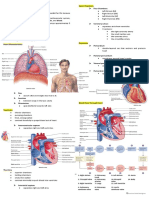
Cardiac Module - Cardio Anaphy
Cardiac Module - Cardio Anaphy
Download as pdf or txt
You might also like
- Cardiovascular Notes - All in One FileDocument299 pagesCardiovascular Notes - All in One FileHasan DiabNo ratings yet
- Cardiovascular System Heart ReviewerDocument8 pagesCardiovascular System Heart ReviewerImmanuel Cris Palasigue100% (1)
- Cardio TransDocument7 pagesCardio TransweissNo ratings yet
- Anatomy: Heart and PericardiumDocument95 pagesAnatomy: Heart and PericardiumDitas Chu100% (1)
- Analec Finals 1Document22 pagesAnalec Finals 1ms.maeosanoNo ratings yet
- Medsurg Cardio Ana&PhysioDocument6 pagesMedsurg Cardio Ana&Physiorabsibala83% (12)
- ... 4 Finals Cardiovascular PhysiologyDocument8 pages... 4 Finals Cardiovascular PhysiologyELIZABETH GRACE AMADORNo ratings yet
- Cardio Pulmo NotesDocument12 pagesCardio Pulmo NotesCherrie MaeNo ratings yet
- Cardiopulmonary System: Relevant Anatomy & Physiology: HeartDocument12 pagesCardiopulmonary System: Relevant Anatomy & Physiology: HeartJulia SalvioNo ratings yet
- Crat - Cardio PulmoDocument11 pagesCrat - Cardio PulmoJULIANE MAE BALANGNo ratings yet
- 3 - Intro, To CVS Lymphatic SystemDocument63 pages3 - Intro, To CVS Lymphatic Systemahmedmustefa773No ratings yet
- Cardiovascular SystemDocument5 pagesCardiovascular Systemy30ny30nNo ratings yet
- Circulatory System TOPIC 4Document52 pagesCirculatory System TOPIC 4epifaniopilapil48No ratings yet
- Cardiovascular SystemDocument57 pagesCardiovascular SystemSarah Shane Cortes CortesNo ratings yet
- HEARTDocument8 pagesHEARTRoeisa SalinasNo ratings yet
- Cardiovascular System - ReviewerDocument11 pagesCardiovascular System - ReviewerEva Marie GaaNo ratings yet
- 1205 Cardiovascvular PDFDocument29 pages1205 Cardiovascvular PDFDhanica B. FiguracionNo ratings yet
- HeartDocument8 pagesHeartrandomdomram12No ratings yet
- REVIEW OF ANAPHY OF CARDIOVASCULAR SYSTEMDocument2 pagesREVIEW OF ANAPHY OF CARDIOVASCULAR SYSTEMJireh Dominguez SapnuNo ratings yet
- A&p - All Files in OneDocument87 pagesA&p - All Files in OneRohan PackiarajNo ratings yet
- Anaphy CardioDocument6 pagesAnaphy CardioDianne DimaanoNo ratings yet
- Anaphy - MOD 3 (Midterms)Document7 pagesAnaphy - MOD 3 (Midterms)smzw4r78sqNo ratings yet
- 3.1 Systemic NoteDocument7 pages3.1 Systemic NoteMekuriya BeregaNo ratings yet
- A&P - 1. Heart Anatomy (9p)Document9 pagesA&P - 1. Heart Anatomy (9p)mr. fakeNo ratings yet
- Circulatory System PearsonsDocument16 pagesCirculatory System Pearsonsblando.shaneNo ratings yet
- Anaphy Lec CardioDocument12 pagesAnaphy Lec CardioRyan Dave UmayamNo ratings yet
- Cardiovascular SystemDocument20 pagesCardiovascular SystemFisco DessereiNo ratings yet
- Anatomy of The Heart - Dr. Wael Amin - 6 March 2024Document33 pagesAnatomy of The Heart - Dr. Wael Amin - 6 March 2024ciyace7849No ratings yet
- HEARTDocument8 pagesHEARTSJane Feria100% (1)
- Cardiovascular System - Mcon 01 (Lec) A4Document6 pagesCardiovascular System - Mcon 01 (Lec) A4Lemon AdeNo ratings yet
- Cardiovascular SystemDocument8 pagesCardiovascular SystemChelsie NicoleNo ratings yet
- Cardiopulmo Notes 2ndDocument12 pagesCardiopulmo Notes 2ndCherrie MaeNo ratings yet
- Structure of The Heart TransesDocument6 pagesStructure of The Heart TransesReign SaplacoNo ratings yet
