POGI Preclampsia 2022
POGI Preclampsia 2022
Download as pdf or txt
You might also like
- 1000 Drug CardsDocument33 pages1000 Drug CardsJelly Bean100% (1)
- Eclampsia: History and Physical Examination Seizure Activity Blood Pressure Monitoring Laboratory Tests UrinalysisDocument1 pageEclampsia: History and Physical Examination Seizure Activity Blood Pressure Monitoring Laboratory Tests UrinalysisjanNo ratings yet
- Hypertensive Disorders in Pregnancy: Maisuri T. ChalidDocument44 pagesHypertensive Disorders in Pregnancy: Maisuri T. ChalidinhaNo ratings yet
- Douglas A. Woelkers, MD Associate Professor of Reproductive Medicine University of California, San DiegoDocument36 pagesDouglas A. Woelkers, MD Associate Professor of Reproductive Medicine University of California, San DiegoongkisawooNo ratings yet
- Case Study Preeclampsia FinDocument5 pagesCase Study Preeclampsia FinAngel Clarisse JariolNo ratings yet
- PathophysiologyDocument2 pagesPathophysiologyNERISSA CABRIADASNo ratings yet
- Hipertensi Dalam Kehamilan FK Unizar DR AdipDocument68 pagesHipertensi Dalam Kehamilan FK Unizar DR AdipAngga FirmansyahNo ratings yet
- Hipertensi Dalam Kehamilan: Dr. Adib Ahmad S, SpogDocument68 pagesHipertensi Dalam Kehamilan: Dr. Adib Ahmad S, SpogNagib HadianNo ratings yet
- L3 Hypertension in PregnancyDocument35 pagesL3 Hypertension in Pregnancysenkchung86No ratings yet
- Preeclampsia: Dra. Merly Muñoz Espinosa Gineco - Obstetricia USCO 2008Document47 pagesPreeclampsia: Dra. Merly Muñoz Espinosa Gineco - Obstetricia USCO 2008Ilse Alejandra Tafolla DuarteNo ratings yet
- Preterm Labor and PROMDocument102 pagesPreterm Labor and PROMDan Matthew BuriasNo ratings yet
- Preeclampsia and EclampsiaDocument23 pagesPreeclampsia and Eclampsiaapi-3705046100% (6)
- CPR in Term Pregnancies-19Document23 pagesCPR in Term Pregnancies-19Blanca Herrera MoralesNo ratings yet
- Hypertension in Pregnancy 2Document41 pagesHypertension in Pregnancy 2gold gbaramoghoNo ratings yet
- Perinatal Asphyxia - Outline of Pathophysiology and Recent Trends in ManagementDocument31 pagesPerinatal Asphyxia - Outline of Pathophysiology and Recent Trends in Managementokwadha simionNo ratings yet
- Perioperative NotesDocument14 pagesPerioperative NotesGil GanibanNo ratings yet
- Case Study Drug AnaDocument7 pagesCase Study Drug AnaMagdaraog Gabrielle A.No ratings yet
- Pa Tho ReviseDocument10 pagesPa Tho ReviseCharl SembranoNo ratings yet
- Alejandra Vélez Perea Res. Ginecología y ObstetriciaDocument71 pagesAlejandra Vélez Perea Res. Ginecología y ObstetriciaMagic_OverNo ratings yet
- Endo-2 Hyperprolactinemia DIDocument40 pagesEndo-2 Hyperprolactinemia DIalhusien.abd2000No ratings yet
- Gyne - Feu ReviewerDocument87 pagesGyne - Feu ReviewerKoko RoqueNo ratings yet
- System Disorder: Active Learning TemplateDocument1 pageSystem Disorder: Active Learning TemplateEli Reyes100% (1)
- Paediatric Guidelines Acute Kidney Injury 2020Document5 pagesPaediatric Guidelines Acute Kidney Injury 2020Seri PriNo ratings yet
- Revision Cardiopatia PeripartoDocument21 pagesRevision Cardiopatia PeripartoAntonia PerezNo ratings yet
- NEONATOLOGI - Sepsis Neonatorum + TTN + Neo PneumoniaDocument18 pagesNEONATOLOGI - Sepsis Neonatorum + TTN + Neo PneumoniaGaluh Martin MaytasariNo ratings yet
- Renal: Cause of HTN Features Investigations PrimaryDocument9 pagesRenal: Cause of HTN Features Investigations PrimarySaadia JavaidNo ratings yet
