Article 1552613421 PDF
Article 1552613421 PDF
Download as pdf or txt
You might also like
- Neurology Multiple Choice Questions With Explanations: Volume IIFrom EverandNeurology Multiple Choice Questions With Explanations: Volume IIRating: 5 out of 5 stars5/5 (2)
- OET Writing SampleDocument4 pagesOET Writing SampleAnganaNo ratings yet
- Human Malformations - 11 - NoseDocument17 pagesHuman Malformations - 11 - NoseAhmed H. Ali ElbestaweyNo ratings yet
- MenereDocument11 pagesMenereJauhari JoNo ratings yet
- 538 540 (Jos)Document3 pages538 540 (Jos)Anonymous ATdLPZNo ratings yet
- The Etiology of Bell's Palsy: A Review: Wenjuan Zhang Lei Xu Tingting Luo Feng Wu Bin Zhao Xianqi LiDocument10 pagesThe Etiology of Bell's Palsy: A Review: Wenjuan Zhang Lei Xu Tingting Luo Feng Wu Bin Zhao Xianqi LiayuNo ratings yet
- Zhang2019 Article TheEtiologyOfBellSPalsyAReview PDFDocument10 pagesZhang2019 Article TheEtiologyOfBellSPalsyAReview PDFYamile AbadiaNo ratings yet
- Obstructive Sleep Apnea: An Overview On Features, Diagnosis & Orthodontic ManagementDocument6 pagesObstructive Sleep Apnea: An Overview On Features, Diagnosis & Orthodontic Managementsajida khanNo ratings yet
- 9d7f PDFDocument4 pages9d7f PDFMubarak HazaziNo ratings yet
- Otolaryngol - Head Neck Surg - 2021 - Cantarella - The Bicentenary of Bell S Description of The Neuroanatomical Basis ofDocument3 pagesOtolaryngol - Head Neck Surg - 2021 - Cantarella - The Bicentenary of Bell S Description of The Neuroanatomical Basis ofโสภาพรรณวดี รวีวารNo ratings yet
- Paralisis FacialDocument4 pagesParalisis FacialFabian Orozco SánchezNo ratings yet
- Polyganglionitis Episodica (PGE) : The New Concept For Viral Polyganglionitis of The Head and NeckDocument25 pagesPolyganglionitis Episodica (PGE) : The New Concept For Viral Polyganglionitis of The Head and Neck0007 AndrezaNo ratings yet
- Raeders SyndromeDocument6 pagesRaeders SyndromeSundayperfectNo ratings yet
- Bilateral Facial Nerve (Bells) Palsy in A 24-Year-Old WomanDocument3 pagesBilateral Facial Nerve (Bells) Palsy in A 24-Year-Old WomanmimicamasoNo ratings yet
- Bilateral Facial Nerve (Bell's) Palsy in A 24-Year-Old Woman: A Case ReportDocument3 pagesBilateral Facial Nerve (Bell's) Palsy in A 24-Year-Old Woman: A Case Reportokto namikaNo ratings yet
- The Special Senses - Clinical CorrelatesDocument4 pagesThe Special Senses - Clinical Correlatesalecsandra96No ratings yet
- Bell's Palsy PresentasiDocument20 pagesBell's Palsy PresentasiIda AmsiyatiNo ratings yet
- Prosthodontic Rehabilitation of Patients With Bell PDFDocument5 pagesProsthodontic Rehabilitation of Patients With Bell PDFLakshmi Sarvani ValluriNo ratings yet
- Ijcmr 3499Document4 pagesIjcmr 3499AlfirahmatikaNo ratings yet
- Systemic Lupus Erythematosus and Hearing Disorders: Literature Review and Meta-Analysis of Clinical and Temporal Bone FindingsDocument11 pagesSystemic Lupus Erythematosus and Hearing Disorders: Literature Review and Meta-Analysis of Clinical and Temporal Bone FindingsLNo ratings yet
- mooneAMS 3 66Document6 pagesmooneAMS 3 66dikiprestya391No ratings yet
- Bell's Palsy: Pathogenesis, Clinical Features, and Diagnosis in AdultsDocument16 pagesBell's Palsy: Pathogenesis, Clinical Features, and Diagnosis in AdultsAmada Angel VillanuevaNo ratings yet