- Basic Anatomy & Physiology: Cardiovascular Heart AnatomyDocument16 pagesBasic Anatomy & Physiology: Cardiovascular Heart AnatomyLalu Ahmad AsmayadiNo ratings yet
- Cardiovascular System - Printable Pages - MariebDocument6 pagesCardiovascular System - Printable Pages - MariebChristal Rae Tac-anNo ratings yet
- The Heart - Chapter 12 Cardiovascular System Functions of The HeartDocument10 pagesThe Heart - Chapter 12 Cardiovascular System Functions of The HeartLol lolNo ratings yet
- Cadiovascular System Iandii: School of Laboratory Medicine and Medical Sciences Anatomy 2022Document38 pagesCadiovascular System Iandii: School of Laboratory Medicine and Medical Sciences Anatomy 2022Humaira BadatNo ratings yet
- Anaphy Reviewer MidtermDocument30 pagesAnaphy Reviewer Midtermjuayma maureen importanteNo ratings yet
- 01 HeartDocument39 pages01 HeartFahvy tvNo ratings yet
- Cardiac Conduction System Power Point PresentationDocument30 pagesCardiac Conduction System Power Point PresentationAaya AdelNo ratings yet
- The Cardiovascular System: Group 1Document92 pagesThe Cardiovascular System: Group 1Jefferson AdralesNo ratings yet
- Chapter 11 - Cardiovascular SystemDocument10 pagesChapter 11 - Cardiovascular SystemrishellemaepilonesNo ratings yet
- Med Surg CardioDocument18 pagesMed Surg CardioRianne Marie MarasiganNo ratings yet
- Chapter 12: HEARTDocument2 pagesChapter 12: HEARTPrecious Faith RodriguezNo ratings yet
- Cardiology NotesDocument31 pagesCardiology Noteshoedward29No ratings yet
- 1 Cardiovascular System (FINAL) PDFDocument11 pages1 Cardiovascular System (FINAL) PDFJohn Juan TwanNo ratings yet
- Cardiovascular SampleDocument31 pagesCardiovascular Sampleyetti TrisnaNo ratings yet
- I. Intro To Cardio: Pericardial FluidDocument5 pagesI. Intro To Cardio: Pericardial FluidElle Ricab EnimesNo ratings yet
- Reviewer 2 Health AssessmentDocument13 pagesReviewer 2 Health AssessmentchristinejeancenabreNo ratings yet
- 09:23 - The Mediastinum PDFDocument42 pages09:23 - The Mediastinum PDFVidya BalaNo ratings yet
- 01AKA Cardiac Muscle and Conduction System of the HeartDocument32 pages01AKA Cardiac Muscle and Conduction System of the Heartmogalmog0909No ratings yet
- Cardiovascular System ATU (Autosaved)Document58 pagesCardiovascular System ATU (Autosaved)maxwell amponsahNo ratings yet
- BIO101 Student Notes PREFINAL the Cardiovascular SytemDocument7 pagesBIO101 Student Notes PREFINAL the Cardiovascular SytemMa. Elaisa BaugbogNo ratings yet
- Transes - Heart and Neck VesselsDocument5 pagesTranses - Heart and Neck VesselscamatoviancaNo ratings yet
- Anatomy of The Heart AssignmentDocument10 pagesAnatomy of The Heart AssignmentKarim AL-TijaniNo ratings yet
- Assessing Heart and Neck Vessel Heart Heart Chambers: (Tricuspid & Bicuspid)Document7 pagesAssessing Heart and Neck Vessel Heart Heart Chambers: (Tricuspid & Bicuspid)Dan Floyd FernandezNo ratings yet
- Anaphy Lab CardioDocument3 pagesAnaphy Lab CardioRyan Dave UmayamNo ratings yet
- 1-Anatomy of The HeartDocument30 pages1-Anatomy of The Hearta730482776No ratings yet
- 24-25 BMSN1601 - Anatomy of Heart, Blood Vessels Lymphatic SystemDocument32 pages24-25 BMSN1601 - Anatomy of Heart, Blood Vessels Lymphatic Systemming sum lawNo ratings yet
- Immediate Life Support for healthcare Practitioners: A Step-By-Step GuideFrom EverandImmediate Life Support for healthcare Practitioners: A Step-By-Step GuideNo ratings yet
