Success& Failures in Endo
Success& Failures in Endo
Download as docx, pdf, or txt
You might also like
- Endodontic RadiologyFrom EverandEndodontic RadiologyBettina BasraniNo ratings yet
- Amalgam FailuresDocument16 pagesAmalgam Failuresrasagna reddyNo ratings yet
- 1 - Ahmed Sle MCQ EndoDocument29 pages1 - Ahmed Sle MCQ EndoShabana Serju83% (18)
- Non Carious LesionsDocument18 pagesNon Carious LesionsAjmal NajeebNo ratings yet
- Cast RestorationsDocument185 pagesCast Restorationsrasagna reddy100% (1)
- Remineralising AgentsDocument142 pagesRemineralising Agentsrasagna reddyNo ratings yet
- Diseases of Periradicular TissuesDocument122 pagesDiseases of Periradicular TissuesAnas Kallayil100% (4)
- Endodontic Failures-A Review: Dr. Sadashiv Daokar, DR - Anita.KalekarDocument6 pagesEndodontic Failures-A Review: Dr. Sadashiv Daokar, DR - Anita.KalekarGunjan Garg100% (1)
- Anatomy of The Pulp SpaceDocument35 pagesAnatomy of The Pulp SpaceDeen Mohd100% (1)
- Vertical Root Fracture !Document42 pagesVertical Root Fracture !Dr Dithy kkNo ratings yet
- Perforations & ManagementDocument163 pagesPerforations & ManagementAPARNA AARATHI SREEKUMARNo ratings yet
- Non Cervical Lesions Meena MamDocument120 pagesNon Cervical Lesions Meena Mamanshida v pNo ratings yet
- Clinical ConsiderationsDocument108 pagesClinical ConsiderationsPankaj JainNo ratings yet
- Flare Ups in EndodonticsDocument12 pagesFlare Ups in EndodonticsAnamika Thakur RanaNo ratings yet
- Pulp and Periapex: Pathologies of Periradicular TissuesDocument12 pagesPulp and Periapex: Pathologies of Periradicular Tissuesdrpriyanka patel100% (1)
- Endodontics Final Exam Study GuideDocument10 pagesEndodontics Final Exam Study GuideBrandon HooperNo ratings yet
- Smearlayerinendodontics 170106182934Document80 pagesSmearlayerinendodontics 170106182934GetLyricsNo ratings yet
- Operative DentistryDocument51 pagesOperative Dentistryqra_beliebersNo ratings yet
- Endodontic Access Preparation The Tools For SuccessDocument9 pagesEndodontic Access Preparation The Tools For SuccessAna YUNo ratings yet
- Access Cavity Preparation FinalDocument63 pagesAccess Cavity Preparation Finalrasagna reddyNo ratings yet
- Soffit and PCD PDFDocument4 pagesSoffit and PCD PDFKalpanaNo ratings yet
- Contemporary Endodontics - DNCADocument219 pagesContemporary Endodontics - DNCAARTNo ratings yet
- Disinfection of The Root CanalDocument45 pagesDisinfection of The Root CanalSachin B Mangalekar100% (1)
- MTA-Based Root Canal Sealers PDFDocument6 pagesMTA-Based Root Canal Sealers PDFAndrew GarciaNo ratings yet
- Endodontic AccessDocument5 pagesEndodontic AccessShyambhavi SrivastavaNo ratings yet
- DIAGNOSTIC METHODS (Emphasis On Recent Advances) IN EndodonticsDocument51 pagesDIAGNOSTIC METHODS (Emphasis On Recent Advances) IN EndodonticsKalpesh Dey100% (1)
- 1 - Intracanal MedicamentsDocument10 pages1 - Intracanal MedicamentsZaid AKNo ratings yet
- Working Length Determination in RCTDocument38 pagesWorking Length Determination in RCTDidar Sadiq Kwekha100% (1)
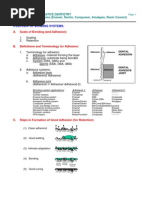
- Overview of Bonding SystemsDocument13 pagesOverview of Bonding SystemsBhanuji Naidu100% (1)
- Apical Seal Versus Coronal SealDocument8 pagesApical Seal Versus Coronal SealSalem RawashdahNo ratings yet
- Recent Advances in Instrumentation Techniques - Dental Ebook & Lecture Notes PDF Download (Studynama - Com - India's Biggest Website For BDS Study Material Downloads)Document23 pagesRecent Advances in Instrumentation Techniques - Dental Ebook & Lecture Notes PDF Download (Studynama - Com - India's Biggest Website For BDS Study Material Downloads)Vinnie SinghNo ratings yet