- AMEER^L120OMRDocument49 pagesAMEER^L120OMRmohammedameersha2001No ratings yet
- 3 PBDocument9 pages3 PBmitchelNo ratings yet
- Bell'S Palsy-A Psychologically Distressing Condition-Overview of LiteratureDocument13 pagesBell'S Palsy-A Psychologically Distressing Condition-Overview of LiteratureheidyNo ratings yet
- A Case Report of Paget's Disease of Bone Involving Maxilla and Mandible: A Diagnostic DilemmaDocument8 pagesA Case Report of Paget's Disease of Bone Involving Maxilla and Mandible: A Diagnostic DilemmaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- chlampah,+MEDICAL REHABILITATION IN PATIENT WITH RIGHT PERIPHERAL FACIAL NERVE+Document7 pageschlampah,+MEDICAL REHABILITATION IN PATIENT WITH RIGHT PERIPHERAL FACIAL NERVE+Princess BubblegumNo ratings yet
- Bells PalsyDocument6 pagesBells PalsyElisabeth TikalakaNo ratings yet
- Recurrent Facial Nerve Paresis in A Child With Chronic Otitis Media With EffusionDocument3 pagesRecurrent Facial Nerve Paresis in A Child With Chronic Otitis Media With Effusionfarah maulida martaNo ratings yet
- CH69Document4 pagesCH69Almeiliana Arruanpasau'No ratings yet
- Paralisis de Bell PDFDocument10 pagesParalisis de Bell PDFCarlos Andrés Barrera ParraNo ratings yet
- Ehlers Danlos Syndrome Associated With Cleft Lip and PalateDocument3 pagesEhlers Danlos Syndrome Associated With Cleft Lip and PalateelmancuernoNo ratings yet
- The FACIAL NERVE Current Trends in Diagnosis, Treatment, and RehabilitationDocument17 pagesThe FACIAL NERVE Current Trends in Diagnosis, Treatment, and RehabilitationkrazeedoctorNo ratings yet
- Anatomy of the Epicanthal FoldDocument2 pagesAnatomy of the Epicanthal Foldlibrarian.blrNo ratings yet
- Craniofacial Deformities Review of Etiologies Distribution and TDocument16 pagesCraniofacial Deformities Review of Etiologies Distribution and TambersNo ratings yet
- The Face-Neurosensory Perspective)Document10 pagesThe Face-Neurosensory Perspective)RobertoNo ratings yet
- Ewings Sarcoma of The Mandible A Rare Case ReportDocument4 pagesEwings Sarcoma of The Mandible A Rare Case Reportsyed ahmedNo ratings yet
- Peters Anomaly An OverviewDocument9 pagesPeters Anomaly An Overviewdbk556n7qsNo ratings yet
- Meige's Disease A Clinical Form of Facial Convulsion, BilateralDocument3 pagesMeige's Disease A Clinical Form of Facial Convulsion, BilateralBruce Fredy Chino ChambillaNo ratings yet
- v10 Literature Review Auricular Disorders Part 1 Physical and Thermal Change Related TraumasDocument6 pagesv10 Literature Review Auricular Disorders Part 1 Physical and Thermal Change Related TraumasAlisNo ratings yet
- Jurnal Saraf 5Document5 pagesJurnal Saraf 5Suci MayveraNo ratings yet
- Jps R 07111519Document3 pagesJps R 07111519Riuin23No ratings yet
- A Case Series of Tessier 3, 4, 7 and Combined 4, 7 Craniofacial CleftsDocument5 pagesA Case Series of Tessier 3, 4, 7 and Combined 4, 7 Craniofacial CleftsMohammad Wildan Hari SHNo ratings yet
- Craniofacial Syndromes.33Document26 pagesCraniofacial Syndromes.33andrew kilshawNo ratings yet
- Oral Medicine 8Document8 pagesOral Medicine 8abdulrazaqNo ratings yet
