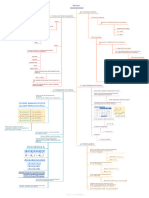
KOMET Study Levetiracetam Vs Depakine
KOMET Study Levetiracetam Vs Depakine
Download as pdf or txt
You might also like
- Top 200 Sorted by Drug ClassDocument3 pagesTop 200 Sorted by Drug Classthompjo2394100% (9)
- CFA Level II Formula Sheet CFA Level II Formula Sheet: Finance (Harvard University) Finance (Harvard University)Document5 pagesCFA Level II Formula Sheet CFA Level II Formula Sheet: Finance (Harvard University) Finance (Harvard University)smith100% (1)
- Example A Language Report Appendix BDocument5 pagesExample A Language Report Appendix BJershon YongNo ratings yet
- Brand Plan For Dienogest by Saqib AltafDocument13 pagesBrand Plan For Dienogest by Saqib AltafSakib ZabooNo ratings yet
- Assignment 9Document2 pagesAssignment 9Nuo XuNo ratings yet
- Non-Isothermal Reactor DesignDocument5 pagesNon-Isothermal Reactor Designnorpius7754No ratings yet
- Larsen & Toubro Limited Kpo Coke Oven Phase-1 LT Cable Sizing Calculation-Bpp AreaDocument12 pagesLarsen & Toubro Limited Kpo Coke Oven Phase-1 LT Cable Sizing Calculation-Bpp AreamustangNo ratings yet
- Test RestDocument2 pagesTest Restf7qzztkkksNo ratings yet
- 2.1.3 - PRISMA 2009 Flow Diagram FillableDocument1 page2.1.3 - PRISMA 2009 Flow Diagram FillablenisasharomNo ratings yet
- Linearity BrochureDocument8 pagesLinearity Brochuremurpy91No ratings yet
- Hoja de Daros Lab9-1Document2 pagesHoja de Daros Lab9-1Angel DikekNo ratings yet
- Adobe Scan 18-Nov-2024Document1 pageAdobe Scan 18-Nov-2024subhadip chakrabortyNo ratings yet
- Nuclear Physics - Mind Map - Lakshya NEET 2024Document1 pageNuclear Physics - Mind Map - Lakshya NEET 2024aanyakaurchonaNo ratings yet
- Acc-406 NoteDocument1 pageAcc-406 Notehanhvy04No ratings yet
- Chemical Kinetics: Col Lisi On Effective CollisDocument1 pageChemical Kinetics: Col Lisi On Effective ColliseliyachrisNo ratings yet
- Est FormulasDocument15 pagesEst FormulasAira GarciaNo ratings yet
- Stat3021 2Document4 pagesStat3021 2sanjna chapseyNo ratings yet
- ElectricityDocument23 pagesElectricitytherankhNo ratings yet
- Assignment 4Document19 pagesAssignment 4Radhe JhaNo ratings yet
- VectorDocument17 pagesVectorPrisha ShailyNo ratings yet
- Allen: Chemical EquilibriumDocument6 pagesAllen: Chemical EquilibriumSaurabh KumarNo ratings yet
- Scale 1491: "Mela Namanarayani": Also Known As: Raga Narmada, Pratapa, Harsh Major-MinorDocument1 pageScale 1491: "Mela Namanarayani": Also Known As: Raga Narmada, Pratapa, Harsh Major-MinorIan RingNo ratings yet
- Upd C11 Phy EngDocument23 pagesUpd C11 Phy EngArinjoy Mervyn GomesNo ratings yet
- Ing ChemDocument4 pagesIng Chempatelheri555No ratings yet
- Midnight Character SheetDocument2 pagesMidnight Character SheetPhilippe LuthiNo ratings yet
- Gaddam, Ikshwak: ResultDocument1 pageGaddam, Ikshwak: Resultpraveen kumarNo ratings yet
- Nuclei - Mind Maps - Yakeen 2.0 2024 BetaDocument1 pageNuclei - Mind Maps - Yakeen 2.0 2024 Betaadarshtiwari4785No ratings yet
- STR DEX CON INT WIS CHA: Operative LVL: 3 Human OutlawDocument3 pagesSTR DEX CON INT WIS CHA: Operative LVL: 3 Human OutlawFacundo GomezNo ratings yet
- Fekete WellTestApplicationsDocument1 pageFekete WellTestApplicationspradyumnNo ratings yet