- 1 Cbct-Evaluation of Remaining Dentin Thickness and Fracture Resistance of Conventional and Conservative Access and Biomechanical Preparation in Molars Using Cone-beam Computed Tomography- An in Vitro StudyDocument4 pages1 Cbct-Evaluation of Remaining Dentin Thickness and Fracture Resistance of Conventional and Conservative Access and Biomechanical Preparation in Molars Using Cone-beam Computed Tomography- An in Vitro StudyalbertaugustineNo ratings yet
- Infiltration, A New Therapy For Masking Enamel White Spot PDFDocument12 pagesInfiltration, A New Therapy For Masking Enamel White Spot PDFwijayanti siswantoNo ratings yet
- Kutler's Thery PDFDocument10 pagesKutler's Thery PDFSam RoyNo ratings yet
- Aae Endodonticglossary2016Document50 pagesAae Endodonticglossary2016h20pologtNo ratings yet
- Conservative DentistryDocument6 pagesConservative DentistryAbdallah Essam Al-ZireeniNo ratings yet
- PulpDocument54 pagesPulpAnsh DuttaNo ratings yet
- Calcium Hydroxide, Root ResorptionDocument9 pagesCalcium Hydroxide, Root ResorptionLize Barnardo100% (1)
- Focal Infection Theory: A Focus On Current AspectsDocument7 pagesFocal Infection Theory: A Focus On Current AspectsDiandra Puspa WidyasariNo ratings yet
- E.monoblock RevisitedDocument5 pagesE.monoblock RevisitedVinisha Vipin SharmaNo ratings yet
- Dental Floss Ties For Rubber Dam Isolation - A Proposed Classification and A New Technique.Document7 pagesDental Floss Ties For Rubber Dam Isolation - A Proposed Classification and A New Technique.marianaduque82No ratings yet
- Intra Canal MedicamentsDocument14 pagesIntra Canal MedicamentsS Noshin ShimiNo ratings yet
- Managementofnoncariouslesions 140228135843 Phpapp01Document145 pagesManagementofnoncariouslesions 140228135843 Phpapp01Anoop maniNo ratings yet
- Endo MishapsDocument66 pagesEndo Mishapsmahmoud100% (1)
- Cementation of Indirect Restorations - An Overview of Resin CementsDocument6 pagesCementation of Indirect Restorations - An Overview of Resin CementsNaoki MezarinaNo ratings yet
- Developmental Disturbances of TeethDocument45 pagesDevelopmental Disturbances of TeethAmritha JamesNo ratings yet
- Endodontic DisesaeDocument9 pagesEndodontic DisesaeNouman NoorNo ratings yet
- Obturation Techniques in ChildDocument6 pagesObturation Techniques in ChildMonisha100% (1)
- Root Canal Sealers - SeminarDocument49 pagesRoot Canal Sealers - Seminarkowmudimaddineni100% (2)
- Apical Third and Its SignificanceDocument20 pagesApical Third and Its SignificanceBharath Ratnakaram100% (1)
- Dental Material MCQ Test Bank Chapter 002Document18 pagesDental Material MCQ Test Bank Chapter 002Táláát ÄlsuroriNo ratings yet
- Transportation of Severely Curved Canals Comparison of One Shape and k3 Rotary SystemsDocument5 pagesTransportation of Severely Curved Canals Comparison of One Shape and k3 Rotary SystemsAnonymous RvEXV2mPNo ratings yet
- Management of Blunderbuss CanalsDocument11 pagesManagement of Blunderbuss CanalsNitesh PatilNo ratings yet
- Etched Cast RestorationsDocument41 pagesEtched Cast Restorationssharanya chekkarrajNo ratings yet
- 3 Recent Advances in Irrigation SystemsDocument12 pages3 Recent Advances in Irrigation SystemsnobelcyrilNo ratings yet
- Regressive Changes of TeethDocument45 pagesRegressive Changes of TeethNader AlaizariNo ratings yet
- Pulp Therapy of Non-Vital Teeth (Pulpectomy)Document27 pagesPulp Therapy of Non-Vital Teeth (Pulpectomy)Mahmoud A. Zoghbor100% (1)
