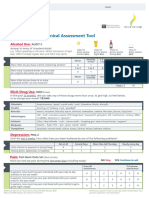
Appenjix A. Study Measures and Self-Report Questionnaires
Appenjix A. Study Measures and Self-Report Questionnaires
Download as docx, pdf, or txt
You might also like
- Hazel Don Step 1Document7 pagesHazel Don Step 1miller22100% (1)
- Alcohol and You - How to Control and Stop Drinking: Stop Drinking BooksFrom EverandAlcohol and You - How to Control and Stop Drinking: Stop Drinking BooksNo ratings yet
- Alcohol Audit Screening Tool mk4Document2 pagesAlcohol Audit Screening Tool mk4joey100% (1)
- Product Information: 2C-B (Hydrochloride)Document1 pageProduct Information: 2C-B (Hydrochloride)Captain KaswanNo ratings yet
- Audit: The Alcohol Use Disorders Identification Test: Self-Report VersionDocument2 pagesAudit: The Alcohol Use Disorders Identification Test: Self-Report Versionkrittika psychologistNo ratings yet
- AUDIT DASHscreeningtoolsDocument6 pagesAUDIT DASHscreeningtoolscarolineNo ratings yet
- Substance Use CompiledDocument2 pagesSubstance Use CompiledRaghuram MiryalaNo ratings yet
- Substance Use CompiledDocument2 pagesSubstance Use CompiledRaghuram MiryalaNo ratings yet
- AUDIT-Questionnaire ( Modified )_backupDocument2 pagesAUDIT-Questionnaire ( Modified )_backupDevashish PatelNo ratings yet
- Substance Use/Misuse Screening and Assessment ToolsDocument2 pagesSubstance Use/Misuse Screening and Assessment ToolsAmel EzNo ratings yet
- AUDIT-Questionnaire ( Modified )Document2 pagesAUDIT-Questionnaire ( Modified )Devashish PatelNo ratings yet
- Screening ToolDocument2 pagesScreening Toolapi-475764290No ratings yet
- Alcohol Abuse and Alcoholism Test - AUDIT ScreenDocument1 pageAlcohol Abuse and Alcoholism Test - AUDIT ScreenJeffrey ManzanoNo ratings yet
- AUDITDocument2 pagesAUDITRoel AbricaNo ratings yet
- AuditDocument4 pagesAuditshakyaNo ratings yet
- Alcohol Use Disorders Identification Test AUDIT For PrintDocument2 pagesAlcohol Use Disorders Identification Test AUDIT For PrintSuadNo ratings yet
- Fast Alcohol Use Screening Test FASTDocument3 pagesFast Alcohol Use Screening Test FASTUtkarsh ShahiNo ratings yet
- Test AuditDocument1 pageTest AuditSilvana Manchego SánchezNo ratings yet
- Drink Less QuestionnaireDocument1 pageDrink Less Questionnaire10905106052No ratings yet
- 2.1.3 Formato AuditDocument1 page2.1.3 Formato Auditale.ibacacheNo ratings yet
- Right Mix 3 PDFDocument2 pagesRight Mix 3 PDFRehabilitasi Narkoba Ar RahmanNo ratings yet
- AUDIT - Alcohol Screening TestDocument5 pagesAUDIT - Alcohol Screening TestPatrícia PenariolNo ratings yet
- Alcohol Questionnaire 1 AUDITDocument1 pageAlcohol Questionnaire 1 AUDITS. LeighNo ratings yet
- AUDIT-test Alcool PDFDocument2 pagesAUDIT-test Alcool PDFrwj2g4px26No ratings yet
- Screening Tool Domain - DUDIT: 0 1 2 3 4 ScoreDocument2 pagesScreening Tool Domain - DUDIT: 0 1 2 3 4 ScoreJasper CubiasNo ratings yet
- Audit Alcohol QuestionnaireDocument2 pagesAudit Alcohol QuestionnaireaberosnerNo ratings yet
- Impact of Alcoholism and The Level of Criminality Among Youth in Barangay New Visayas Montevista Davao de Oro Questionnaire Full Name: - NicknameDocument10 pagesImpact of Alcoholism and The Level of Criminality Among Youth in Barangay New Visayas Montevista Davao de Oro Questionnaire Full Name: - NicknameCamille CobrillaNo ratings yet