- Hypertension in Pregnancy PDFDocument8 pagesHypertension in Pregnancy PDF001mahwishNo ratings yet
- Perdarahan Uterus DisfungsionalDocument22 pagesPerdarahan Uterus DisfungsionalAggiFitiyaningsihNo ratings yet
- Epidemiology, Prevention & Promotion For Cardiovascular Disease (CVD)Document43 pagesEpidemiology, Prevention & Promotion For Cardiovascular Disease (CVD)SriNoviantiNo ratings yet
- Early Pregnancy CME CBD 14.6Document29 pagesEarly Pregnancy CME CBD 14.6Alice KaariaNo ratings yet
- Cerebral PalsyDocument152 pagesCerebral PalsyPrateek Kumar PandaNo ratings yet
- Cholestatic Liver DiseaseDocument35 pagesCholestatic Liver DiseasealnyhilwanyNo ratings yet
- Preventing Elective Deliveries Before 39 WeeksDocument11 pagesPreventing Elective Deliveries Before 39 WeekskcochranNo ratings yet
- Menstrual DisordersDocument29 pagesMenstrual DisorderstuhinsinghNo ratings yet
- Addison's Disease FileDocument25 pagesAddison's Disease FileZyla KrisshaNo ratings yet
- Prediction, Prevention, and Prognosis of Preeclampsia: RecommendationsDocument8 pagesPrediction, Prevention, and Prognosis of Preeclampsia: RecommendationskunkkonkNo ratings yet
- Wa0004.Document72 pagesWa0004.Huda AbdelfattahNo ratings yet
- Dr. Ashon Sa'adiDocument33 pagesDr. Ashon Sa'adianindhita_vania100% (1)
- Caisip NCM109Document3 pagesCaisip NCM109Vannesa TarifaNo ratings yet
- Infertility Current DX TXDocument12 pagesInfertility Current DX TXEkanita DesianiNo ratings yet
- Iem-Lect-6.1.2022 2Document56 pagesIem-Lect-6.1.2022 2kxdptqbsvsNo ratings yet
- Pembahasan To Online 3Document201 pagesPembahasan To Online 3Fate DreamworkNo ratings yet
- Pre Eclampsia & Hellp Syndrome Pre Eclampsia & Hellp SyndromeDocument19 pagesPre Eclampsia & Hellp Syndrome Pre Eclampsia & Hellp Syndromewidya AudistiNo ratings yet
- Pediatric DiseasesDocument36 pagesPediatric DiseasesSitti MutmainnahNo ratings yet
- Placenta Previa Case StudyDocument7 pagesPlacenta Previa Case StudyKing NavsunNo ratings yet
- Acute Kidney Injury (ARF)Document23 pagesAcute Kidney Injury (ARF)Aizaz AhmadNo ratings yet
- Pre EclampsiaDocument12 pagesPre EclampsiaLady Jane CaguladaNo ratings yet
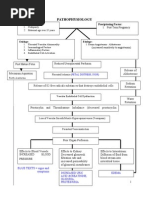
- PATHOPHYSIOLOGYDocument2 pagesPATHOPHYSIOLOGYPerl AngelicNo ratings yet
- Boala Basedow Graves FinalDocument112 pagesBoala Basedow Graves Finalandrutza37100% (1)
- Etiology and Evaluation of Abnormal Uterine BleedingDocument13 pagesEtiology and Evaluation of Abnormal Uterine BleedingSilva RahmaNo ratings yet
- Name of Drug Classification Mechanism of Action Indication Contraindication Side Effects Nursing ResponsibilitiesDocument4 pagesName of Drug Classification Mechanism of Action Indication Contraindication Side Effects Nursing ResponsibilitiesStephen VillegasNo ratings yet
- Medical Nutrition Therapy For Neuropsychiatric DisorderDocument52 pagesMedical Nutrition Therapy For Neuropsychiatric DisorderSavira setyoningsihNo ratings yet
- Pregnancy Induced HypertensionDocument38 pagesPregnancy Induced HypertensionЕрнур КасымбаевNo ratings yet
- PROF SURYANI-Medical Nutrition Therapy NeuroDocument52 pagesPROF SURYANI-Medical Nutrition Therapy NeuroAsriNo ratings yet
- Evaluation and Diagnosis of The Dysmorphic InfantDocument19 pagesEvaluation and Diagnosis of The Dysmorphic Infantcamila.belloarellanoNo ratings yet
- Acute Fatty Liver TOGDocument5 pagesAcute Fatty Liver TOGS_XangaiNo ratings yet
- Systemic Lupus 1Document15 pagesSystemic Lupus 1ANNAMA3 SELMERNo ratings yet