- Metodos IntegralesDocument31 pagesMetodos IntegralesJosé Arturo FerreraNo ratings yet
- Columbia University Metropolitan State University of DenverDocument1 pageColumbia University Metropolitan State University of DenverM. TanveerNo ratings yet
- 2017-2018 Actors - in - World - Politics - 181217 PDFDocument72 pages2017-2018 Actors - in - World - Politics - 181217 PDFFrancesco RagazziNo ratings yet
- Ac History Matrix - Year 8 Ferris 2017Document1 pageAc History Matrix - Year 8 Ferris 2017api-263403037No ratings yet
- Lund Emily Boyd f17Document4 pagesLund Emily Boyd f17api-456588986No ratings yet
- DC Motors FormulasDocument3 pagesDC Motors FormulasSaabierah SalieNo ratings yet
- Hybrid Blade Element and Lifting Line For Propeller or Propfan PerformanceDocument11 pagesHybrid Blade Element and Lifting Line For Propeller or Propfan PerformancewharNo ratings yet
- 胡 線代 3Document1 page胡 線代 3ljiezhi90No ratings yet
- If Absolutely Conditionally: ComparisonDocument3 pagesIf Absolutely Conditionally: Comparisonlimyh123abcNo ratings yet
- Formulario ReactoresDocument1 pageFormulario Reactoreslourdesmarien31No ratings yet
- 351-Lecture 21Document16 pages351-Lecture 21Rahul BiswasNo ratings yet
- Atomic Structure - Formula Sheet 02 - Arjuna JEE 2025Document2 pagesAtomic Structure - Formula Sheet 02 - Arjuna JEE 2025amitkumarshamli1986No ratings yet
- L16, L17, L18 RL, RC, RLC & Parallel CircuitDocument20 pagesL16, L17, L18 RL, RC, RLC & Parallel Circuitdhruv100% (1)
- 3 - Stoichiometry 2024-09-19 04 - 23 - 10Document8 pages3 - Stoichiometry 2024-09-19 04 - 23 - 10John Noel CabusasNo ratings yet
- Chemical Kinetics Class - 7 (Notes)Document26 pagesChemical Kinetics Class - 7 (Notes)ᴜsʜɴᴇᴇᴋNo ratings yet
- DissertationDocument1 pageDissertationManar AbdulrahmanNo ratings yet
- Cheat SheetDocument1 pageCheat SheetFrancis TanNo ratings yet
- Remaining ProblemsDocument4 pagesRemaining ProblemsKyokyo TokimiNo ratings yet
- Lecture 01Document7 pagesLecture 01guanlin HeNo ratings yet
- Project Management Professional PMP FormulasDocument4 pagesProject Management Professional PMP FormulassachingandhiNo ratings yet
- Protection Settings For 11Kv Bus TieDocument5 pagesProtection Settings For 11Kv Bus Tiemarcelo_santNo ratings yet
- Week 3Document21 pagesWeek 38dzkyfxkn5No ratings yet
- Genberg-Adaptive Optical SystemsDocument23 pagesGenberg-Adaptive Optical SystemskitdocprintNo ratings yet
- Active Components Part 1Document3 pagesActive Components Part 1Dhiraj PatilNo ratings yet
- MLRD 7Document23 pagesMLRD 7damasodra33No ratings yet
- Group Activity - AssignmentDocument1 pageGroup Activity - AssignmentkarmaudeNo ratings yet
- Plano Secciones 002Document1 pagePlano Secciones 002Edward Llanqui RodriguesNo ratings yet
- SurdsDocument30 pagesSurdsmahesh singhNo ratings yet
- EM PresenDocument27 pagesEM Presenchuljoong kangNo ratings yet
- VolteDocument1 pageVoltemohamed100% (1)
- SANAD II ValproateDocument12 pagesSANAD II ValproateveerrajuNo ratings yet
- Internal Medicine Clinical Practice Guidelines 2018 Midyear Review PDFDocument17 pagesInternal Medicine Clinical Practice Guidelines 2018 Midyear Review PDFveerrajuNo ratings yet
