6 Alt
6 Alt
Download as doc, pdf, or txt
You might also like
- SASII Standard Short Form With Supplemental QuestionsDocument17 pagesSASII Standard Short Form With Supplemental QuestionsRaquel MalheirosNo ratings yet
- Teco Diagnostics: Alt (SGPT) Liquid Reagent (Kinetic Method)Document2 pagesTeco Diagnostics: Alt (SGPT) Liquid Reagent (Kinetic Method)Wendy ZacaríasNo ratings yet
- 9 AstDocument7 pages9 AstAzhar Clinical Laboratory TubeNo ratings yet
- 5-Alkaline PhosphataseDocument7 pages5-Alkaline PhosphataseAzhar Clinical Laboratory TubeNo ratings yet
- 12 CKLDocument7 pages12 CKLAzhar Clinical Laboratory TubeNo ratings yet
- 7 AmmoniaDocument7 pages7 AmmoniaAzhar Clinical Laboratory TubeNo ratings yet
- ALTL enDocument3 pagesALTL enyolanda0811No ratings yet
- 14 CreatinineDocument8 pages14 CreatinineAzhar Clinical Laboratory TubeNo ratings yet
- 10 AlciumDocument9 pages10 AlciumAzhar Clinical Laboratory TubeNo ratings yet
- 8 AmylaseDocument9 pages8 AmylaseAzhar Clinical Laboratory TubeNo ratings yet
- 4 AlbuminDocument6 pages4 AlbuminAzhar Clinical Laboratory TubeNo ratings yet
- Sop of Alkaline PhosphataseDocument6 pagesSop of Alkaline PhosphataseUMMID WashimNo ratings yet
- AAGP2 enDocument3 pagesAAGP2 enLince WijoyoNo ratings yet
- 13 CKMBDocument8 pages13 CKMBAzhar Clinical Laboratory TubeNo ratings yet
- AAT2 enDocument3 pagesAAT2 enSyahdie FahledieNo ratings yet
- Bilirubin Total Blosr6x12 enDocument2 pagesBilirubin Total Blosr6x12 enMeethuanNo ratings yet
- Laboratory-Exercise-Total-Protein-1Document10 pagesLaboratory-Exercise-Total-Protein-1hcqt9cvss7No ratings yet
- En - Lactate DehydrogenaseDocument2 pagesEn - Lactate DehydrogenasecarineNo ratings yet
- Transferrin: OSR6152 4 X 7 ML R1 4 X 8 ML R2Document2 pagesTransferrin: OSR6152 4 X 7 ML R1 4 X 8 ML R2TanveerNo ratings yet
- ACCENT-200 ALPHA-FETOPROTEIN ADocument2 pagesACCENT-200 ALPHA-FETOPROTEIN Aemc.medicalserviceNo ratings yet
- Euro CRP TurbilatexDocument2 pagesEuro CRP TurbilatexDharmesh Patel100% (1)
- ACCENT-200 ALAT ADocument2 pagesACCENT-200 ALAT Aemc.medicalserviceNo ratings yet
- (ADA) Package Insert (CE)Document31 pages(ADA) Package Insert (CE)Sinari AlfatNo ratings yet
- 6.POTASSIUM EnzymaticDocument2 pages6.POTASSIUM EnzymaticHiếu Chí PhanNo ratings yet
- Bilirubin Direct Blosr6x11 enDocument2 pagesBilirubin Direct Blosr6x11 enMeethuanNo ratings yet
- CT10282Document4 pagesCT10282KOUAME EDYMAIN FRANCISNo ratings yet
- Crp-Ultra 43134Document2 pagesCrp-Ultra 43134Đỗ Quốc MạnhNo ratings yet
- Bsis13-I Creatinina 2014Document1 pageBsis13-I Creatinina 2014Alejandra MoralesNo ratings yet
- CALCIUM CPC+STD ANG 2015 02 17Document2 pagesCALCIUM CPC+STD ANG 2015 02 17yehiwal756No ratings yet
- ALBUMIN BLOSR6x02 ENDocument2 pagesALBUMIN BLOSR6x02 ENMeethuanNo ratings yet
- C-Reactive Protein: TurbilatexDocument1 pageC-Reactive Protein: TurbilatexAssane Senghor100% (1)
- Generic Name: High Sensitivity C-Reaction Protein Kit Abbreviated name:HS-CRP Order InformationDocument36 pagesGeneric Name: High Sensitivity C-Reaction Protein Kit Abbreviated name:HS-CRP Order InformationSharom Zelene Cordova RomanNo ratings yet
- LDH 110 - Xsys0013 - eDocument4 pagesLDH 110 - Xsys0013 - eYousra ZeidanNo ratings yet
- MK055 ADA Assay 040615Document2 pagesMK055 ADA Assay 040615Smithesh TpNo ratings yet
