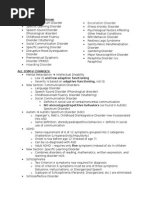
Psychosis Objectives
Psychosis Objectives
Download as pdf or txt
You might also like
- Teaching ProfessionDocument12 pagesTeaching ProfessionAnonymous E2A6hn4U100% (2)
- Psychiatry Under the Influence: Institutional Corruption, Social Injury, and Prescriptions for ReformFrom EverandPsychiatry Under the Influence: Institutional Corruption, Social Injury, and Prescriptions for ReformRating: 2 out of 5 stars2/5 (1)
- Chapter 23 - Medication Interest ModelDocument83 pagesChapter 23 - Medication Interest ModelNaomi LiangNo ratings yet
- 4 - Kiehn, B & Swales, M. (2007) - An Overview of Dialectical Behaviour Therapy in The Treatment ofDocument9 pages4 - Kiehn, B & Swales, M. (2007) - An Overview of Dialectical Behaviour Therapy in The Treatment ofAnastasiya PlohihNo ratings yet
- Why Learn A New Treatment?: Why Dialectical Behavior Therapy (DBT) ?Document22 pagesWhy Learn A New Treatment?: Why Dialectical Behavior Therapy (DBT) ?Doomimummo100% (2)
- Bipolar Disorder: Understanding Bipolar Disorder, and how it can be managed, treated, and improvedFrom EverandBipolar Disorder: Understanding Bipolar Disorder, and how it can be managed, treated, and improvedNo ratings yet
- Psychological DisordersDocument48 pagesPsychological DisordersBrian WuNo ratings yet
- Lcmhca Pds LohornDocument3 pagesLcmhca Pds Lohornapi-433830434No ratings yet
- 1-History of PsychiatryDocument3 pages1-History of PsychiatryLevy DuranNo ratings yet
- DSM V SummaryDocument3 pagesDSM V Summaryhachoi007No ratings yet
- Shared Psychotic Disorder - NCBIDocument8 pagesShared Psychotic Disorder - NCBI5KevNo ratings yet
- My Emotions and Facial ExpressionsDocument8 pagesMy Emotions and Facial ExpressionsVanessa RamírezNo ratings yet
- Hierarchy of Feared SituationsDocument1 pageHierarchy of Feared SituationspanickedchickNo ratings yet
- Mental Health Module DraftDocument21 pagesMental Health Module DraftArnold RamirezNo ratings yet
- Young Children PDFDocument8 pagesYoung Children PDFfotinimavr94No ratings yet
- OCD Action Book List Obsessive Compulsive DisorderDocument3 pagesOCD Action Book List Obsessive Compulsive DisorderrrrrrrrrrrrrrrrrrrrrrrNo ratings yet
- SSCT InterpDocument4 pagesSSCT InterppaorovedilloNo ratings yet
- Use Drugs - Pay To Die Drugs AddictionDocument11 pagesUse Drugs - Pay To Die Drugs AddictionelvineNo ratings yet
- MI Change PlanDocument3 pagesMI Change Planeclatant100% (1)
- Suicidal Ideation Coping ResponsesDocument32 pagesSuicidal Ideation Coping ResponsesKath BuñoNo ratings yet
- The Stages of Change: Experience LifeDocument13 pagesThe Stages of Change: Experience LifeRicky MonsalveNo ratings yet
- Bipolar Disorder: Download PDF Download Epub Order A Free Hardcopy en EspañolDocument50 pagesBipolar Disorder: Download PDF Download Epub Order A Free Hardcopy en EspañolMark Anthony Bueno AsuncionNo ratings yet
- Kinder Home LinksDocument12 pagesKinder Home Linksapi-360345401No ratings yet
- Orientation ManualDocument55 pagesOrientation ManualprashanthNo ratings yet
- DSM-5 Survival Guide Formatted FinalDocument73 pagesDSM-5 Survival Guide Formatted FinalrobajonesincNo ratings yet
- AbpsyDocument18 pagesAbpsyirish xNo ratings yet
- Rational Emotive Behaviour TherapyDocument16 pagesRational Emotive Behaviour TherapyCharrise RamkissoonNo ratings yet
- Adult Psychiatric Inpatient Unit Patient ScheduleDocument2 pagesAdult Psychiatric Inpatient Unit Patient ScheduleJuanCarlos Yogi100% (1)
