DOAC Chart
DOAC Chart
Download as docx, pdf, or txt
You might also like
- Dosage Calculation Practice WorkbookDocument35 pagesDosage Calculation Practice Workbookcrazy crazy crazy100% (1)
- NEONATOLOGYDocument8 pagesNEONATOLOGYmymamym100% (1)
- VTE Risk AssessmentDocument2 pagesVTE Risk AssessmentpriyopanjiNo ratings yet
- Route of AdministrationDocument48 pagesRoute of AdministrationFranchesca LugoNo ratings yet
- Venous Thromboembolism With Blanks ResidentsDocument9 pagesVenous Thromboembolism With Blanks Residentsapi-648714317No ratings yet
- Mild Moderate Severe Clinical Criteria: Covid ProtocolDocument4 pagesMild Moderate Severe Clinical Criteria: Covid ProtocolSiaNo ratings yet
- (April 2020) : Is The Indication Appropriate For A Doac?Document1 page(April 2020) : Is The Indication Appropriate For A Doac?SNo ratings yet
- ABVD-v1.1Document5 pagesABVD-v1.1hapnt79No ratings yet
- SHC ABX Dosing GuideDocument7 pagesSHC ABX Dosing GuideDanielVillaNo ratings yet
- Antiplatelet Drug Comparison Chart (Asa-Clopi-Prasu-Tica)Document1 pageAntiplatelet Drug Comparison Chart (Asa-Clopi-Prasu-Tica)Ponpimol Odee BongkeawNo ratings yet
- Acid Supressive TherapyDocument89 pagesAcid Supressive TherapyWahyu Agung DewaandikaNo ratings yet
- Thrombosis Risk Factor Assessment (Choose All That Apply) : Deep Vein Thrombosis (DVT) Prophylaxis OrdersDocument2 pagesThrombosis Risk Factor Assessment (Choose All That Apply) : Deep Vein Thrombosis (DVT) Prophylaxis OrdersPutu Gizha Satrya GautamaNo ratings yet
- Stanford Health Care Antimicrobial Dosing Reference GuideDocument7 pagesStanford Health Care Antimicrobial Dosing Reference GuideKarl Martin PinedaNo ratings yet
- Antimicrobial Dosing GuideDocument7 pagesAntimicrobial Dosing GuideMuhammad RawasNo ratings yet
- SHC ABX Dosing GuideDocument7 pagesSHC ABX Dosing GuideDeena AlJawamisNo ratings yet
- NOAC ChartDocument2 pagesNOAC Chartsgod34No ratings yet
- 2014 SHC ABX Dosing GuideDocument4 pages2014 SHC ABX Dosing GuideisnaeniNo ratings yet
- Revised COVID 19 SARS-COV2 Treatment Protocol - FinalDocument6 pagesRevised COVID 19 SARS-COV2 Treatment Protocol - FinalupsahuNo ratings yet
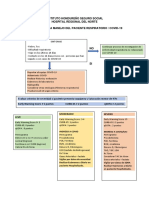
- Protocolo Covid 19 Ihss HRN PDFDocument5 pagesProtocolo Covid 19 Ihss HRN PDFJennifer CarcamoNo ratings yet
- (R) Choep: IndicationDocument5 pages(R) Choep: IndicationAlina CrissNo ratings yet
- NH Protocol For Covid Management FinalDocument7 pagesNH Protocol For Covid Management FinalhoneyworksNo ratings yet
- SHC Antimicrobial Dosing GuideDocument7 pagesSHC Antimicrobial Dosing GuideHelder LopesNo ratings yet
- Anticoagulation 2024Document11 pagesAnticoagulation 2024V NNo ratings yet
- Drugrenaladjustment 12052565Document18 pagesDrugrenaladjustment 12052565jirat iyarapongNo ratings yet
- BMC COVID Anticoagulation Algorithm Update 5 1 20Document1 pageBMC COVID Anticoagulation Algorithm Update 5 1 20Avinash KumbharNo ratings yet
- SHC Vancomycin Dosing GuideDocument8 pagesSHC Vancomycin Dosing GuidePitchya WangmeesriNo ratings yet
- FAQ - DOAC in CKD Update - FinalDocument4 pagesFAQ - DOAC in CKD Update - Finalraea.dobsonNo ratings yet
- STEMI NotesDocument8 pagesSTEMI NotesIzzul HafiyNo ratings yet
- PTO DM 2 Rev Akhir FikkDocument30 pagesPTO DM 2 Rev Akhir FikkDhani WiganiNo ratings yet
- Renal Dosage Adjustment Guidelines For Antimicrobials: WWW - Unmc.edu/aspDocument34 pagesRenal Dosage Adjustment Guidelines For Antimicrobials: WWW - Unmc.edu/aspعبدالواسع نعمانNo ratings yet
- XARELTODocument4 pagesXARELTOMohammed IbrahimNo ratings yet