- Diagnosis of Dental CariesDocument24 pagesDiagnosis of Dental CariesyomanNo ratings yet
- Post-Treatment Endodontic Disease and Re-Treatment Dummer2008Document2 pagesPost-Treatment Endodontic Disease and Re-Treatment Dummer2008Neeraj1973No ratings yet
- A Cess Cavity PreparationDocument54 pagesA Cess Cavity Preparationmandy0077No ratings yet
- Non CariousDocument4 pagesNon CariousUpasana BhandariNo ratings yet
- Working LengthDocument67 pagesWorking LengthnishthaNo ratings yet
- Caries DiagnosisDocument31 pagesCaries Diagnosisrasagna reddyNo ratings yet
- Endodontic MicrobiologyDocument219 pagesEndodontic Microbiologyrasagna reddy100% (1)
- Biomechanics of Pin and Post Retained Restorations-MadhurimaDocument190 pagesBiomechanics of Pin and Post Retained Restorations-Madhurimarasagna reddy100% (1)
- Amalgam Structure and Properties PPT With AudioDocument25 pagesAmalgam Structure and Properties PPT With Audiorasagna reddy100% (2)
- Restorative Resin Composites: For Direct RestorationsDocument75 pagesRestorative Resin Composites: For Direct Restorationsrasagna reddyNo ratings yet
- Department of Periodontics and Implantology: Calcium MetabolismDocument63 pagesDepartment of Periodontics and Implantology: Calcium Metabolismrasagna reddy100% (1)
- 6.chair PositionsDocument17 pages6.chair Positionsrasagna reddy100% (1)
- Antioxidants in EndodonticsDocument48 pagesAntioxidants in Endodonticsrasagna reddyNo ratings yet
- Rationale in EndodonticsDocument16 pagesRationale in Endodonticsrasagna reddyNo ratings yet
- COMPLEX AMALGAM REST RamDocument80 pagesCOMPLEX AMALGAM REST Ramrasagna reddyNo ratings yet
- Presentation2 CeramicsDocument160 pagesPresentation2 Ceramicsrasagna reddyNo ratings yet
- DIRECT FILLING GOLD RamDocument148 pagesDIRECT FILLING GOLD Ramrasagna reddyNo ratings yet
- Smear LayerDocument130 pagesSmear Layerrasagna reddy100% (4)
- Dentinal Hypersensitivity: Guided By: Dr.P.Karunakar DR - Umrana Faizuddin DR - Ashish JainDocument144 pagesDentinal Hypersensitivity: Guided By: Dr.P.Karunakar DR - Umrana Faizuddin DR - Ashish Jainrasagna reddyNo ratings yet
- Presentation 6 1 1Document73 pagesPresentation 6 1 1rasagna reddyNo ratings yet
- Intracanal Medicaments: Presented By: DR - Suruchi Sisodia Dept. of Conservative Dentistry and EndodonticsDocument106 pagesIntracanal Medicaments: Presented By: DR - Suruchi Sisodia Dept. of Conservative Dentistry and Endodonticsrasagna reddy100% (1)
- 10 1016@j Joen 2020 04 007Document9 pages10 1016@j Joen 2020 04 007rasagna reddyNo ratings yet
- Root-End Filling Materials: An Update On The Latest Materials: A ReviewDocument5 pagesRoot-End Filling Materials: An Update On The Latest Materials: A Reviewrasagna reddyNo ratings yet
- Case Report Management of An Upper Central Incisor Having Periapical Pathology With Unusual PresentationDocument4 pagesCase Report Management of An Upper Central Incisor Having Periapical Pathology With Unusual Presentationrasagna reddyNo ratings yet
- Clinical Management of Orthodontic Root Resorption Glenn T. Sameshima 2024 Scribd DownloadDocument62 pagesClinical Management of Orthodontic Root Resorption Glenn T. Sameshima 2024 Scribd Downloadrmungabia100% (2)
- Relationship Between Calcium Hydroxide PDocument9 pagesRelationship Between Calcium Hydroxide PRazvan UngureanuNo ratings yet
- Pathological Tooth ResorptionDocument143 pagesPathological Tooth ResorptionAnas KallayilNo ratings yet
- Dental Trauma in Young Perma123nent TeethDocument75 pagesDental Trauma in Young Perma123nent TeethGiulian SabinNo ratings yet