- Neurology Bell'S Palsy: by Group 1Document22 pagesNeurology Bell'S Palsy: by Group 1Rizky AmaLia Ar-RosyidNo ratings yet
- Anancephaly 2Document3 pagesAnancephaly 2Metta SariNo ratings yet
- SX HornerDocument5 pagesSX HornermariferNo ratings yet
- Annular Alopecia Areata: Report of Two CasesDocument4 pagesAnnular Alopecia Areata: Report of Two CasesZAHYRA MARÍA VALDERRAMA POLANIANo ratings yet
- Bells Palsy TutorialDocument19 pagesBells Palsy Tutorialhessty100% (2)
- Auriculo Condylar Syndrome - A Case Report With Differential DiagnosisDocument6 pagesAuriculo Condylar Syndrome - A Case Report With Differential DiagnosisbrijeshsNo ratings yet
- Book Reviews: Diagnostic Handbook of OtorhinolaryngologyDocument1 pageBook Reviews: Diagnostic Handbook of OtorhinolaryngologyVernika AngelinaNo ratings yet
- Satoyoshi Syndrome - A Case Report From India: Venkatraman Mani MD - Renu George MDDocument3 pagesSatoyoshi Syndrome - A Case Report From India: Venkatraman Mani MD - Renu George MDEmrah AĞDERENo ratings yet
- Osa OrthopaedicsDocument13 pagesOsa OrthopaedicsJustin KimberlakeNo ratings yet
- The Apert and Crouzon Syndromes: General and Dental Aspects and Management in Orthodontics and Dentofacial Orthopaedics: A Review ArticleDocument10 pagesThe Apert and Crouzon Syndromes: General and Dental Aspects and Management in Orthodontics and Dentofacial Orthopaedics: A Review ArticleOral DentNo ratings yet
- Herpes Zoster Lyme Disease Syphilis Epstein-Barr Viral Infection Cytomegalovirus HIV Mycoplasma Diabetes Mellitus HypertensionDocument14 pagesHerpes Zoster Lyme Disease Syphilis Epstein-Barr Viral Infection Cytomegalovirus HIV Mycoplasma Diabetes Mellitus HypertensionShasha ShakinahNo ratings yet
- Anatomical Classification of Facial, Cranio-Facial and Latero-Facial CleftsDocument24 pagesAnatomical Classification of Facial, Cranio-Facial and Latero-Facial CleftsAlvaro Jose Uribe TamaraNo ratings yet
- A Diagnostic Conundrum Prac Neuro 2017Document7 pagesA Diagnostic Conundrum Prac Neuro 2017Goh Jin YiNo ratings yet
- 2011 TourenoDocument6 pages2011 TourenoazizhamoudNo ratings yet
- Unilateral Facial Palsy in Two Dogs-A Report: The Indian Veterinary Journal December 2018Document3 pagesUnilateral Facial Palsy in Two Dogs-A Report: The Indian Veterinary Journal December 2018MahdawwNo ratings yet
- The New Neurotology: A Comprehensive Clinical GuideFrom EverandThe New Neurotology: A Comprehensive Clinical GuideNo ratings yet
- Prosthetic Rehabilitation Using Extra Coronal Attachments: Case ReportDocument4 pagesProsthetic Rehabilitation Using Extra Coronal Attachments: Case ReportLakshmi Sarvani ValluriNo ratings yet
- Chairside Technique For Expediting Indirect Interim RestorationsDocument2 pagesChairside Technique For Expediting Indirect Interim RestorationsLakshmi Sarvani ValluriNo ratings yet
- Keith1982 PDFDocument8 pagesKeith1982 PDFLakshmi Sarvani ValluriNo ratings yet
- Growthof Nasomaxillarycomplex FinalDocument99 pagesGrowthof Nasomaxillarycomplex FinalLakshmi Sarvani ValluriNo ratings yet
- 2 4 4Document3 pages2 4 4Lakshmi Sarvani ValluriNo ratings yet
- Prosthodontic Rehabilitation of Patients With Bell PDFDocument5 pagesProsthodontic Rehabilitation of Patients With Bell PDFLakshmi Sarvani ValluriNo ratings yet
