JAMA 2002 Bhutta 728 37
JAMA 2002 Bhutta 728 37
Uploaded by
BelenCopyright:
Available Formats
JAMA 2002 Bhutta 728 37
JAMA 2002 Bhutta 728 37
Uploaded by
BelenOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Copyright:
Available Formats
JAMA 2002 Bhutta 728 37
JAMA 2002 Bhutta 728 37
Uploaded by
BelenCopyright:
Available Formats
REVIEW
Cognitive and Behavioral Outcomes
of School-Aged Children
Who Were Born Preterm
A Meta-analysis
Adnan T. Bhutta, MBBS Context The cognitive and behavioral outcomes of school-aged children who were born
Mario A. Cleves, PhD preterm have been reported extensively. Many of these studies have methodological flaws
that preclude an accurate estimate of the long-term outcomes of prematurity.
Patrick H. Casey, MD
Objective To estimate the effect of preterm birth on cognition and behavior in school-
Mary M. Cradock, PhD aged children.
K. J. S. Anand, MBBS, DPhil Data Sources MEDLINE search (1980 to November 2001) for English-language
articles, supplemented by a manual search of personal files maintained by 2 of the
T
HE INFANT MORTALITY RATE IN authors.
the United States has de- Study Selection We included case-control studies reporting cognitive and/or be-
creased from more than 12 per havioral data of children who were born preterm and who were evaluated after their
1000 live births in 1980 to ap- fifth birthday if the attrition rate was less than 30%. From the 227 reviewed studies,
proximately 7 per 1000 live births in cognitive data from 15 studies and behavioral data from 16 studies were selected.
1998. This reduction in mortality has oc- Data Extraction Data on population demographics, study characteristics, and cog-
curred during a period when an increas- nitive and behavioral outcomes were extracted from each study, entered in a custom-
ing percentage of children have been ized database, and reviewed twice to minimize error. Differences between the mean
born preterm (⬍37 weeks) with low cognitive scores of cases and controls were pooled. Homogeneity across studies was
birth weights (LBWs) (⬍2500 g) or very formally tested using a general variance-based method and graphically using Gal-
LBWs (⬍1500 g).1 This decrease can be braith plots. Linear meta-analysis regression models were fitted to explore the impact
attributed to improvements in postna- of birth weight and gestational age on cognitive outcomes. Study-specific relative risks
(RRs) were calculated for the incidence of attention-deficit/hyperactivity disorder (ADHD)
tal care provided in the delivery rooms and pooled. Quality assessment of the studies was performed based on a 10-point
and neonatal intensive care units. scale. Publication bias was examined using Begg modified funnel plots and formally
This decrease in mortality is paral- tested using the Egger weighted-linear regression method.
leled by an increasing recognition of
Data Synthesis Among 1556 cases and 1720 controls, controls had significantly
neurodevelopmental disabilities in higher cognitive scores compared with children who were born preterm (weighted mean
these children at school age. A large difference, 10.9; 95% confidence interval [CI], 9.2-12.5). The mean cognitive scores
number of children who were born with of preterm-born cases and term-born controls were directly proportional to their birth
a LBW or preterm have adverse out- weight (R2 =0.51; P⬍.001) and gestational age (R2 =0.49; P⬍.001). Age at evaluation
comes such as cerebral palsy, hydro- had no significant correlation with mean difference in cognitive scores (R2 =0.12; P=.20).
cephalus, blindness, deafness, or sei- Preterm-born children showed increases in externalizing and internalizing behaviors
zures.2-4 Multiple observational studies in 81% of studies and had more than twice the RR for developing ADHD (pooled RR,
of children who were born preterm have 2.64; 95% CI, 1.85-3.78). No differences were noted in cognition and behaviors based
on the quality of the study.
followed up cohorts from birth to
school age (ⱖ5 years) and have re- Conclusions Children who were born preterm are at risk for reduced cognitive test
ported on their cognitive and behav- scores and their immaturity at birth is directly proportional to the mean cognitive scores
at school age. Preterm-born children also show an increased incidence of ADHD and
ioral outcomes. Even in children with-
other behaviors.
out obvious neurological deficits, subtle
JAMA. 2002;288:728-737 www.jama.com
abnormalities occur, which include
Author Affiliations are listed at the end of this MBBS, DPhil, Arkansas Children’s Hospital, 800
lower cognitive test scores and in- article. Marshall St, S-431, Little Rock, AR 72202 (e-mail:
creased behavioral problems.5,6 How- Corresponding Author and Reprints: K. J. S. Anand, anandsunny@exchange.uams.edu).