- New Registration PackDocument12 pagesNew Registration PackrosielavisNo ratings yet
- Supplementary File Survey Question Response OptionsDocument3 pagesSupplementary File Survey Question Response OptionsEliza DNNo ratings yet
- 2010 - CUDIT R Revised With Scoring ENDocument1 page2010 - CUDIT R Revised With Scoring ENDiana BNo ratings yet
- Alcohol LeafletDocument2 pagesAlcohol LeafletMihai FoxNo ratings yet
- AUDIT SpanishDocument1 pageAUDIT SpanishFirdovsi AliyevNo ratings yet
- The Audit: Questions 0 1 2 3 4Document1 pageThe Audit: Questions 0 1 2 3 4GoFishGoNo ratings yet
- Dependenta AlcoolDocument2 pagesDependenta AlcoolAnonymous FXvVwYyakONo ratings yet
- Patient LM AbuseDocument1 pagePatient LM AbuseTracey VillalbaNo ratings yet
- Alcohol Use QuestionnaireDocument4 pagesAlcohol Use QuestionnaireJulius DolanaNo ratings yet
- 검진문진표 - Health Examination QuestionnaireDocument6 pages검진문진표 - Health Examination QuestionnaireNabila Shaffa Rizky ChandraNo ratings yet
- Cudit R Cannabis Use Disorders Identification TestDocument1 pageCudit R Cannabis Use Disorders Identification TestSanskrit education DepartmentNo ratings yet
- ACI-Brief-psychosocial-clinical-assessment-toolDocument2 pagesACI-Brief-psychosocial-clinical-assessment-toolRoseanne BressanNo ratings yet
- Alcohol Related Liver DiseaseDocument9 pagesAlcohol Related Liver Diseasesabahat.husainNo ratings yet
- No Evidence of DependenceDocument2 pagesNo Evidence of Dependencemago1961No ratings yet
- 7786 19 Health and Welbeing QuestionnaireDocument29 pages7786 19 Health and Welbeing QuestionnairemadhuNo ratings yet
- Alcohol Addiction Treatment and Self-HelpDocument5 pagesAlcohol Addiction Treatment and Self-HelpdanielbradfordNo ratings yet
- Leeds Dependence Questionnaire1Document1 pageLeeds Dependence Questionnaire1drmadankumarbnysNo ratings yet
- Alcohol QuestionnaireDocument2 pagesAlcohol QuestionnaireXtream 2016No ratings yet
- Mhi NPV PacketDocument10 pagesMhi NPV PacketCodyNo ratings yet
- Arc QuestionnaireDocument1 pageArc QuestionnaireJanet FernandezNo ratings yet
- ALCOHOLDocument1 pageALCOHOLJohana Pinagayao AngkadNo ratings yet
- Initial GHQ 12 QDocument2 pagesInitial GHQ 12 QJohn Wilbert SarausosNo ratings yet
- Cannabis Use Disorder Identification TestDocument1 pageCannabis Use Disorder Identification TestMichael_Lee_RobertsNo ratings yet
- Audit C en EspañolDocument2 pagesAudit C en EspañolNataliaRafaelRoblesNo ratings yet
- Recognising Problem DrinkingDocument2 pagesRecognising Problem DrinkingHa RuNo ratings yet
- LW Challenge FormDocument13 pagesLW Challenge Formapi-316724738No ratings yet
- Adult Reg Pack 291021Document10 pagesAdult Reg Pack 291021oliverstevensonhoareNo ratings yet
- Alcool Test Si AdictiiDocument36 pagesAlcool Test Si Adictiisolaris1ro100% (1)
- Healthier Alcohol Choices No BleedDocument12 pagesHealthier Alcohol Choices No BleedPaulNo ratings yet
- Alcohol Addiction TreatmentDocument12 pagesAlcohol Addiction Treatmentkuna2750% (2)
- Alcohol Use Disorder: A Comparison Between DSM-IV and DSM-5Document5 pagesAlcohol Use Disorder: A Comparison Between DSM-IV and DSM-5Grecia BocuNo ratings yet
- Reg Form - Adult 2016Document9 pagesReg Form - Adult 2016Antonio LoscialeNo ratings yet
- Appendix A: Study Measures and Self-Report QuestionnairesDocument1 pageAppendix A: Study Measures and Self-Report QuestionnairesKen RegisterNo ratings yet