- Marijuana THC PresentationDocument21 pagesMarijuana THC PresentationJomariexOrtizNo ratings yet
- The Caused and Risk of Drugs On AdolescentsDocument20 pagesThe Caused and Risk of Drugs On AdolescentsSyra Mae LausaNo ratings yet
- Module 4 - Part 3 - SED 2100Document15 pagesModule 4 - Part 3 - SED 2100kylieNo ratings yet
- Anger and Stress ManagementDocument40 pagesAnger and Stress ManagementMaharaja Maharonga100% (1)
- Child DisordersDocument111 pagesChild Disorderspriyanka raj100% (1)
- The Side Effects of Common Psychiatric DrugsDocument28 pagesThe Side Effects of Common Psychiatric Drugsivanarjona100% (1)
- NIH Public Access: Author ManuscriptDocument14 pagesNIH Public Access: Author ManuscriptMarcos ParedesNo ratings yet
- Emotional Disturbance: The Individuals With Disabilities Education Act IDEA Defines Emotional Disturbance As FollowsDocument15 pagesEmotional Disturbance: The Individuals With Disabilities Education Act IDEA Defines Emotional Disturbance As FollowsJeorgette T. GarroteNo ratings yet
- APA - DSM 5 Depression Bereavement Exclusion PDFDocument2 pagesAPA - DSM 5 Depression Bereavement Exclusion PDFDaniel NgNo ratings yet
- The Cycle of ViolenceDocument2 pagesThe Cycle of ViolenceEngr Fahimuddin QureshiNo ratings yet
- Fairness WorksheetDocument2 pagesFairness Worksheetapi-376666984No ratings yet
- Caregiver Nursing InterventionsDocument5 pagesCaregiver Nursing InterventionsSona AntoNo ratings yet
- Psychosis PDFDocument34 pagesPsychosis PDFGrace LNo ratings yet
- What Is Mental Health?: Risk FactorsDocument2 pagesWhat Is Mental Health?: Risk FactorsElmaRabagoNo ratings yet
- What Are Grief and Loss?Document4 pagesWhat Are Grief and Loss?TommyNo ratings yet
- Columbia Suicide Severity Rating Scale Screen VersionDocument2 pagesColumbia Suicide Severity Rating Scale Screen VersionPaul SmithNo ratings yet
- Cognitive-BehaviouralTherapyinCancerPatients (1) - Brief CBT For CancerDocument23 pagesCognitive-BehaviouralTherapyinCancerPatients (1) - Brief CBT For CancerfitranoenoeNo ratings yet
- Mental ExamDocument7 pagesMental ExamEricka Mae GarciaNo ratings yet
- EmotionalDocument7 pagesEmotionalapi-367611011No ratings yet
- Counselling Psy NotesDocument25 pagesCounselling Psy NotesPragnya Nidugonda100% (1)
- Guia - AdolescentesDocument6 pagesGuia - AdolescentesCentro De Psicoterapia Condesa100% (1)
- Voices and Pseudo-Voices in Psychosis and OCD Differential DiagnosisDocument5 pagesVoices and Pseudo-Voices in Psychosis and OCD Differential DiagnosisRobert A. LindsayNo ratings yet
- Rumination 2Document25 pagesRumination 2Abigail RosenkoetterNo ratings yet
- Loss, Grief, and Death Typed NotesDocument7 pagesLoss, Grief, and Death Typed NotesYoung LexieNo ratings yet
- Self CompassionDocument4 pagesSelf CompassionnoraNo ratings yet
- Provisional DiagnosisDocument10 pagesProvisional DiagnosisVanessa DiazNo ratings yet
- The Treatment and Management of Selfharm in Emergency Departments Slide Set Powerpoint 189897661Document41 pagesThe Treatment and Management of Selfharm in Emergency Departments Slide Set Powerpoint 189897661Zorbey TurkalpNo ratings yet
- CasestudyDocument6 pagesCasestudyapi-297258832No ratings yet
- Management of Psychotic SymptomsDocument25 pagesManagement of Psychotic Symptomsmisstheatricality130No ratings yet
- Treatment of High-Risk Sexual Offenders: An Integrated ApproachFrom EverandTreatment of High-Risk Sexual Offenders: An Integrated ApproachNo ratings yet