728 JAMA, August 14, 2002—Vol 288, No. 6 (Reprinted) ©2002 American Medical Association. All rights reserved.
Downloaded from jama.ama-assn.org by guest on June 2, 2011
COGNITION AND BEHAVIOR OF CHILDREN BORN PRETERM
ever, some studies have found no dif- to English-language publications, and it erature.8,9,12-14 The data extracted from
ferences between preterm-born cases was supplemented by a manual search these studies were entered in an open-
and term-born controls.7 of the reference lists of all primary articles ended fashion and coding of the vari-
The magnitude of the effect of pre- and review articles. No attempt was made ables at the time of data entry was mini-
term birth on cognitive and behav- to contact the authors of any of these mized. The data from each study were
ioral outcomes at school age is un- studies. We also performed a manual reviewed twice to minimize the chances
known. The extreme variability in the search of files maintained by 2 coau- of data-entry errors. A wide array of be-
published data results from the rela- thors (P.H.C. and K.J.S.A.). haviors were assessed and various be-
tively small numbers of subjects in each We defined a priori criteria for the in- havioral methods were used in the se-
study and marked variation in the meth- clusion of studies in this meta-analysis, lected studies. For the purposes of this
ods used for their evaluation. Several selecting only those studies that in- meta-analysis, we classified the behav-
of these studies have been criticized due cluded an evaluation of concurrent con- ior of subjects into externalizing behav-
to problems with study design, non- trols. Studies were included if they (1) iors (eg, hyperactivity, delinquency) or
representative study samples, inad- had a case-control design, (2) reported internalizing behaviors (eg, anxiety, de-
equate demographic data, high attri- cognitive data, behavioral data or both, pression, phobias). Data from studies
tion rates, poor selection of control (3) performed evaluations after the fifth that used standard diagnostic criteria for
groups, the systematic exclusion of sub- birthday of the enrolled subjects, (4) had attention-deficit/hyperactivity disor-
groups of patients, and other con- an attrition rate (loss to follow-up) of less der (ADHD), either the Diagnostic and
cerns.8 This has led to difficulties in es- than 30%, and (5) were published in Statistical Manual of Mental Disorders,
timating the true effect of preterm birth 1980 or later. Studies were excluded if Third Edition (DSM-III), Diagnostic and
on cognition and behavior problems. they did not meet all of these inclusion Statistical Manual of Mental Disorders, Re-
We performed a meta-analysis to ar- criteria. Studies that primarily exam- vised Third Edition (DSM-III-R), or Di-
rive at a better estimate of the effect of ined LBW children were excluded be- agnostic and Statistical Manual of Men-
preterm birth on cognitive and behav- cause of the possibility that small-for- tal Disorders, Fourth Edition (DSM-IV),
ioral outcomes in school-aged chil- gestational-age term infants may be were extracted for further analysis.
dren. The 2 available meta-analyses on included in these cohorts.
this patient population were pub- If multiple studies were published Statistical Methods
lished more than 10 years ago and in- from the same cohort of subjects at dif- This meta-analysis was performed us-
vestigated neurodevelopmental out- ferent ages, only the last published re- ing STATA statistical software (Version
comes in preschool children.9,10 We port was included (unless the cogni- 7, STATA Corp, College Station, Tex).