- Management of Common Infections With Antimicrobials Guidance Clinical Practice Guidelines (2019) PDFDocument4 pagesManagement of Common Infections With Antimicrobials Guidance Clinical Practice Guidelines (2019) PDFveerrajuNo ratings yet
- Migraine Treatment Guidelines (2019) PDFDocument2 pagesMigraine Treatment Guidelines (2019) PDFveerrajuNo ratings yet
- Pharmacology N23 Group2Document4 pagesPharmacology N23 Group2Andrie JaraveloNo ratings yet
- PracticalDocument10 pagesPracticalGo proNo ratings yet
- Pharmacology QuestionsDocument6 pagesPharmacology Questionsliaqat ahmed100% (1)
- SoriniDocument2 pagesSoriniianecunar100% (2)
- Psychiatric Drugs - ZarinaDocument25 pagesPsychiatric Drugs - Zarinaszarina_7No ratings yet
- Vaccine Order Form SampleDocument3 pagesVaccine Order Form Sampleecint.trmNo ratings yet
- Pharmacology and Venipuncture (Prelim)Document14 pagesPharmacology and Venipuncture (Prelim)Shan Angelie SarmientoNo ratings yet
- (Eğitim Tanrısı) Sarah Lerchenfeldt, Gary Rosenfeld - BRS Pharmacology-LWW (2019) PDFDocument364 pages(Eğitim Tanrısı) Sarah Lerchenfeldt, Gary Rosenfeld - BRS Pharmacology-LWW (2019) PDFjacky58950% (2)
- Acetylcysteine - Drug Information - UpToDateDocument22 pagesAcetylcysteine - Drug Information - UpToDateDaniel ChávezNo ratings yet
- DR Kelvin Vaccine Schedule - Latest 2Document1 pageDR Kelvin Vaccine Schedule - Latest 2Komagal KunaisekaranNo ratings yet
- UntitledDocument205 pagesUntitledAdil PatelNo ratings yet
- B.Pharm Project Work TopicsDocument2 pagesB.Pharm Project Work Topicsbs6794830No ratings yet
- Forecast Reguler TGL 18 Juni Yg Di Kirim Ke PemasokDocument669 pagesForecast Reguler TGL 18 Juni Yg Di Kirim Ke PemasokKFA SENGKANGNo ratings yet
- BuscopanDocument2 pagesBuscopanMae Ann Bueno Castillon100% (1)
- Steroid Tapering and Supportive Treatment Guidance V1.0 PDFDocument1 pageSteroid Tapering and Supportive Treatment Guidance V1.0 PDFyunita hapsariNo ratings yet
- Drug Information HandbookDocument1 pageDrug Information Handbookwulansari nurjanahNo ratings yet
- Wcva Poster Dipyrone Cats - MeDocument1 pageWcva Poster Dipyrone Cats - MeMarina Cayetano EvangelistaNo ratings yet
- Lecture 1 Introduction To PharmacotherapeuticsDocument30 pagesLecture 1 Introduction To Pharmacotherapeuticssha rcNo ratings yet
- Amlodipine ReadingDocument12 pagesAmlodipine Readingines pachecoNo ratings yet
- Pedo Seminar - Analgesics and Antibiotics Used in ChildrenDocument44 pagesPedo Seminar - Analgesics and Antibiotics Used in ChildrenPuneet ChoudharyNo ratings yet
- Drug InspectorDocument6 pagesDrug InspectorDinkar Pandey50% (2)
- Sessa - Shaping The Renaissance of Psychedelic Research - 2012Document2 pagesSessa - Shaping The Renaissance of Psychedelic Research - 2012Mel LissaNo ratings yet
- 1Document12 pages1RAED GhunaimNo ratings yet
- Dara Mola 2016Document5 pagesDara Mola 2016andiniNo ratings yet
- Allergic Rhinitis: PathophysiologyDocument28 pagesAllergic Rhinitis: Pathophysiologysneh1509No ratings yet
- PG Full OseDocument2 pagesPG Full OseDR AbidNo ratings yet
- Pediatric AnesthesiaDocument70 pagesPediatric AnesthesiaAdel Taradji100% (1)
- Praktikum Pengendalian IIDocument22 pagesPraktikum Pengendalian IItrisna kurniaNo ratings yet