Neuro Psych - Antiepileptic Drug Chart
Neuro Psych - Antiepileptic Drug Chart
Download as pdf or txt
At a glance
Powered by AI
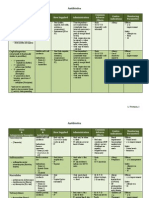
The document discusses various anti-epileptic drugs including their mechanisms of action, indications, dosing, side effects and pharmacokinetics.
The main mechanisms of action discussed include sodium channel blockade, potentiation of GABA, inhibition of GABA transaminase and enhancement of potassium currents.
Common side effects include dizziness, headache, nausea, sedation, ataxia and fatigue.
You might also like
- Simman 2024Document54 pagesSimman 2024Doshi SahilNo ratings yet
- Heart Failure Topic DiscussionDocument11 pagesHeart Failure Topic Discussionapi-665372449100% (1)
- Top 300 Drugs Pocket Reference Guide (2021 Edition)From EverandTop 300 Drugs Pocket Reference Guide (2021 Edition)Rating: 5 out of 5 stars5/5 (1)
- Antibiotics Study Guide For NursesDocument3 pagesAntibiotics Study Guide For NursesLauren Trotman100% (7)
- AP Biology Cheat Sheet PDFDocument7 pagesAP Biology Cheat Sheet PDFJ15No ratings yet
- Infectious Diseases IDocument7 pagesInfectious Diseases ITiff VoNo ratings yet
- Antiarrhythmic Medication Chart - EBM Consult v3Document2 pagesAntiarrhythmic Medication Chart - EBM Consult v3Linlin100% (1)
- Lang 10 EditionDocument235 pagesLang 10 Editionraju niraulaNo ratings yet
- Lange Smart Charts: Pharmacology, 2e Pharmacologic SuffixesDocument2 pagesLange Smart Charts: Pharmacology, 2e Pharmacologic SuffixesSolNo ratings yet
- Neurology QuestionsDocument58 pagesNeurology QuestionsMonica J Ortiz Pereira100% (2)
- NCP HypertensionDocument2 pagesNCP Hypertensionsinister1781% (27)
- Appleton - Obstetrics and GinecologyDocument306 pagesAppleton - Obstetrics and GinecologyFajar Raharja50% (2)
- Example Project ProposalDocument20 pagesExample Project ProposalAbid Hossain Apu100% (1)
- PCOL Maps PDFDocument11 pagesPCOL Maps PDFZinc YuloNo ratings yet
- A-Autonomic Drugs: 1) CholinergicDocument28 pagesA-Autonomic Drugs: 1) CholinergicMahmoud Ahmed MahmoudNo ratings yet
- Chart Antibacterial Drugs PDFDocument1 pageChart Antibacterial Drugs PDFMunaf AlsumaryNo ratings yet
- Total Pharmacy Notes TPN For EEDocument1,601 pagesTotal Pharmacy Notes TPN For EEClaire Cura100% (2)
- Drug of Choice and First Line of TreatmentDocument2 pagesDrug of Choice and First Line of Treatmentprinz1mendezNo ratings yet
- Pain and Inflammation Med ChartsDocument4 pagesPain and Inflammation Med Chartssurviving nursing school100% (1)
- A New Way of Mnemonics - Hypertension-cough-asthma-NSAID - WMDocument26 pagesA New Way of Mnemonics - Hypertension-cough-asthma-NSAID - WMKartik Mendiratta100% (1)
- Different Body Receptors PDFDocument1 pageDifferent Body Receptors PDFSantosh patelNo ratings yet
- Respiratory System: Antiasthmatic Drugs Cardiac GlycosidesDocument4 pagesRespiratory System: Antiasthmatic Drugs Cardiac GlycosidesNurse Hooman100% (1)
- Top 200 Expanded 1Document27 pagesTop 200 Expanded 1Dean HarperNo ratings yet
- Pharmacology of Cardiac Diseases MINEDocument3 pagesPharmacology of Cardiac Diseases MINEMitu Miressa ت100% (1)