report the first meta-analysis on the cog- tive and behavioral data were published For each study, the nonstandardized dif-
nitive and behavioral outcomes of separately, in which case both reports ference between the mean cognitive test
school-aged children who were born were included). Studies were also ex- scores of cases (preterm-born children)
preterm by combining the results from cluded if they reported outcomes on a and controls (term-born children) was
case-control studies published be- defined subgroup of the population (eg, weighted by the inverse of the variance
tween 1980 and November 2001. only cases with intraventricular hem- for this difference. These weighted mean
orrhage) or if the same cognitive test differences (WMDs) were pooled across
METHODS was not used for all subjects. From the studies to compute an overall mean cog-
Selection of Studies 227 studies retrieved and reviewed, only nitive difference between cases and con-
The guidelines published by Stroup et al11 15 studies with cognitive data and 16 trols. Cognitive scores from all studies
for the meta-analysis of observational studies with behavioral data met these were obtained from comparable tests of
studies were followed in the design, per- selection criteria. cognition (normative data from all re-
formance, and reporting of this meta- ported tests had a mean [SD] of 100 [15].
analysis. A MEDLINE search included Data Extraction Therefore, the nonstandardized WMD
the period from 1980 to November 2001 Data were entered into a customized was chosen as the cognitive outcome
and used the subject headings infant- database created for this meta-analysis, measure for combining studies in this
premature; or infant, low birth weight; and with data extracted on the study de- meta-analysis.
cognition; developmental disabilities; child sign, attrition rate, demographic vari- We used random-effects and fixed-
development; personality development; ables, geographic location, socioeco- effects least-square regression models
child development disorders; human devel- nomic status, and detailed information for combining the results in this meta-
opment; behavior; child behavior disor- on the cognitive and behavioral evalu- analysis. The fixed-effects and random-
ders; attention deficit; and disruptive behav- ations performed. Explanatory vari- effects models produced virtually iden-
ior disorders. These search terms were ables were chosen based on their sig- tical results; therefore, only the results
combined with the “explode” feature nificant association with cognitive and obtained from the random-effects mod-
when applicable, the search was limited behavioral outcomes in the published lit- els are presented.
©2002 American Medical Association. All rights reserved. (Reprinted) JAMA, August 14, 2002—Vol 288, No. 6 729
Downloaded from jama.ama-assn.org by guest on June 2, 2011
COGNITION AND BEHAVIOR OF CHILDREN BORN PRETERM
had a 95% CI that included zero (−1.64
Table 1. Quality Criteria for Observational Studies*
to 1.93), thus suggesting no evidence
Score
for a systematic disagreement bias be-
Quality Parameters 2 1 0 tween the 2 reviewers.
Population sample Defined geographic ⱖ1 Hospital Convenience sample
area (1 clinic) RESULTS
Study design Prospective Patients contacted NA Cognition
longitudinal after neonatal
follow-up intensive care unit From these 15 case-control studies, 17
discharge
groups of children (including 1556
Demographic data† NA Complete description Inadequate
cases and 1720 controls) were evalu-
Socioeconomic data‡ NA Adequate Inadequate
ated after their fifth birthday. The de-
Neurological outcomes Complete description Partial description Inadequate
of prematurity§ mographic data from these studies are
Matching of cases and ⬎3 Factors 1-3 Factors None listed in TABLE 2.6,23-36 Three studies
controls contained data from the United States,
*NA indicates data not available. 9 studies looked at regional popula-
†Gestational age at birth, sex, race, or age at evaluation.
‡Family income, insurance status, maternal education, paternal education, or Hollingshead index. tions, and the others followed hospital-
§Neurological deficits, blindness, deafness, cerebral palsy, or hydrocephalus. based cohorts. Sample size of the cases
ranged from 15 to 255 and of the con-
The homogeneity of the WMDs across study was measured by computing trols ranged from 15 to 500. Control
studies was formally tested using the (based on the percentages of ADHD populations in all the studies were
general variance-based method de- children reported in cases and con- matched with the cases on 1 or more
scribed by Greenland.15 Because this test trols) a study-specific relative risk (RR). demographic features. As shown in
is known to have low power, homoge- These RRs were combined to estimate Table 2, information on demographic
neity was further investigated graphi- a pooled RR using the same inverse vari- variables such as sex, race, and socio-
cally using Galbraith plots.16-18 These ance-weighted least-squares method de- economic status was not always re-
plots allow the contribution of each scribed above for the analysis of cog- ported.
