Dhino Armand Quispe SánchezNo ratings yet
- Social Cognition and 2018Document20 pagesSocial Cognition and 2018Dhino Armand Quispe SánchezNo ratings yet
- Cognitive Neuroscience of 2018Document17 pagesCognitive Neuroscience of 2018Dhino Armand Quispe SánchezNo ratings yet
- Advocacy For Psychodynamic 2018Document15 pagesAdvocacy For Psychodynamic 2018Dhino Armand Quispe SánchezNo ratings yet
- Comorbidity of Borderline 2018Document11 pagesComorbidity of Borderline 2018Dhino Armand Quispe SánchezNo ratings yet
- Treatment ResistantDocument13 pagesTreatment ResistantDhino Armand Quispe SánchezNo ratings yet
- Psychodynamic Psychiatry, 6-Minute 2018Document13 pagesPsychodynamic Psychiatry, 6-Minute 2018Dhino Armand Quispe SánchezNo ratings yet
- Journal of Affective DisordersDocument64 pagesJournal of Affective DisordersDhino Armand Quispe SánchezNo ratings yet
- Urgent and EmergentDocument15 pagesUrgent and EmergentDhino Armand Quispe SánchezNo ratings yet
- Cardiac Amyloidosis: Updates in Diagnosis and ManagementDocument13 pagesCardiac Amyloidosis: Updates in Diagnosis and ManagementDhino Armand Quispe SánchezNo ratings yet
- Psychiatric I PDFDocument10 pagesPsychiatric I PDFDhino Armand Quispe SánchezNo ratings yet
- Guideline WatchDocument43 pagesGuideline WatchDhino Armand Quispe SánchezNo ratings yet
- Kennedy Ross Mac Nab 2015Document38 pagesKennedy Ross Mac Nab 2015HERRY HERRYNo ratings yet
- Treatment of Adult Major Depressive Disorder (MDD) ToolDocument12 pagesTreatment of Adult Major Depressive Disorder (MDD) ToolSubhash SharmaNo ratings yet
- Bereavement and GriefDocument28 pagesBereavement and GriefGeorgiana PrisoschiNo ratings yet
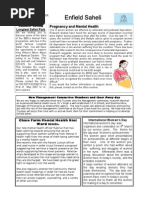
- April 2007Document2 pagesApril 2007enfieldclubhouseNo ratings yet
- Psychiatric Nursing Exam f2fDocument5 pagesPsychiatric Nursing Exam f2fFerdinand Tercero100% (1)
- Schizophrenia Spectrum and Other Psychotic DisordersDocument84 pagesSchizophrenia Spectrum and Other Psychotic DisordersJara YumiNo ratings yet
- APA Guidelines For Treating Adults With SchizophreniaDocument8 pagesAPA Guidelines For Treating Adults With SchizophreniaKaren C. ManoodNo ratings yet
- Javeria ZahidDocument16 pagesJaveria ZahidSAMIA BATOOLNo ratings yet
- PHQ 2 PDFDocument2 pagesPHQ 2 PDFnaufal12345No ratings yet
- APA - DSM5 - Level 2 Depression Adult PDFDocument3 pagesAPA - DSM5 - Level 2 Depression Adult PDFandreea_zgrNo ratings yet
- PDF - Scientific AmericanDocument80 pagesPDF - Scientific Americanprotectthebrain100% (8)
- Thesis DefendedDocument84 pagesThesis Defendedkathleen bernardoNo ratings yet
- Bullying ArticleDocument6 pagesBullying Articlebarn5094100% (1)
- English For Academic and Professional Purposes: Quarter 2 - Module 8Document35 pagesEnglish For Academic and Professional Purposes: Quarter 2 - Module 8Unick Soriano NastorNo ratings yet
- Chapter 16: Psychological Disorders: Multiple ChoiceDocument4 pagesChapter 16: Psychological Disorders: Multiple ChoiceJamie100% (1)
- From Personalized Medicine To Population Health: A Survey of Mhealth Sensing TechniquesDocument24 pagesFrom Personalized Medicine To Population Health: A Survey of Mhealth Sensing TechniquesAbdulrhman AlshameriNo ratings yet
- Episodes of Mania/Depression: Psychopathophysiology (Bipolar 1 Disorder, Mre Manic With Psychotic Features)Document1 pageEpisodes of Mania/Depression: Psychopathophysiology (Bipolar 1 Disorder, Mre Manic With Psychotic Features)KathHinlogNo ratings yet
- DEC 2007-NPT 2-Questions and RationaleDocument17 pagesDEC 2007-NPT 2-Questions and RationaleRoy Salvador100% (1)
- Pelzer Et Al 2023 Neurological and Psychiatric Comorbidities of Migraine Concepts and Future PerspectivesDocument15 pagesPelzer Et Al 2023 Neurological and Psychiatric Comorbidities of Migraine Concepts and Future Perspectivespaulo gutierrezNo ratings yet
- Perdev Module 4 Lesson Plan - RevisedDocument12 pagesPerdev Module 4 Lesson Plan - Revisedmsalino.tcNo ratings yet
- Clinical Psychologists' Perceptions of Persons With Mental IllnessDocument6 pagesClinical Psychologists' Perceptions of Persons With Mental IllnessdsfasdfNo ratings yet
- REStat 2020 Income Shocks and Suicides - Causal Evidence From IndonesiaDocument16 pagesREStat 2020 Income Shocks and Suicides - Causal Evidence From IndonesiaMichelleNo ratings yet
- Prescribing Antipsychotics in Geriatric Patients:: First of 3 PartsDocument8 pagesPrescribing Antipsychotics in Geriatric Patients:: First of 3 PartsAlexRázuri100% (1)
- The Five Senses: A Patient Preference-Based Comparative AnalysisDocument8 pagesThe Five Senses: A Patient Preference-Based Comparative AnalysisasclepiuspdfsNo ratings yet
- BMJ 2023 078084.fullDocument14 pagesBMJ 2023 078084.fulljayswalrameshNo ratings yet
- Masterclass On Grief and LossDocument27 pagesMasterclass On Grief and LosspsychaidconsultsNo ratings yet
- CBT WorkshopDocument52 pagesCBT WorkshopKhoa Le Nguyen100% (13)
- What Is A Mood Stabilizer?: Psychological Medicine June 2007Document7 pagesWhat Is A Mood Stabilizer?: Psychological Medicine June 2007Yulia RestyNo ratings yet
- Increased Screen Time and Its AssociationDocument11 pagesIncreased Screen Time and Its AssociationTiara SekarNo ratings yet