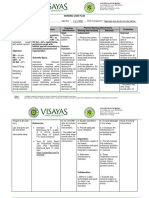
NCP
NCP
Download as doc, pdf, or txt
You might also like
- Machine Design - 1508581959091 PDFDocument67 pagesMachine Design - 1508581959091 PDFEjay Balaba50% (2)
- NCP For HemothoraxDocument12 pagesNCP For Hemothoraxroseonabreeze0% (1)
- NCP Ineffective Airway ClearanceDocument3 pagesNCP Ineffective Airway ClearanceNicholas TagleNo ratings yet
- Assessment Nursing Diagnosis Inference Objectives Nursing Intervention Rationale EvaluationDocument10 pagesAssessment Nursing Diagnosis Inference Objectives Nursing Intervention Rationale EvaluationJobelle Acena100% (2)
- Nursing Care Plan Ineffective Airway Clearance Related To Tracheobronchial Secretions CAPDocument2 pagesNursing Care Plan Ineffective Airway Clearance Related To Tracheobronchial Secretions CAPLP Benoza100% (2)
- CopdDocument6 pagesCopdapi-3717941100% (2)
- Nursing Care Plan Assessment Diagnosis Rationale Planning Intervention Rationale Evaluation IndependentDocument13 pagesNursing Care Plan Assessment Diagnosis Rationale Planning Intervention Rationale Evaluation Independentyanny03No ratings yet
- NCP For CAP TB.Document5 pagesNCP For CAP TB.Cherry Ann BalagotNo ratings yet
- NCP Cap MRDocument2 pagesNCP Cap MREngely Mercader100% (1)
- Bronchial Asthma (Parinas Rhoanne)Document10 pagesBronchial Asthma (Parinas Rhoanne)Carlojay IniegoNo ratings yet
- NCPDocument3 pagesNCPDyanne BautistaNo ratings yet
- NCP For PneumoniaDocument3 pagesNCP For PneumoniaLeogalvez BedanoNo ratings yet
- NCP Difficulties in BreathingDocument4 pagesNCP Difficulties in BreathingKingJayson Pacman06No ratings yet
- Cues Nursing Diagnosis Analysis GOALS and Objectives Nursing Intervention Rationale Evaluation Subjective: GoalDocument4 pagesCues Nursing Diagnosis Analysis GOALS and Objectives Nursing Intervention Rationale Evaluation Subjective: GoalMonica Angelique SalayoNo ratings yet
- Chona NCP 1Document5 pagesChona NCP 1Jan Mark SotoNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument9 pagesAssessment Diagnosis Planning Intervention Rationale EvaluationYzel Vasquez AdavanNo ratings yet
- Impaired Gas Exchange PneumoniaDocument2 pagesImpaired Gas Exchange PneumoniaShanice BedecirNo ratings yet
- Materi Nursing Care PlanDocument1 pageMateri Nursing Care PlanSiti nur Kholifatus samsiyahNo ratings yet
- Ineffective Airway ClearanceDocument6 pagesIneffective Airway ClearanceKarl Angelo MontanoNo ratings yet
- Nursing Care Plan (Pedia)Document5 pagesNursing Care Plan (Pedia)JA BerzabalNo ratings yet
- Assessment Diagnosis Planning Interventions Rationale Evaluation Subjective Data: Short Term Independent: Short TermDocument14 pagesAssessment Diagnosis Planning Interventions Rationale Evaluation Subjective Data: Short Term Independent: Short TermMarlo Dañez NorbeNo ratings yet
- Nursing Care Plan #2:: Assessment Diagnosis Scientific Basis Planning Nursing Interventions Rationale EvaluationDocument4 pagesNursing Care Plan #2:: Assessment Diagnosis Scientific Basis Planning Nursing Interventions Rationale EvaluationGeraldine SantosNo ratings yet
- Piguerra - Week 1 Activty Case Study - Ha Rle 2023to24Document5 pagesPiguerra - Week 1 Activty Case Study - Ha Rle 2023to24kc bpNo ratings yet