study to the overall homogeneity test sta- nitive data. Statistical analyses similar A random-effects meta-analysis
tistic to be examined visually. The Gal- to those described above were also used showed that the WMD between the
braith plot graphs each study’s z score to test for homogeneity of the RR for mean cognitive scores of the cases and
(the mean difference divided by the SE ADHD across studies and to assess for the controls was 10.9 (95% CI, 9.2-
of the difference [d/SE{d}]) vs the re- publication bias. 12.5) in favor of the controls (z=13.14;
ciprocal of the SE of the mean differ- P⬍.001; FIGURE 1). However, the 2 test
ence [1/SE{d}] and fits a least-square re- Assessment of Study Quality for heterogeneity was significant
2
gression line constraining the intersect We performed assessments of study ( 16 =33.65; P=.006). A Galbraith plot
to zero. Studies exhibiting high hetero- quality based on a novel 10-point score to assess study heterogeneity showed
geneity will have a z score that falls out- developed for this meta-analysis. The that the 2 populations32,35 with the high-
side 2 SDs above and below the fitted re- scoring was based on factors thought est WMD were the cause for this het-
gression line. Linear meta-analysis to be good quality indicators for obser- erogeneity. Taylor et al35 showed the
regression models were fitted to ex- vational studies using a case-control de- highest WMD between the cases and
plore the impact of study-specific co- sign; these criteria are described in controls, which is possibly explained by
variates on heterogeneity.15 The poten- TABLE 1. Studies that scored 8 or higher the fact that this study included cog-
tial for publication bias was visually were grouped as high quality, whereas nitive assessment of children with se-
assessed by examining for possible skew- studies scoring less than 8 were grouped vere neurological disability and as-
ness in Begg modified funnel plots.19 For- as low quality for the purpose of sub- signed them the lower limit of IQ scores
mal tests for skewness in the funnel plots group analysis. (39 points) to preserve sample size.
and thus for publication bias were imple- Quality assessment scoring was per- Similarly, Stjernqvist and Svenning-
mented using the weighted-linear re- formed independently by 2 of the au- sen32 also included the IQ scores of chil-
gression approach proposed by Egger et thors (A.T.B. and K.J.S.A) and showed dren with severe disability (IQ score
al.20 The relationships between the mean high concordance between the 2 rat- ⬍70 or 2 SDs below mean). The re-
cognitive score and birth weight and ges- ers as measured by the Lin concor- maining studies, with the exception of
tational age in each study were exam- dance correlation coefficient (Pc=0.79; the study by Teplin et al,27 had ex-
ined independently using inverse– 95% CI, 0.62-0.96).21 Furthermore, us- cluded children who could not be ad-
variance-weighted linear regression. ing the Bland and Altman limits-of- ministered the tests of cognition. Het-
The relationship between preterm agreement procedure,22 the average dis- erogeneity was no longer significant
birth and school-aged ADHD in each agreement was close to zero (0.14) and after excluding the data reported by