- PROMs Submission 1 - Attachment 2Document13 pagesPROMs Submission 1 - Attachment 2Ken RegisterNo ratings yet
- Measure - Goal Attainment Scale ExamplesDocument1 pageMeasure - Goal Attainment Scale ExamplesKen RegisterNo ratings yet
- Physical Symptoms PHQ-15 ScoredDocument2 pagesPhysical Symptoms PHQ-15 ScoredKen RegisterNo ratings yet
- Good MorningDocument32 pagesGood MorningDdidie100% (1)
- Chapter 5 DRUG EDUCDocument38 pagesChapter 5 DRUG EDUCRiza Roxanne ManongdoNo ratings yet
- Baby Thesis About Drug AddictionDocument7 pagesBaby Thesis About Drug Addictionamberedmondsonnorman100% (2)
- Unilab Case StudyDocument27 pagesUnilab Case StudyIvan Jio Revilla SanchezNo ratings yet
- Drug Education: Prevention of Substance Use and AbuseDocument37 pagesDrug Education: Prevention of Substance Use and Abusejohn lesterNo ratings yet
- DrugsDocument4 pagesDrugsAlfred Amba100% (1)
- The Analysis of Pharmaceutical MarketDocument10 pagesThe Analysis of Pharmaceutical MarketAnamaria BejenariuNo ratings yet
- Dangerous DrugsDocument48 pagesDangerous DrugsNigel HopeNo ratings yet
- Module 4 FinalDocument13 pagesModule 4 FinalMin HwanNo ratings yet
- Hospital PharmacyDocument100 pagesHospital PharmacySyeda Eshaal JavaidNo ratings yet
- Topic: What Are Drugs?: CDI 7: Vice and Drug Education and ControlDocument14 pagesTopic: What Are Drugs?: CDI 7: Vice and Drug Education and ControlSmith Blake0% (1)
- Hospital Pharmacy Service Guideline, 2072 (2015) - Translated FinalDocument8 pagesHospital Pharmacy Service Guideline, 2072 (2015) - Translated Finalprakash.kmc81No ratings yet
- Substance Abuse in ChildrenDocument1 pageSubstance Abuse in ChildrenasdfjkNo ratings yet
- History of Pharmacy in IndiaDocument11 pagesHistory of Pharmacy in Indiasyedurrahman855No ratings yet
- Pharmacology Notes (Introduction To Pharmacology)Document16 pagesPharmacology Notes (Introduction To Pharmacology)BRYCE WILLIAM GONo ratings yet
- Republic Act No 7394Document40 pagesRepublic Act No 7394M Azeneth JJ100% (1)
- Drug AnalysisDocument23 pagesDrug AnalysisCRoMoXT officialNo ratings yet
- Detailed Lesson Plan in Physical EducatiDocument7 pagesDetailed Lesson Plan in Physical EducatiEdalyn Despe Montemor100% (1)
- GDocument22 pagesGMohammad Rayan BaltNo ratings yet
- 814 Model AnswerDocument33 pages814 Model AnswerInFiNiTyNo ratings yet
- I. Crossword Puzzle: Use The Provided Clues To Fill Out The Puzzle. (10 Items X 2 Points)Document3 pagesI. Crossword Puzzle: Use The Provided Clues To Fill Out The Puzzle. (10 Items X 2 Points)Russelle judeNo ratings yet
- Diagnostic Test in Mapeh: I. MusicDocument4 pagesDiagnostic Test in Mapeh: I. MusicLea nessa OrnedoNo ratings yet
- Alexa Cassandra MDocument4 pagesAlexa Cassandra MAlexa VeluzNo ratings yet
- Drugs Q and ADocument5 pagesDrugs Q and ALicudine Hiasmin100% (2)
- Classical Osteopathy PDFDocument400 pagesClassical Osteopathy PDFAnonymous yvlCvHw100% (6)
- Articles of AssociationDocument25 pagesArticles of AssociationОльга МиличенковаNo ratings yet
- Interview QsDocument6 pagesInterview QsRaise RaiseNo ratings yet
- 3.4.3 Test (TST) - DrugsDocument10 pages3.4.3 Test (TST) - Drugsjvillarreal489No ratings yet
- Mapeh 8 4th Quarter Summative TestDocument4 pagesMapeh 8 4th Quarter Summative Testnujnuj nitagac80% (5)