- Drug of Choice in Various Diseases - Candidiasis - PharmacologyDocument1 pageDrug of Choice in Various Diseases - Candidiasis - PharmacologyPragnesh ParmarNo ratings yet
- Drug Side EffectsDocument2 pagesDrug Side EffectsAngelic khanNo ratings yet
- BED12 - Antibiotics PharmacologyDocument2 pagesBED12 - Antibiotics PharmacologyAmir AmirulNo ratings yet
- Microbiology Step 1 Antimicrobials ChartDocument6 pagesMicrobiology Step 1 Antimicrobials ChartM Patel100% (1)
- Confuseddrugnames 201902Document11 pagesConfuseddrugnames 201902Detya PertiwiNo ratings yet
- Pharmacology Drug Chart: Drug Name Receptor Therapeutic Uses Adverse EffectsDocument18 pagesPharmacology Drug Chart: Drug Name Receptor Therapeutic Uses Adverse EffectsPadmavathy Naidu Chokkapu100% (2)
- TLDR HIV Cheat Sheet v2Document1 pageTLDR HIV Cheat Sheet v2AisleenHNo ratings yet
- Inhibit Clasification Antibiotics: (Broad Spectrum) (Narrow Spectrum)Document1 pageInhibit Clasification Antibiotics: (Broad Spectrum) (Narrow Spectrum)SY WongNo ratings yet
- 2023 RxPrep NAPLEX Course Book Mnemonics and PearlsDocument7 pages2023 RxPrep NAPLEX Course Book Mnemonics and PearlsfelixkaharaNo ratings yet
- Hmg-Coa Reductase Inhibitors (Statins) : Side Effects, Contraindications, InteractionsDocument6 pagesHmg-Coa Reductase Inhibitors (Statins) : Side Effects, Contraindications, Interactionswaste78No ratings yet
- Gout DrugsDocument1 pageGout DrugsMichael BrownNo ratings yet
- Respiratory DrugsDocument2 pagesRespiratory Drugsmed testNo ratings yet
- Ninja - Anti-HTN PDFDocument6 pagesNinja - Anti-HTN PDFErica Hyeyeon Lee100% (2)
- Beta Lactam AntibioticsDocument1 pageBeta Lactam AntibioticsCourtney TownsendNo ratings yet
- Drug of ChoiceDocument5 pagesDrug of ChoiceAsmaa Radwan100% (1)
- Central Nervous System: Drug of Choices Notes - Kent Andrei Paelma Bsn-2FDocument22 pagesCentral Nervous System: Drug of Choices Notes - Kent Andrei Paelma Bsn-2FOfficially RandomNo ratings yet
- Drugclasses Pharmacologypart 1 PDFDocument25 pagesDrugclasses Pharmacologypart 1 PDFSutanya100% (3)
- KDT Only ClassificationsDocument72 pagesKDT Only ClassificationsDebashis ParidaNo ratings yet
- Abx FinalDocument3 pagesAbx Finalyanks1120No ratings yet
- OTC Exam 2 Study GuideDocument32 pagesOTC Exam 2 Study GuideDave WinNo ratings yet
- Top 200 Drug ExamDocument1 pageTop 200 Drug ExamUyen V. NguyenNo ratings yet
- NAPLEX 2023 Quick GuidesDocument76 pagesNAPLEX 2023 Quick Guidesyaksha9100% (1)
- Drug TerminologyDocument5 pagesDrug Terminologyimdaking123No ratings yet
- Pharmacology Quick HitsDocument6 pagesPharmacology Quick HitsHuma Hameed DogarNo ratings yet
- AnalgesicDocument2 pagesAnalgesicLA BriguelaNo ratings yet
- Top 200 Drug Study Reference RLPDocument31 pagesTop 200 Drug Study Reference RLPYathrika Yathrika100% (1)
- Introduction To Pharmacology AntibioticDocument15 pagesIntroduction To Pharmacology AntibioticZaira Reine Santos100% (1)
- Kaplan Notes. ExamenSO IMPORTANTDocument145 pagesKaplan Notes. ExamenSO IMPORTANTLisaNo ratings yet
- Antibiotics - Pathogen ChartDocument3 pagesAntibiotics - Pathogen ChartYanling Li100% (2)