730 JAMA, August 14, 2002—Vol 288, No. 6 (Reprinted) ©2002 American Medical Association. All rights reserved.
Downloaded from jama.ama-assn.org by guest on June 2, 2011
COGNITION AND BEHAVIOR OF CHILDREN BORN PRETERM
Table 2. Case-Control Studies With Cognitive Data*
Type of Mean
Male, White, Years Gestational Age at Cognitive Mean (SD) Quality
Source % % of Birth Birth Weight, g† Age, wk‡ Evaluation, y Test Score§ Score
Lloyd et al,23 1988㛳¶
Cases (n = 44) 47 76 1975-1979 ⬍1500 (1302) [850-1500] 321 (26-37) 7 BAS 93 (15) 6
Controls (n = 44) 47 77 1975-1978 NA 40 7 BAS 100.4 (12.9)
Portnoy et al,24 1988㛳¶
Cases (n = 15) 60 66 1980-1981 ⬍1000 (909) NA 5 MIQS 93 (20) 8
Controls (n = 15) 60 66 1980-1981 ⬎2500 38-42 5 MIQS 103 (13)
McDonald et al,25 1989
Cases (n = 16) NA NA NA ⬍2500; 1776 (510) ⬍35; 31.4 (3) 5 WPPSI 113 (21) 5
Controls (n = 18) NA NA NA 3359 (481) 40 5 WPPSI 124 (13)
Smith and Knight-Jones,26
1990
Cases (n = 43) 47 86 1981 1306 (165) [850-1500] ⬎28 5 MIQS 88.6 (13) 7
Controls (n = 43) 47 NA 1981 3342 (430) ⬎37 5 MIQS 101 (13)
Teplin et al,27 1991
Cases (n = 28) 50 46 1980 ⬍1000; 905 (86) 28 (1.5) 6 KABC 86 (13.6) 6.5
Controls (n = 26) NA NA 1980 NA 40 6 KABC 98.7 (14.3)
Sommerfelt et al,6 1993
Cases (n = 29) 62 NA 1981-1982 ⬍1500; 1251 (166) 31 (2.6) 8 WISC-R 93.2 (16) 8.5
Controls (n = 29) 62 NA 1981-1982 3650 (490) 40 8 WISC-R 104.2 (14)
Levy-Shiff et al,28 1994
Cases (n = 90) NA NA NA ⬍1500; 1190 (209) 29 (2.3) 13 WISC-R 105.1 (10.5) 7
Controls (n = 90) NA NA NA ⬎2500; 3225 (334) 39 (1.2) 13 WISC-R 114.4 (9.8)
Hall et al,29 1995㛳
Cases (n = 255) NA NA 1984 1000-1499 NA 8 BAS 93.7 (13.6) 6.5
Cases (n = 44) NA NA 1984 ⬍1000 NA 8 BAS 90.4 (11.1)
Controls (n = 500) NA NA 1984 NA 40 8 BAS 101.1 (12.4)
Controls (n = 90) NA NA 1984 NA 40 8 BAS 102.5 (12.4)
Sommerfelt et al,30 1995
Cases (n = 144) 51 NA 1986-1988 ⬍2000; 1555 (368) 32 (3) 5 WPPSI-R 97 (14) 8.5
Controls (n = 163) 55 NA 1986-1988 ⬎3000 40 5 WPPSI-R 104 (14)
Botting et al,31 1998
Cases (n = 138) NA NA 1980-1983 ⬍1500 NA 12 WISC-III 89.7 (17.2) 5.5
Controls (n = 163) NA NA 1980-1983 ⬎2500 40 12 WISC-III 97.8 (17.4)
Stjernqvist and
Svenningsen,32 1999
Cases (n = 61) 41 NA 1985-1986 500-1480; 1042 (242) 27.1 (1.03) 10.5 WISC-III-R 89.8 (15.1) 8
Controls (n = 61) 43 NA 1985-1986 3648 (533) 40.1 (1.43) 10.6 WISC-III-R 106.5 (15.1)
Wolke and Meyer,33 1999
Cases (n = 264) 56 NA 1985-1986 1288 ⬍32 (29.5) 6 KABC 84.8 (95% CI, 8.5
82.7-99.7)
Controls (n = 264) 56 NA 1985-1986 3407 39.6 6 KABC 98.4-101.1
Saigal et al,34 2000§㛳
Cases (n = 150) 47 NA 1977-1982 500-1000; 833 (126) 27 (2.4) 14 WISC-R 89 (19) 9.5
Controls (n = 124) 44 NA 1977-1982 3395 (483) 40 14 WISC-R 102 (13)
Taylor et al,35 2000㛳
Cases (n = 60) 32 55 1982-1986 500-1000; 665.6 (68) 25.7 (1.8) 11 KABC 83.5 (19.7) 8.5
Cases (n = 55) 31 51 1982-1986 1001-1500; 1173.2 (217) 29.4 (2.4) 11 KABC 96.8 (14.4)
Controls (n = 49) 33 59 1982-1986 3300 (660) 40 11 KABC 106.2 (14.3)
Rickards et al,36 2001
Cases (n = 120) 54 NA 1980-1982 1167 (215) 29.3 (2) 14 WISC-III 96.2 (15.5) 7
Controls (n = 41) 61 NA 1980-1982 3417 (432) 39.9 (1) 14 WISC-III 105 (13.3)
*NA indicates data were not reported or not extractable; BAS, British Abilities Scale; MIQS, McCarthy IQ Scale; WPPSI, Wechsler Preschool and Primary Scale of Intelligence;
KABC, Kaufmann Assessment Battery of Childhood; WISC-R, revised Wechsler Intelligence Scale for Children; WPPSI-R, revised Wechsler Preschool and Primary Scale of
Intelligence; WISC-III, third Wechsler Intelligence Scale for Children; and WISC-III-R, revised third Wechsler Intelligence Scale for Children.