- Stanford Dosing AntibioticsDocument6 pagesStanford Dosing AntibioticsSayeerah MamaNo ratings yet
- Management of Convulsion in PaediatricsDocument21 pagesManagement of Convulsion in PaediatricsjuwelukgNo ratings yet
- 38054 台北市聯合醫院抗生素商品名對照表 PDFDocument99 pages38054 台北市聯合醫院抗生素商品名對照表 PDFka timNo ratings yet
- Pediatric Drug Dosing GuidelinesDocument182 pagesPediatric Drug Dosing GuidelinesamiratolanNo ratings yet
- Frequent Asking & QuestionDocument18 pagesFrequent Asking & QuestionLhynda Priarti LatifNo ratings yet
- R Mini CHOPDocument5 pagesR Mini CHOPgrethelvalencialaurelNo ratings yet
- Sample Obstetrics Orders: By: Mitra Ahmad SoltaniDocument62 pagesSample Obstetrics Orders: By: Mitra Ahmad Soltanialmslmani9524100% (2)
- 3 - Ob Orders, or Tech, MaterialsDocument14 pages3 - Ob Orders, or Tech, MaterialsJC GoodLifeNo ratings yet
- Stanford Hospital & Clinics Antimicrobial Dosing Reference Guide 2013Document3 pagesStanford Hospital & Clinics Antimicrobial Dosing Reference Guide 2013SANCHOSKYNo ratings yet
- Antibiotic Dosing Guidelines For Renal ImpairmentDocument6 pagesAntibiotic Dosing Guidelines For Renal ImpairmentvitauxianaNo ratings yet
- SHC Vancomycin Dosing Guide PDFDocument6 pagesSHC Vancomycin Dosing Guide PDFAbu Hammoud AlyazeediNo ratings yet
- Direct Oral Anticoagulants (DOACs) For Treatment of DVTDocument11 pagesDirect Oral Anticoagulants (DOACs) For Treatment of DVTLuana MNo ratings yet
- GP AEC DVT Talk FinalDocument57 pagesGP AEC DVT Talk FinalTuan NguyenNo ratings yet
- Stanford Health Care Antimicrobial Dosing Reference GuideDocument6 pagesStanford Health Care Antimicrobial Dosing Reference GuidePaan SuthahathaiNo ratings yet
- Paper 1 Resource PackDocument22 pagesPaper 1 Resource PackHaw Feng ChanNo ratings yet
- Stress Related Mucosal Injury (SRMI) - FinalDocument36 pagesStress Related Mucosal Injury (SRMI) - Finalvadivel kumaran sivasankaranNo ratings yet
- Doacs For VteDocument10 pagesDoacs For VteAhmed MohammedNo ratings yet
- Antiretroviral Therapy: Pharmacology: Cristina Gruta, PharmdDocument47 pagesAntiretroviral Therapy: Pharmacology: Cristina Gruta, PharmdMalueth AnguiNo ratings yet
- Lipids Topic DiscussionDocument10 pagesLipids Topic Discussionapi-665372449No ratings yet
- Antibiotik For Renal FailureDocument6 pagesAntibiotik For Renal FailureWidhy Joss BangetzNo ratings yet
- White Chodosh Appendix VI HSV FINALDocument5 pagesWhite Chodosh Appendix VI HSV FINALSuzana VoiculescuNo ratings yet
- SHC Vancomycin Dosing GuideDocument9 pagesSHC Vancomycin Dosing GuideDanielVillaNo ratings yet
- Renal PharmacologyDocument52 pagesRenal Pharmacologyashraf0% (1)
- Guide To AnticoagulantsDocument6 pagesGuide To AnticoagulantssargentsilerNo ratings yet
- Olaparib BRCA Mutated HER2 Negative Early Breast CancerDocument8 pagesOlaparib BRCA Mutated HER2 Negative Early Breast CancersmokkerNo ratings yet
- Abvd Hem HLDocument6 pagesAbvd Hem HLTowhidulIslamNo ratings yet
- Acs 2023 Part 4 Presentation VersionDocument38 pagesAcs 2023 Part 4 Presentation Versionapi-668470097No ratings yet
- VancomycinDocument6 pagesVancomycinMohammed SaifanNo ratings yet
- 2016 01 M.R. Antibiotic Renal Dosing PDFDocument5 pages2016 01 M.R. Antibiotic Renal Dosing PDFMardari Bogdan CatalinNo ratings yet
- Simplifying Psychiatric Documentation: Time-Saving Templates for Medication RecommendationsFrom EverandSimplifying Psychiatric Documentation: Time-Saving Templates for Medication RecommendationsNo ratings yet
- Financialmanagement 1Document3 pagesFinancialmanagement 1Sujatha J Jayabal100% (2)