- Cesarean Delivery: Postoperative Issues - UpToDateDocument12 pagesCesarean Delivery: Postoperative Issues - UpToDateZurya UdayanaNo ratings yet
- Case Study Jim SandersonDocument6 pagesCase Study Jim SandersonJessica McAlexanderNo ratings yet
- Pelvic ExaminationDocument3 pagesPelvic ExaminationAdisorn ChaikitNo ratings yet
- Pedo QsDocument13 pagesPedo QsGaYda'a Kana'anNo ratings yet
- "Central Giant Cell Granuloma" - An Update: Invited ReviewDocument3 pages"Central Giant Cell Granuloma" - An Update: Invited ReviewPrapu RamNo ratings yet
- Pulmonary Vascular DiseaseDocument4 pagesPulmonary Vascular DiseaseSaima JabbarNo ratings yet
- Prepared By: ASMA M A First M.Pharm PharmacologyDocument25 pagesPrepared By: ASMA M A First M.Pharm Pharmacologyhumag143100% (1)
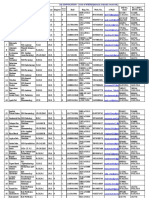
- Rs. 2,500 / DD No.-Date Rs. 2,000 / DD No.-Date: 5th CONVOCATION - 2016 of WBUHS (Details of Drafts Received)Document66 pagesRs. 2,500 / DD No.-Date Rs. 2,000 / DD No.-Date: 5th CONVOCATION - 2016 of WBUHS (Details of Drafts Received)Kriti KumariNo ratings yet
- Surgery Extra NotesDocument2 pagesSurgery Extra NotesrohalawiNo ratings yet
- Acupuncture For InfertilityDocument6 pagesAcupuncture For InfertilityflaviobpjrNo ratings yet
- Vital SignsDocument8 pagesVital SignsTempoNo ratings yet
- CharterMedical - Cell-FreezeDocument10 pagesCharterMedical - Cell-FreezeCampaign MediaNo ratings yet
- Fraktur UmumDocument94 pagesFraktur UmumrhinyNo ratings yet
- Ch05 Nutrition and Theories of AgingDocument98 pagesCh05 Nutrition and Theories of AgingKeersee CacayuranNo ratings yet
- MCQ Part 1 2003Document2 pagesMCQ Part 1 2003Jhonn NaiseNo ratings yet
- Guidewires and Micro CathetersDocument34 pagesGuidewires and Micro CathetersDivyeshNo ratings yet
- UntitledDocument663 pagesUntitledAna Beatriz Medeiros100% (1)
- Am J Clin Nutr 1979 Anderson 2312 21Document10 pagesAm J Clin Nutr 1979 Anderson 2312 21Riza Haida WardhaniNo ratings yet
- Jointly Team: SMLE GroupDocument22 pagesJointly Team: SMLE GroupAkpevwe EmefeNo ratings yet
- Types of Classrooms in Special EducationDocument3 pagesTypes of Classrooms in Special EducationMaaz KhanNo ratings yet
- Eltrombopag en DengueDocument8 pagesEltrombopag en DengueJ Isaac VelazquezNo ratings yet
- Sri SuryoDocument6 pagesSri SuryoFiLiOeiNo ratings yet
- Sonopuls 692 6-Series User ManualDocument107 pagesSonopuls 692 6-Series User ManualMaryam BushraNo ratings yet
- Acute and Chronic DiseasesDocument13 pagesAcute and Chronic DiseasesAchyut AryanNo ratings yet
- Infected Blister How To Tell & What To Do About It - Blister PreventionDocument1 pageInfected Blister How To Tell & What To Do About It - Blister Preventiondashielleadelaide18No ratings yet
- Shabad Beliefsabout Causesof Depression TDSJCL2011Document12 pagesShabad Beliefsabout Causesof Depression TDSJCL2011zulfikarfuadiNo ratings yet
- Co-Tle 8Document19 pagesCo-Tle 8janine100% (1)
- EssenInterMed ChurLivin (Rinconmedico - Me) PDFDocument832 pagesEssenInterMed ChurLivin (Rinconmedico - Me) PDFLuis Armando Buenaventura100% (1)
- Rapid AssesmentDocument2 pagesRapid AssesmentgtsantosNo ratings yet