- Nursing Care PlanDocument8 pagesNursing Care Planalexander abasNo ratings yet
- Nursing Diagnosis PneumoniaDocument1 pageNursing Diagnosis PneumoniaPasa ShresthaNo ratings yet
- Impaired Gas Exchange NCPDocument4 pagesImpaired Gas Exchange NCPkimglaidyl bontuyanNo ratings yet
- IPPA SampleDocument28 pagesIPPA Samplekimglaidyl bontuyanNo ratings yet
- Nursing Care PlanDocument7 pagesNursing Care Planits niniNo ratings yet
- Alteration in OxygenDocument8 pagesAlteration in OxygenBb RabbitNo ratings yet
- Week 3 - Ms1 Course Task - Cu 3Document2 pagesWeek 3 - Ms1 Course Task - Cu 302 - DIMAYUGA, BRYANNo ratings yet
- NCPDocument3 pagesNCPNikki del Rosario100% (2)
- Task NCPDocument12 pagesTask NCPferdy ilhamNo ratings yet
- NCP - Sta. 6Document2 pagesNCP - Sta. 6vmasalarda2019No ratings yet
- NCP Anaphylactic ShockDocument6 pagesNCP Anaphylactic ShockKirstin del CarmenNo ratings yet
- NCP-Drug Study 2Document4 pagesNCP-Drug Study 2hsiriaNo ratings yet
- Pulmonary Tuberculosis G3Document12 pagesPulmonary Tuberculosis G3Cuttie Anne GalangNo ratings yet
- San Francisco St. Butuan City 8600, Region XIII Caraga, PhilippinesDocument3 pagesSan Francisco St. Butuan City 8600, Region XIII Caraga, Philippineskuro hanabusaNo ratings yet
- NCP#1-Impaired Gas ExchangeDocument2 pagesNCP#1-Impaired Gas ExchangeJoshua Dumanjug SyNo ratings yet
- University of Cordilleras College of Nursing NCP: Mycobacterium TuberculosisDocument3 pagesUniversity of Cordilleras College of Nursing NCP: Mycobacterium TuberculosisLyn MhoreNo ratings yet
- NCPDocument6 pagesNCPJoannabel RodriguezNo ratings yet
- Name and Classification of DrugDocument7 pagesName and Classification of DrugMelrhean GraceNo ratings yet
- Nursing Intervention Diagnose 1 Purpose and Criteria Results Intervention Rational NIC Labels Respiratory MonitoringDocument10 pagesNursing Intervention Diagnose 1 Purpose and Criteria Results Intervention Rational NIC Labels Respiratory MonitoringFhicholy Davied VanrioNo ratings yet
- NCP, Drug StudyDocument9 pagesNCP, Drug StudyTresha CaliboNo ratings yet
- NCP FinalDocument16 pagesNCP FinalEuleen Tria PadrigoNo ratings yet
- Gr.4 NCP Health AssessmentDocument3 pagesGr.4 NCP Health AssessmentAlessandro MadrigalNo ratings yet
- Name: Mr. M AGE: 62 Years Old SEX: Male CC: Persistent Cough Admitting/Working Diagnosis: PnuemoniaDocument3 pagesName: Mr. M AGE: 62 Years Old SEX: Male CC: Persistent Cough Admitting/Working Diagnosis: PnuemoniaMae Therese B. MAGNONo ratings yet
- Assessment Nursing Diagnossis Scientific Basis Goal Nursing Intervention Rationale Evaluation IndependentDocument10 pagesAssessment Nursing Diagnossis Scientific Basis Goal Nursing Intervention Rationale Evaluation IndependentPamela laquindanumNo ratings yet
- NCP Format 3 CKD Chronic Kidney Disease DM Diabetes Mellitus NephropathyDocument4 pagesNCP Format 3 CKD Chronic Kidney Disease DM Diabetes Mellitus NephropathySapna thakur100% (1)
- Assessment Nursing Diagnosis Scientific Rationale Planning Nursing Interventions Rationale EvaluationDocument3 pagesAssessment Nursing Diagnosis Scientific Rationale Planning Nursing Interventions Rationale EvaluationMel Izhra N. MargateNo ratings yet