- Evaluasi Penggunaan Antibiotika Berdasarkan Metode: Defined Daily Dose (DDD) Pada Pasien Ulkus DiabetikumDocument9 pagesEvaluasi Penggunaan Antibiotika Berdasarkan Metode: Defined Daily Dose (DDD) Pada Pasien Ulkus DiabetikumAzahrah Mawaddah IINo ratings yet
- Notices For The Application of Plant Master FileDocument7 pagesNotices For The Application of Plant Master FileAnandharaj AsaithambiNo ratings yet
- Advanced Cosmetic Sciences Admission Procedure 21-22 English AbstractDocument9 pagesAdvanced Cosmetic Sciences Admission Procedure 21-22 English AbstractTinotenda GambaraNo ratings yet
- Kansas Pharmaceutical Collaborative - 2006 CSG Innovations Award WinngerDocument6 pagesKansas Pharmaceutical Collaborative - 2006 CSG Innovations Award Winngerbvoit1895No ratings yet
- Technician Manual PDFDocument35 pagesTechnician Manual PDFMohamed RageNo ratings yet
- Bpharm 5 Sem Industrial Pharmacy 1 bp502t 2022Document1 pageBpharm 5 Sem Industrial Pharmacy 1 bp502t 2022Shaan MohammadNo ratings yet
- Sambungan Data Persediaan Obat PuskesmasDocument7 pagesSambungan Data Persediaan Obat PuskesmasMerry OctafiaNo ratings yet
- Formatting, Assembling, and Submitting The New Drug ApplicationDocument25 pagesFormatting, Assembling, and Submitting The New Drug ApplicationAgnimitra Dinda100% (1)
- 02-2 A History of Pharmacy in PicturesDocument39 pages02-2 A History of Pharmacy in Picturesnimona berhanuNo ratings yet
- 08-12-2022Document26 pages08-12-2022Hendy Kilat BuanaNo ratings yet
- Herbs, Laboratories, and RevolDocument15 pagesHerbs, Laboratories, and Revolhung tsung jenNo ratings yet
- Daftar Obat UgdDocument5 pagesDaftar Obat Ugddedi darmawanNo ratings yet
- Quick Review On All The Aphorisms of Organon of Medicine 6 EditionDocument11 pagesQuick Review On All The Aphorisms of Organon of Medicine 6 EditionVishalNo ratings yet
- Rational Use of MedicineDocument18 pagesRational Use of MedicineSteven A'Baqr EgiliNo ratings yet
- Dr. G Praveen KumarDocument36 pagesDr. G Praveen KumarMuhammad Riaz BhattiNo ratings yet
- Chapter 4: Multiple Choice Questions: InstructionsDocument16 pagesChapter 4: Multiple Choice Questions: InstructionsDavidNo ratings yet
- Data Analysis in Preclinical DevelopementDocument26 pagesData Analysis in Preclinical DevelopementOmkar KaleNo ratings yet
- Hospital Pharmacy Practice in Saudi Arabia: Dispensing and Administration in The Riyadh RegionDocument9 pagesHospital Pharmacy Practice in Saudi Arabia: Dispensing and Administration in The Riyadh RegionNisa SundariNo ratings yet
- MEDICAMENTOSDocument8 pagesMEDICAMENTOSPakinn ShadoowNo ratings yet
- List of Predator JournalsDocument31 pagesList of Predator JournalsVicko SuswidiantoroNo ratings yet
- Daily Activities of A Clinical PharmacistDocument20 pagesDaily Activities of A Clinical PharmacistAnoop Tandur0% (1)
- Perspectives of Hospital Administration in Geriatrics Care: Miguel A. Ramos JR., MD, PHDDocument4 pagesPerspectives of Hospital Administration in Geriatrics Care: Miguel A. Ramos JR., MD, PHDrnrmmanphdNo ratings yet
- Pre-Import Permit: CommodityDocument3 pagesPre-Import Permit: Commoditychristina tetemkeNo ratings yet
- Hospital Functions and Support Functions AssignmentDocument7 pagesHospital Functions and Support Functions AssignmentPrasoon BanerjeeNo ratings yet
- ECTD Tech Guide v1.1Document26 pagesECTD Tech Guide v1.1DontYou KnowMeNo ratings yet
- FDA EUA Covid-19 TestsDocument3 pagesFDA EUA Covid-19 TestsActionNewsJaxNo ratings yet
- AUC and Clearance-Drug CalculationsDocument6 pagesAUC and Clearance-Drug CalculationsManikanta GupthaNo ratings yet