- Pharm Drug Outline AdrDocument1 pagePharm Drug Outline AdrCess Lagera YbanezNo ratings yet
- Warfarin Sodium: INR Levels 4.0 or Less Ok To Carry Out Procedure Test Atleast 72 Hrs Prior To ProcedureDocument6 pagesWarfarin Sodium: INR Levels 4.0 or Less Ok To Carry Out Procedure Test Atleast 72 Hrs Prior To ProcedureVimi GeorgeNo ratings yet
- RX Cheat Sheet Pharmacy CrackDocument1 pageRX Cheat Sheet Pharmacy Crackramesh kumar100% (1)
- Drug Interactions 2 Paper PDFDocument2 pagesDrug Interactions 2 Paper PDFAzima AbdelrhamanNo ratings yet
- Brand Generic Class Other: NAPLEX ReviewDocument72 pagesBrand Generic Class Other: NAPLEX Reviewbapimirab654No ratings yet
- IV PO Conversion CAPDocument3 pagesIV PO Conversion CAPdamondouglasNo ratings yet
- DiazepamDocument1 pageDiazepamIvanne Hisoler71% (7)
- Activity 2 Drug Study LinaoDocument21 pagesActivity 2 Drug Study LinaoNursing ClassNo ratings yet
- ANALGETIKDocument32 pagesANALGETIKshofa nur rahmannisaNo ratings yet
- 6 MAGNESIUM SULFATE Drug StudyDocument2 pages6 MAGNESIUM SULFATE Drug StudyGwyn Rosales100% (2)
- Lui Sh-Colored Lips and Finger Nails Blur Red VisionDocument1 pageLui Sh-Colored Lips and Finger Nails Blur Red VisionMagdayao Romamea100% (1)
- Magnesium SulfateDocument2 pagesMagnesium SulfateGwyn Rosales100% (1)
- Drug Study Analgesics AcetaminophenDocument2 pagesDrug Study Analgesics AcetaminophenGwyneth SantiagoNo ratings yet
- Mov22. Hyperkinetic Disorders 3 (Tics, Myoclonus, Other)Document6 pagesMov22. Hyperkinetic Disorders 3 (Tics, Myoclonus, Other)Monica J Ortiz PereiraNo ratings yet
- The Basic Science of Articular Cartilage: Structure, Composition, and FunctionDocument8 pagesThe Basic Science of Articular Cartilage: Structure, Composition, and FunctionMonica J Ortiz PereiraNo ratings yet
- Gastroenterology - Pancreatitis PDFDocument2 pagesGastroenterology - Pancreatitis PDFMonica J Ortiz PereiraNo ratings yet
- Gastroenterology - Malabsorption PDFDocument1 pageGastroenterology - Malabsorption PDFMonica J Ortiz PereiraNo ratings yet
- Gastroenterology - Pancreatitis PDFDocument2 pagesGastroenterology - Pancreatitis PDFMonica J Ortiz PereiraNo ratings yet
- Cancer Trials Terminology Study Design StatsDocument3 pagesCancer Trials Terminology Study Design StatsMonica J Ortiz PereiraNo ratings yet
- Neurosyphilis: Pathology, Clinical FeaturesDocument6 pagesNeurosyphilis: Pathology, Clinical FeaturesMonica J Ortiz PereiraNo ratings yet
- Generic Name Brand Name Abbreviation: © 2017 Find Your Script HIV Medications - Drug Names Quick SheetDocument1 pageGeneric Name Brand Name Abbreviation: © 2017 Find Your Script HIV Medications - Drug Names Quick SheetMonica J Ortiz PereiraNo ratings yet
- Vitamins: Endocrine System, Metabolism: VitaminsDocument25 pagesVitamins: Endocrine System, Metabolism: VitaminsMonica J Ortiz PereiraNo ratings yet
- Nephrology MCQ PDFDocument7 pagesNephrology MCQ PDFMonica J Ortiz PereiraNo ratings yet
- Usmlestep2cs 2Document100 pagesUsmlestep2cs 2Monica J Ortiz PereiraNo ratings yet
- Note. Includes Dietary and Supplemental Nutrition IntakeDocument5 pagesNote. Includes Dietary and Supplemental Nutrition IntakeMonica J Ortiz PereiraNo ratings yet