- Corticotomy-Assisted OrthodonticsDocument6 pagesCorticotomy-Assisted Orthodonticsyui cherryNo ratings yet
- Clinical Management of Severe External Root Resorption: T C K Y A C C P LDocument6 pagesClinical Management of Severe External Root Resorption: T C K Y A C C P LNevena SaulicNo ratings yet
- Int Endodontic J - 2011 - MohammadiDocument34 pagesInt Endodontic J - 2011 - Mohammadifelipe martinezNo ratings yet
- Pathophysiological Mechanisms of Root Resorption After Dental TraumaDocument15 pagesPathophysiological Mechanisms of Root Resorption After Dental TraumadianaNo ratings yet
- Radiographic Features of RL LesionsDocument7 pagesRadiographic Features of RL Lesionszyad ahmedNo ratings yet
- PDF Clinical Periodontology and Implant Dentistry 4th Edition Jan Lindhe DownloadDocument84 pagesPDF Clinical Periodontology and Implant Dentistry 4th Edition Jan Lindhe Downloadtiussyslak100% (2)
- Dental Trauma - An Overview of Its Influence On The Management of Orthodontic Treatment - Part 1.Document11 pagesDental Trauma - An Overview of Its Influence On The Management of Orthodontic Treatment - Part 1.Djoka DjordjevicNo ratings yet
- Important Tables of Oral PathologyDocument17 pagesImportant Tables of Oral PathologyEasy Med LecturesNo ratings yet
- U4Document8 pagesU4Ana CristinaNo ratings yet
- MUCLecture 2023 2100800Document11 pagesMUCLecture 2023 2100800kashifahmed31gkpNo ratings yet
- Root Surface Demineralization in Periodontal Therapy Subject ReviewDocument6 pagesRoot Surface Demineralization in Periodontal Therapy Subject ReviewRosvin FernandezNo ratings yet
- European Journal of OrthodonticsDocument288 pagesEuropean Journal of Orthodonticsikeuchi_ogawaNo ratings yet
- Trauma From Occlusion - Periodontal TraumatismDocument14 pagesTrauma From Occlusion - Periodontal TraumatismGrestyasanti WimasanNo ratings yet
- 2012 Pulp and Periodontal TissueDocument6 pages2012 Pulp and Periodontal TissuebaridinoNo ratings yet
- PLANETS OF ORTHODONTICS- VOLUME 7- ADULTS AND COMPLEX CASES IN ORTHODON-TICS PLANET URANUSDocument158 pagesPLANETS OF ORTHODONTICS- VOLUME 7- ADULTS AND COMPLEX CASES IN ORTHODON-TICS PLANET URANUSranouNo ratings yet
- Cervical Root Resorption and Non Vital Bleaching.16Document6 pagesCervical Root Resorption and Non Vital Bleaching.16yasser bedirNo ratings yet
- Borkar 2015Document6 pagesBorkar 2015Jing XueNo ratings yet
- Development of The ToothDocument22 pagesDevelopment of The ToothJoyce LimNo ratings yet
- Endodontics Final Exam Study GuideDocument10 pagesEndodontics Final Exam Study GuideBrandon HooperNo ratings yet
- DR - Ritty Arouje Recent Question Paper FileDocument118 pagesDR - Ritty Arouje Recent Question Paper Filemuneer024No ratings yet
- SHAHRANIDocument6 pagesSHAHRANIMishellKarelisMorochoSegarraNo ratings yet
- DiagnosisDocument51 pagesDiagnosisRamya ChowdaryNo ratings yet
- Aristizábal-P - 2014 - Ortodoncia Acelerada y Ortodoncia de Transito Expreso (OTE) ®, Un Concepto Contemporáneo de Alta Eficiencia TTDocument18 pagesAristizábal-P - 2014 - Ortodoncia Acelerada y Ortodoncia de Transito Expreso (OTE) ®, Un Concepto Contemporáneo de Alta Eficiencia TTMilton david Rios serratoNo ratings yet
- Comparison of Root Resorption After Bone-Borne and Tooth-Borne Rapid Maxillary Expansion Evaluated With The Use of MicrotomographyDocument9 pagesComparison of Root Resorption After Bone-Borne and Tooth-Borne Rapid Maxillary Expansion Evaluated With The Use of MicrotomographyMonojit DuttaNo ratings yet