- Eent Case: Diagnosis: Septic Shock, Pneumonia in Pre Immunocompromised Host, Oropharyngeal CA Stage IVDocument7 pagesEent Case: Diagnosis: Septic Shock, Pneumonia in Pre Immunocompromised Host, Oropharyngeal CA Stage IVYram Yoj ZeraujNo ratings yet
- Nursing Care Plan: Lorma Colleges Con Template Related Learning ExperienceDocument6 pagesNursing Care Plan: Lorma Colleges Con Template Related Learning ExperiencePauline GarciaNo ratings yet
- Nursing Care Plan: Ineffective Breathing Pattern Related ToDocument4 pagesNursing Care Plan: Ineffective Breathing Pattern Related ToFrudz Orjaleza100% (2)
- Final NCP AsthmaDocument5 pagesFinal NCP AsthmaAlexe Nicole BiscanteNo ratings yet
- Covid NCPDocument6 pagesCovid NCPNathalia Cabalse100% (2)
- Assessment Planning Intervention Rationale Evaluation: Nursing DiagnosisDocument2 pagesAssessment Planning Intervention Rationale Evaluation: Nursing DiagnosisLovely CacapitNo ratings yet
- Assessment Nursing Diagnosis Planning Intervention Rationale EvaluationDocument9 pagesAssessment Nursing Diagnosis Planning Intervention Rationale EvaluationKen IgnacioNo ratings yet
- Nursing Care Plan Assessment Data Nursing Diagnosis Scientific Rationale Planning Nursing Interventions Rationale Evaluation IndependentDocument3 pagesNursing Care Plan Assessment Data Nursing Diagnosis Scientific Rationale Planning Nursing Interventions Rationale Evaluation IndependentWyeth Earl Padar EndrianoNo ratings yet
- NCP#2-Ineffective Breathing PatternDocument2 pagesNCP#2-Ineffective Breathing PatternJoshua Dumanjug SyNo ratings yet
- Snoring, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandSnoring, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Your Family Doctor Asthma: Understanding Asthma / Avoiding Allergies / Proper Use of InhalersFrom EverandYour Family Doctor Asthma: Understanding Asthma / Avoiding Allergies / Proper Use of InhalersNo ratings yet
- Problem Set No. 2 PDFDocument2 pagesProblem Set No. 2 PDFRuth MontebonNo ratings yet
- Machine Design Problems 1&2 AlcorconDocument68 pagesMachine Design Problems 1&2 AlcorconRuth Montebon100% (1)
- Statement of The Problem-HYPHOTHESIS-Significance of The Study-Scope and LimitationsDocument4 pagesStatement of The Problem-HYPHOTHESIS-Significance of The Study-Scope and LimitationsRuth MontebonNo ratings yet
- Quiz 3 PDFDocument8 pagesQuiz 3 PDFRuth MontebonNo ratings yet
- Chapter 1: The Problem and A Review of Related Literature RationaleDocument30 pagesChapter 1: The Problem and A Review of Related Literature RationaleRuth MontebonNo ratings yet
- Quiz 2 PDFDocument7 pagesQuiz 2 PDFRuth Montebon0% (1)
- Quiz 1 PDFDocument7 pagesQuiz 1 PDFRuth MontebonNo ratings yet
- Chest Physiotherapy in Paediatric Patients Hospitalised With Community-Acquired Pneumonia: A Randomised Clinical TrialDocument7 pagesChest Physiotherapy in Paediatric Patients Hospitalised With Community-Acquired Pneumonia: A Randomised Clinical Trialaufa memeyNo ratings yet
- Test de Apnea - Neurocritical Care 2021Document13 pagesTest de Apnea - Neurocritical Care 2021Eva SánchezNo ratings yet