- History Lab Investigation: EclampsiaDocument5 pagesHistory Lab Investigation: EclampsiaShafiq Ur RahmanNo ratings yet
- Emergencies in Diabetes: Diagnosis, Management and PreventionFrom EverandEmergencies in Diabetes: Diagnosis, Management and PreventionNo ratings yet
- Infection Control in A Dental Laboratory 1Document2 pagesInfection Control in A Dental Laboratory 1Lynne SoloriaNo ratings yet
- Exclusive BreastfeedingDocument19 pagesExclusive BreastfeedingVANGAWA JOHNNo ratings yet
- Restaurant Report Card: September 14, 2023Document5 pagesRestaurant Report Card: September 14, 2023KBTXNo ratings yet
- Medical Eligibility Criteria 2009Document9 pagesMedical Eligibility Criteria 2009dzakyNo ratings yet
- Hep B Declination - Fillable 2Document1 pageHep B Declination - Fillable 2navneetshekhar.11No ratings yet
- Handwashing QuestionsDocument2 pagesHandwashing Questionsknicky FranciscoNo ratings yet
- Thesis Paper On SyphilisDocument7 pagesThesis Paper On Syphiliskulilev0bod3100% (4)
- Dr. Cissy PKB BOGOR 17032018Document46 pagesDr. Cissy PKB BOGOR 17032018boy bionardoNo ratings yet
- The Soundness of MindDocument14 pagesThe Soundness of MindAnonymous oQEx3zNo ratings yet
- Problems With The PassageDocument13 pagesProblems With The PassageMaria Theresa BuscasNo ratings yet
- Diagnosis of Helicobacter Pylori InfectionDocument50 pagesDiagnosis of Helicobacter Pylori InfectionErik Sesuatu BangeetNo ratings yet
- BCPCDocument4 pagesBCPCjocelyn081078No ratings yet
- COVID 19 Briefing Note April 13 2020Document9 pagesCOVID 19 Briefing Note April 13 2020Aristegui NoticiasNo ratings yet
- Health Teaching Plan FormDocument2 pagesHealth Teaching Plan FormChadd Vyllmorr VillarinNo ratings yet
- English Semester 2Document7 pagesEnglish Semester 2Abdullah AbidNo ratings yet
- Silliman University: Immediate Postpartum CareDocument5 pagesSilliman University: Immediate Postpartum CarealorNo ratings yet
- Microorganisms Class 8Document7 pagesMicroorganisms Class 8Ambika LalNo ratings yet
- Detailed Speakers Listing 2-25-11Document14 pagesDetailed Speakers Listing 2-25-11magfound4mpNo ratings yet
- 49 Field Guidance 21Document6 pages49 Field Guidance 21CBS NewsNo ratings yet
- Institutional Hand Hygine - Review - Manjiri GajmalDocument13 pagesInstitutional Hand Hygine - Review - Manjiri Gajmalmanjirigajmal07No ratings yet
- Why and How Vaccines WorkDocument6 pagesWhy and How Vaccines WorkAniruddha RoyNo ratings yet
- Etiologi Dan Gejala Klinis Pneumonia RevisiDocument15 pagesEtiologi Dan Gejala Klinis Pneumonia Revisiazis purwantoNo ratings yet
- Design and Planning of Sanitation System in Rajbari DistrictDocument8 pagesDesign and Planning of Sanitation System in Rajbari DistrictMd. Habibur Rahman Bejoy Khan ,155408No ratings yet
- CHICKEN POX Genesis CarandangDocument10 pagesCHICKEN POX Genesis CarandangGenEsis CarandangNo ratings yet
- Kettering Business PlanDocument22 pagesKettering Business PlanfrankNo ratings yet
- Question Bank 2Document6 pagesQuestion Bank 2Mohamed abdelhadiNo ratings yet
- AnimalDocument27 pagesAnimaljessalyn iladaNo ratings yet
- 7636 24127 1 PBDocument6 pages7636 24127 1 PBWIDYA ELISABETH SILALAHI2020BLOK 1No ratings yet
- Journal: Scabies New Opportunities For Management and Population ControlDocument11 pagesJournal: Scabies New Opportunities For Management and Population Controladeta yunizaNo ratings yet
- Fresh Frozen FoodDocument28 pagesFresh Frozen FoodsekoudaramieNo ratings yet