- p1w1 Nur149 Session 1Document75 pagesp1w1 Nur149 Session 1Alliah Marie CababarosNo ratings yet
- Lodi Junqueira2018Document2 pagesLodi Junqueira2018lilamedstudNo ratings yet
- General Pharmacology NotesDocument67 pagesGeneral Pharmacology NotesZehra KhanNo ratings yet
- Wessely's Way: Rhetoric or Reason? Malcolm Hooper Margaret Williams 22 March 2008Document23 pagesWessely's Way: Rhetoric or Reason? Malcolm Hooper Margaret Williams 22 March 2008fbomxdijzyorNo ratings yet
- KLIMAKTHEELDocument4 pagesKLIMAKTHEELDuvan Trilleras100% (1)
- Table of Common Human PATHOGENS - Name, Type, Disease, Tissue, Method of Transmission, Virulence Factors, Normal Habitat, and TreatmentDocument3 pagesTable of Common Human PATHOGENS - Name, Type, Disease, Tissue, Method of Transmission, Virulence Factors, Normal Habitat, and TreatmentweslynnesmithNo ratings yet
- Asbestos: From Wikipedia, The Free Encyclopedia Jump To:, For Other Uses, SeeDocument26 pagesAsbestos: From Wikipedia, The Free Encyclopedia Jump To:, For Other Uses, SeeSonorizari BrasovNo ratings yet
- Case Scenarios: Scenario 1Document2 pagesCase Scenarios: Scenario 1Kym RonquilloNo ratings yet
- Tle 10Document3 pagesTle 10Aldrin BagasinaNo ratings yet
- Corona Virus Disease (COVID-19)Document3 pagesCorona Virus Disease (COVID-19)Saya KenzaNo ratings yet
- CMBEBIH 2017 Proceedings of The International Conference On Medical and Biological Engineering 2017 1st Edition Almir Badnjevic (Eds.)Document62 pagesCMBEBIH 2017 Proceedings of The International Conference On Medical and Biological Engineering 2017 1st Edition Almir Badnjevic (Eds.)sliszheeyaet100% (4)
- Lesson Plan On HELLP Syndrome: SGT University Faculty of NursingDocument14 pagesLesson Plan On HELLP Syndrome: SGT University Faculty of Nursingajnesh100% (1)
- Fluid Balance in Clinical PracticeDocument8 pagesFluid Balance in Clinical Practicefernando_vaz2010100% (1)
- Modern Materials ChemicalsDocument19 pagesModern Materials ChemicalsUsama Majid100% (1)
- Baby BathDocument7 pagesBaby BathHamzedNo ratings yet
- PCMDocument4 pagesPCMMADHUMITHA VEMULANo ratings yet
- ChitnisDocument1 pageChitnisAkash Dhiman100% (1)
- History Collection and Physical Examination Kardex Nurses Notes PDFDocument53 pagesHistory Collection and Physical Examination Kardex Nurses Notes PDFSalma SultanaNo ratings yet
- Wessex Neuro ICU GuidelinesDocument200 pagesWessex Neuro ICU GuidelinesJVSP Servicos Medicos LTDANo ratings yet
- Pregnancy and Lactation AnswersDocument8 pagesPregnancy and Lactation AnswersAoiNo ratings yet
- Fonc 11 808721Document7 pagesFonc 11 808721Bruno MendesNo ratings yet
- Biological Warfare Attack, Diagnosis, TreatmentDocument41 pagesBiological Warfare Attack, Diagnosis, Treatmentapi-3695725No ratings yet
- Case Study 17Document5 pagesCase Study 17api-27655178367% (3)
- Age-Related Variations in Global Spinal Alignment and Sagittal Balance in Asymptomatic Japanese AdultsDocument6 pagesAge-Related Variations in Global Spinal Alignment and Sagittal Balance in Asymptomatic Japanese AdultsDr.Khalid GhaznaviNo ratings yet
- Obesity and DiabetesDocument41 pagesObesity and DiabetesHuzaifa KhanNo ratings yet