- Fluitest U/Csf: Ultrasensitive ProteinDocument4 pagesFluitest U/Csf: Ultrasensitive ProteinDarko MaksimovicNo ratings yet
- Budi Altgpt - Doc NewDocument3 pagesBudi Altgpt - Doc NewIrvanda ENVIOUSNo ratings yet
- Autopure T LDL-C: Specimen Collection & PreservationDocument2 pagesAutopure T LDL-C: Specimen Collection & PreservationNanda Nabilah UbayNo ratings yet
- Ifu 1418 1092 LactateDocument1 pageIfu 1418 1092 LactateLê Văn DươngNo ratings yet
- 1.alpha AmylaseDocument2 pages1.alpha AmylaseHiếu Chí PhanNo ratings yet
- LDHI2 enDocument3 pagesLDHI2 enArnaz AdisaputraNo ratings yet
- Lab Policies Alkaline Phosphatase C311 Lab 8803Document4 pagesLab Policies Alkaline Phosphatase C311 Lab 8803Valdez Francis ZaccheauNo ratings yet
- C Reactive Protein CRP TurbilatexDocument2 pagesC Reactive Protein CRP Turbilatexmicklemagdy50No ratings yet
- RF TurbilatexDocument2 pagesRF TurbilatexAhmed YhyaNo ratings yet
- CL 0100 CH 2 X 50 ML CL 0500 CH 4 X 125 ML: in Vitro Diagnostic Medical DeviceDocument1 pageCL 0100 CH 2 X 50 ML CL 0500 CH 4 X 125 ML: in Vitro Diagnostic Medical DeviceBPG ServiceNo ratings yet
- Amylase enDocument1 pageAmylase enRakib Hossain 3A-159No ratings yet
- Sop of Interleukin-6 (IL-6) Testing: A.PurposeDocument7 pagesSop of Interleukin-6 (IL-6) Testing: A.PurposeUMMID WashimNo ratings yet
- KR10060Document2 pagesKR10060KOUAME EDYMAIN FRANCISNo ratings yet
- Generic Name: 5 - Nucleotidase Kit Abbreviated Name: 5 - NT Order Information Cat. No. Package SizeDocument30 pagesGeneric Name: 5 - Nucleotidase Kit Abbreviated Name: 5 - NT Order Information Cat. No. Package SizeSharom Zelene Cordova RomanNo ratings yet
- Amy2 JS01Document2 pagesAmy2 JS01Inversiones Llanolab, c.a. LlanolabNo ratings yet
- Turbitex ASL: Antistreptolysin-ODocument4 pagesTurbitex ASL: Antistreptolysin-ODarko MaksimovicNo ratings yet
- Alkaline Phosphatase LiquicolorDocument2 pagesAlkaline Phosphatase LiquicolorDaniel LaraNo ratings yet
- Altl 2017-01 v12Document4 pagesAltl 2017-01 v12Edymain Francis KouaméNo ratings yet
- LDHL Opt enDocument3 pagesLDHL Opt enArnaz AdisaputraNo ratings yet
- Promotion & Discount Pricelist/CatalogDocument49 pagesPromotion & Discount Pricelist/CatalogShoukrey AusmanNo ratings yet
- Human IL-6 RalphaDocument2 pagesHuman IL-6 RalphapavangchettyNo ratings yet
- Cre2 JS01Document2 pagesCre2 JS01Inversiones Llanolab, c.a. LlanolabNo ratings yet
- Standard Operating Procedure For Testing Aspartate Aminotransferase (AST)Document7 pagesStandard Operating Procedure For Testing Aspartate Aminotransferase (AST)kahlilNo ratings yet
- 3478-Crpturbi v2.10 enDocument4 pages3478-Crpturbi v2.10 enxuanhungyteNo ratings yet
- CA Calcio MindrayDocument32 pagesCA Calcio Mindrayjcpc272005100% (1)
- CRP BiolatexDocument2 pagesCRP BiolatexN. K. MandilNo ratings yet
- 10 AlciumDocument9 pages10 AlciumAzhar Clinical Laboratory TubeNo ratings yet
- 13 CKMBDocument8 pages13 CKMBAzhar Clinical Laboratory TubeNo ratings yet
- AutoimmunediseaseDocument87 pagesAutoimmunediseaseAzhar Clinical Laboratory TubeNo ratings yet
- Diagnosis of Autoimmune Diseases: Presented By, S.Nagaraj, M.Sc. 3 YearDocument51 pagesDiagnosis of Autoimmune Diseases: Presented By, S.Nagaraj, M.Sc. 3 YearAzhar Clinical Laboratory TubeNo ratings yet
- Hiv CBL 2Document6 pagesHiv CBL 2Azhar Clinical Laboratory TubeNo ratings yet