- Mechanical Ventilation Troubleshooting Skill Respiratory Therapy COVID 19 Toolkit - 070420Document8 pagesMechanical Ventilation Troubleshooting Skill Respiratory Therapy COVID 19 Toolkit - 070420Sirgut TesfayeNo ratings yet
- Ax PneumothoraxDocument8 pagesAx Pneumothoraxapi-3797941100% (2)
- Understanding Copd-Overlap SyndromesDocument63 pagesUnderstanding Copd-Overlap SyndromesGeorge Cătălin AlexandruNo ratings yet
- I Need A Tissue: A Social Story For AdrianDocument14 pagesI Need A Tissue: A Social Story For AdrianPatricia AquinoNo ratings yet
- Airfit p10 Airfit p10 For Her User Guide Apac EngDocument47 pagesAirfit p10 Airfit p10 For Her User Guide Apac EngjannguidoNo ratings yet
- ADRIANO BONDOC ORSOLINO VIADOR - Docx 1Document10 pagesADRIANO BONDOC ORSOLINO VIADOR - Docx 1Luis LazaroNo ratings yet
- Oxygen InsufficiencyDocument16 pagesOxygen Insufficiencydeolzf100% (1)
- Dupilumab COPD NEJMDocument10 pagesDupilumab COPD NEJM5fqkqkcdhtNo ratings yet
- Introduction To Pediatric VentilationDocument41 pagesIntroduction To Pediatric Ventilationedderj2585No ratings yet
- Obstructive Pulmonary DiseasesDocument50 pagesObstructive Pulmonary DiseasesGopala HariNo ratings yet
- Chapter 23 Obstructive Lung Disease Chronic Obstructive Pulmonary DiseaseDocument10 pagesChapter 23 Obstructive Lung Disease Chronic Obstructive Pulmonary DiseaseZahra Margrette SchuckNo ratings yet
- Air Travel and PneumothorakDocument7 pagesAir Travel and PneumothorakRojullun TaufikNo ratings yet
- AUS PEEPValves 493480097 V02 0712Document2 pagesAUS PEEPValves 493480097 V02 0712paniyaNo ratings yet
- Thoracic TraumaDocument24 pagesThoracic TraumaBibaswan ChakrabartyNo ratings yet
- نيومومياDocument1 pageنيومومياMohamed AlsaabNo ratings yet
- PA500 Medical Ventilator: Superior Ventilation From ExperienceDocument11 pagesPA500 Medical Ventilator: Superior Ventilation From ExperienceYesy NurNo ratings yet
- Endotracheal IntubationDocument2 pagesEndotracheal Intubationedison aorianoNo ratings yet
- Ventilator Graphics.Document69 pagesVentilator Graphics.LauraAlvarezMulett100% (3)
- Care of The Clients With Respiratory DisordersDocument10 pagesCare of The Clients With Respiratory Disordersdexter100% (3)
- Transient Tachypnea of The Newborn (TTN)Document6 pagesTransient Tachypnea of The Newborn (TTN)Wivan Havilian DjohanNo ratings yet
- Health-Problems 2 - 63706Document1 pageHealth-Problems 2 - 63706Lyudmila VergunNo ratings yet
- Asthma: Setya Puspa Dewi AprilyaniDocument19 pagesAsthma: Setya Puspa Dewi Aprilyaninadia kurnia100% (3)
- Automation of Mechanical VentilationDocument12 pagesAutomation of Mechanical VentilationjuanNo ratings yet
- Artikel Ilmiah - Nov Dion FuadillahDocument13 pagesArtikel Ilmiah - Nov Dion FuadillahNov Dion FuadillahNo ratings yet
- Idiopathic Pulmonary Fibrosis NEWDocument34 pagesIdiopathic Pulmonary Fibrosis NEWrahayuNo ratings yet
- Activity 3 DindaDocument7 pagesActivity 3 DindaOktaviana Ronauli MarbunNo ratings yet
- Body Plethysmography AvneetDocument54 pagesBody Plethysmography Avneetsalimtajamul100% (3)
- Drug Study AmbroxolDocument2 pagesDrug Study AmbroxolBelle MakinanoNo ratings yet