- So TabDocument22 pagesSo TabdewakusumaNo ratings yet
- Open Bite - Spectrum of Treatment Potentials and LimitationsDocument20 pagesOpen Bite - Spectrum of Treatment Potentials and LimitationsDr.Thrivikhraman KothandaramanNo ratings yet
- Muhamad Khairul Ilham (230106122)Document6 pagesMuhamad Khairul Ilham (230106122)Dicky PratamaNo ratings yet
- Chest AuscultationDocument24 pagesChest AuscultationAtu KaushalNo ratings yet
- Anatomy Practice QuestionsDocument5 pagesAnatomy Practice Questionsfrank davidNo ratings yet
- Banerjee 2014Document2 pagesBanerjee 2014nithya_sendhilNo ratings yet
- Pectus Carinatum Pigeon ChestDocument2 pagesPectus Carinatum Pigeon ChestWulanSyafitriNo ratings yet
- Pyloric StenosisDocument18 pagesPyloric StenosisAnkita Samanta0% (1)
- Imaging in Neonatus MARS 2.0 - Dr. Indrastuti Normahayu, Sp. Rad-KDocument36 pagesImaging in Neonatus MARS 2.0 - Dr. Indrastuti Normahayu, Sp. Rad-KarifdeathsciethNo ratings yet
- Plastic Surgeon in MalaysiaDocument2 pagesPlastic Surgeon in MalaysiaAnusha NairNo ratings yet
- TREATMENT Algorithm For Bilateral Alveolarcleft Based On The Position of The Premaxillaand The Width of The Alveolar GapDocument7 pagesTREATMENT Algorithm For Bilateral Alveolarcleft Based On The Position of The Premaxillaand The Width of The Alveolar GapFranklin HaroNo ratings yet
- Ebstein AnomalyDocument14 pagesEbstein AnomalyNataliaMaedyNo ratings yet
- CV AgtDocument6 pagesCV AgtHafzhy TravelNo ratings yet
- Complications of Biliary T-Tubes After Choledochotomy: Original ArticleDocument4 pagesComplications of Biliary T-Tubes After Choledochotomy: Original ArticleBikash SahNo ratings yet
- Introduction To Radiology: For Medical Students CIIDocument66 pagesIntroduction To Radiology: For Medical Students CIImehdikhalid09No ratings yet
- Anatomy and Physiology QP 1st B.SCDocument2 pagesAnatomy and Physiology QP 1st B.SCSuchitaNo ratings yet
- Pediatric Emergency Medicine Log BookDocument5 pagesPediatric Emergency Medicine Log BookwaadNo ratings yet
- Ecg Abnormal 1-HpwDocument77 pagesEcg Abnormal 1-HpwAndre JuliantNo ratings yet
- V6 - Health CS VC Collectors 22.08.2023Document92 pagesV6 - Health CS VC Collectors 22.08.2023MdnowfalNo ratings yet
- Blood Vessels QuizDocument3 pagesBlood Vessels QuizxibsjddhsNo ratings yet
- Cataract and Lens Surgery (Mehdi Shajari (Editor) Etc.) (Z-Library)Document800 pagesCataract and Lens Surgery (Mehdi Shajari (Editor) Etc.) (Z-Library)Артем ПустовитNo ratings yet
- High-Risk Pregnancy TreatmentDocument1 pageHigh-Risk Pregnancy TreatmentdrsabitakumarigynaeNo ratings yet
- Dorsal SlitDocument5 pagesDorsal SlitarikaNo ratings yet
- Chapter 15 The Urinary SystemDocument97 pagesChapter 15 The Urinary SystemNoquillo FranzyNo ratings yet
- Fassbender 2020Document10 pagesFassbender 2020widyadariNo ratings yet
- Eee-Instr F432 - QDocument2 pagesEee-Instr F432 - QAdya ChatterjeeNo ratings yet
- Dental PricingDocument4 pagesDental PricingsolutionbeautyNo ratings yet
- Current Concepts in BlepharoplastyDocument11 pagesCurrent Concepts in BlepharoplastyRajinder Kumar Bassan100% (1)
- Burst FractureDocument4 pagesBurst FracturepuchioNo ratings yet
- Surgical Count PolicyDocument21 pagesSurgical Count Policyalibaalbake97No ratings yet