- Antigenandantibodyreaction 120515041533 Phpapp01Document44 pagesAntigenandantibodyreaction 120515041533 Phpapp01Azhar Clinical Laboratory TubeNo ratings yet
- Lesson 25: Heath: Medical and DentalDocument19 pagesLesson 25: Heath: Medical and DentalEasy WriteNo ratings yet
- BaumRP 2021-02-21 Bern Winter School Dosimetry NET&PSMA PDF VersionDocument73 pagesBaumRP 2021-02-21 Bern Winter School Dosimetry NET&PSMA PDF VersionRobert B. SklaroffNo ratings yet
- Anxiety NCPDocument8 pagesAnxiety NCPJULIANNE BAYHONNo ratings yet
- RMST Brochure PeersDocument2 pagesRMST Brochure Peersapi-272816420No ratings yet
- Childhood Cancer Resources Directory Asia - Final v170908Document35 pagesChildhood Cancer Resources Directory Asia - Final v170908Anna VieeNo ratings yet
- Revision 3,4 - TACN (U1-6)Document9 pagesRevision 3,4 - TACN (U1-6)kimchicute8No ratings yet
- Nursing Care PlanDocument22 pagesNursing Care PlanjamNo ratings yet
- Clinical Pathology of Mother Tinctures &lower PotenciesDocument64 pagesClinical Pathology of Mother Tinctures &lower PotenciesAntony antony100% (2)
- Hancock PPT Chapter 03Document19 pagesHancock PPT Chapter 03Olivia OssegeNo ratings yet
- Angina PostprandialDocument10 pagesAngina PostprandialJoaquín SosaNo ratings yet
- Comparison RepertoryDocument3 pagesComparison RepertorySuhasSkyNo ratings yet
- CPS-guidelines-bronchiolitis 2Document8 pagesCPS-guidelines-bronchiolitis 2tessa wulandariNo ratings yet
- 118 RLE Suction PDFDocument4 pages118 RLE Suction PDFclaire yowsNo ratings yet
- Urine Complete Examination: Colour Appearance PHDocument2 pagesUrine Complete Examination: Colour Appearance PHSeshagiri DeenadayaluNo ratings yet
- Hand Out Ppavd.Document4 pagesHand Out Ppavd.Hæłíę SikuarieNo ratings yet
- Daftar Pustaka Marwah NH 1210312044Document4 pagesDaftar Pustaka Marwah NH 1210312044Linda WijayantiNo ratings yet
- Snake Bite RSPBDocument57 pagesSnake Bite RSPBVania Azalia HariyantoNo ratings yet
- Hna Produk Pharos IndonesiaDocument56 pagesHna Produk Pharos IndonesiaMuhammadIqbal100% (1)
- Tugas Bahasa InggrisDocument4 pagesTugas Bahasa InggrisRini AriskawatiNo ratings yet
- Par Format For Physiotherapy of NHM OdishaDocument7 pagesPar Format For Physiotherapy of NHM Odishakrishna bptNo ratings yet
- Late Diagnosis of Hereditary Tyrosinemia Type I: The Case of Two First CousinsDocument3 pagesLate Diagnosis of Hereditary Tyrosinemia Type I: The Case of Two First CousinsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- NCP Activity IntoleranceDocument3 pagesNCP Activity IntoleranceWyen CabatbatNo ratings yet
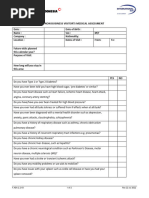
- Form Non Business Visitors Medical Assessment (New)Document2 pagesForm Non Business Visitors Medical Assessment (New)franciscus.santosoNo ratings yet
- Biology Medicine and Surgery of South American Wild Animals - 2001 - FowlerDocument6 pagesBiology Medicine and Surgery of South American Wild Animals - 2001 - FowlerallthoseNo ratings yet
- Velasof PillsbagDocument6 pagesVelasof Pillsbagvijayalakshmi JanakiramanNo ratings yet
- Clinical Pharmacology IntroductionDocument24 pagesClinical Pharmacology IntroductionSunilNo ratings yet
- 6887 25815 1 PB PDFDocument7 pages6887 25815 1 PB PDFmochkurniawanNo ratings yet
- Esophageal DiverticulaDocument18 pagesEsophageal DiverticulaAbigail BascoNo ratings yet
- NCM 117-Somatic DisordersDocument5 pagesNCM 117-Somatic DisordersJa DimasNo ratings yet