- Teenage Health Concerns: How Parents Can Manage Eating Disorders In Teenage ChildrenFrom EverandTeenage Health Concerns: How Parents Can Manage Eating Disorders In Teenage ChildrenNo ratings yet
- Registration & Notices On The RegisterDocument46 pagesRegistration & Notices On The RegisterZoey ChangNo ratings yet
- Khilafah Abu AyoobDocument14 pagesKhilafah Abu AyoobMusab Ibn UmayerNo ratings yet
- CH 1 PDFDocument10 pagesCH 1 PDFRajat PradhanNo ratings yet
- ENGLISH 11 TEST FOR UNIT 4-2Document6 pagesENGLISH 11 TEST FOR UNIT 4-2John NguyễnNo ratings yet
- Chapter 4,5 and 6Document30 pagesChapter 4,5 and 6yitayewmalede1987No ratings yet
- Conferment of Pakistan Civil Awards 2023Document29 pagesConferment of Pakistan Civil Awards 2023faizan warraichNo ratings yet
- How To Spot Trends: A Trend Training Manual (With Actual Examples Inside!)Document26 pagesHow To Spot Trends: A Trend Training Manual (With Actual Examples Inside!)Jessieann Balmaceda CabanganNo ratings yet
- StatisticsDocument4 pagesStatisticsPakistani ReactionNo ratings yet
- Araling PanlipunanDocument2 pagesAraling PanlipunanMaria Cristina False100% (2)
- 1.2W Audio Power Amplifier-Yd820: Youda Integrated CircuitDocument4 pages1.2W Audio Power Amplifier-Yd820: Youda Integrated CircuitGenus SumNo ratings yet
- Implementación Proyectos Con myRIO H2 2018Document49 pagesImplementación Proyectos Con myRIO H2 2018Miguel Martin100% (1)
- 22 - G.R. No. 145578Document8 pages22 - G.R. No. 145578Clarince Joyce Lao DoroyNo ratings yet
- Factors Influencing Successful Brand ExtensionDocument12 pagesFactors Influencing Successful Brand ExtensionTayyaba MahrNo ratings yet
- Chapter IIDocument10 pagesChapter IISHeen100% (1)
- Audio AidsDocument7 pagesAudio Aidsanupa_joyNo ratings yet
- Womens Suffrage EssayDocument5 pagesWomens Suffrage Essayvotukezez1z2100% (2)
- SCTZ 0343 Hi - ResDocument84 pagesSCTZ 0343 Hi - ResTibério BarreiraNo ratings yet
- Mitd Dentsu Koichi PresentationDocument51 pagesMitd Dentsu Koichi Presentationdp4mobNo ratings yet
- WWW - Rbu.ac - In: Rabindra Bharati University WebsiteDocument8 pagesWWW - Rbu.ac - In: Rabindra Bharati University WebsiteMayukhSarkarNo ratings yet
- P.4 MTC Set IiDocument11 pagesP.4 MTC Set Iiokwir daniel chrispusNo ratings yet
- Humss - Creative Writing - Q2 - Mod7 - W4 - Staging Modalities and Envisioning The ScriptDocument17 pagesHumss - Creative Writing - Q2 - Mod7 - W4 - Staging Modalities and Envisioning The ScriptSHERMAE ANNE JANE ROLAND100% (1)
- Bussiness EthiquttesDocument9 pagesBussiness EthiquttesPriya DharshiniNo ratings yet
- Teach Like A Champion 100 Percent and No Opt OutDocument25 pagesTeach Like A Champion 100 Percent and No Opt Outapi-314075845No ratings yet
- DUA Budget AssignmentDocument2 pagesDUA Budget AssignmentabisheyimramNo ratings yet
- EL 107 Reviewer (1st Unit Test)Document20 pagesEL 107 Reviewer (1st Unit Test)Princess AngelNo ratings yet
- 1st Quarter Tos UcspDocument2 pages1st Quarter Tos UcspNorven DulaugonNo ratings yet
- The Tourist (2010)Document3 pagesThe Tourist (2010)Krystle WongNo ratings yet
- Climate - Change - Meets - Habitat - Fragmentation - TIBI PDFDocument13 pagesClimate - Change - Meets - Habitat - Fragmentation - TIBI PDFStefana BernatNo ratings yet
- Printable 2024 Calendars Cats LandscapeDocument12 pagesPrintable 2024 Calendars Cats LandscapeDeby ViardiantyNo ratings yet