†Values are expressed as “mean”; “mean; mean (SD)”; “mean range”; “mean (SD)”; “mean range; mean (SD)”; or “mean (SD) [range].”
‡Values are expressed as “mean”; “range”; “mean (range)”; “mean (SD)”; or “mean; mean (SD).”
§Values are also expressed as “mean (95% confidence interval [CI])”; and “range.”
㛳There was no difference in socioeconomic status. This result was not available for the other studies.
¶Cases and controls were matched for socioeconomic class.
©2002 American Medical Association. All rights reserved. (Reprinted) JAMA, August 14, 2002—Vol 288, No. 6 731
Downloaded from jama.ama-assn.org by guest on June 2, 2011
COGNITION AND BEHAVIOR OF CHILDREN BORN PRETERM
There was a trend toward a greater
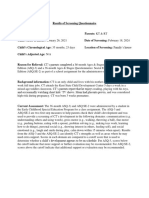
Figure 1. Random-Effects Meta-analysis Comparing Cognitive Test Scores Between Cases
and Controls WMD in the high-quality studies com-
pared with the low-quality studies (11.2
Weighted Mean [95% CI, 9.7-12.7] vs 9.4 [95% CI, 8.0-
Source Difference (95% CI) Favors Cases Favors Controls 10.8]), but this difference was not sta-
Lloyd et al,23 1988 7.40 (1.55 to 13.25)
Portnoy et al,24 1988 10.00 (–2.07 to 22.07)
tistically significant (P=.17).
McDonald et al,25 1989 11.00 (–0.91 to 22.91) We assessed the possibility of pub-
Smith and Knight-Jones,26 1990 12.40 (6.90 to 17.90) lication bias by using a funnel plot to
Teplin et al,27 1991 12.70 (5.24 to 20.16)
Sommerfelt et al,6 1993 11.00 (3.26 to 18.74) assess for skewness. This method sug-
gested no significant publication bias
Levy-Shiff et al,28 1994 9.00 (6.03 to 11.97)
Hall et al,29 1995 (P = .82). Further formal testing was
Study 1 8.80 (5.74 to 11.86) done using the method of Egger et al,20
Study 2 10.70 (7.24 to 14.16)
Sommerfelt et al,30 1995 7.00 (3.86 to 10.14) which also showed a lack of publica-
Botting et al,31 1998 8.10 (4.18 to 12.02) tion bias (R2 =0.30; P=.69).
Stjernqvist and Svenningsen,32 1999 16.70 (11.36 to 22.04)
Wolke and Meyer,33 1999 12.20 (9.80 to 14.60)
Saigal et al,34 2000 13.00 (9.19 to 16.81) Behavior
Taylor et al,35 2000
Study 1 9.40 (3.88 to 14.92)
Sixteen studies provided a compari-
Study 2 22.70 (16.31 to 29.09) son of the incidence of behavioral prob-
Rickards et al,36 2001 8.80 (3.87 to 13.73)
lems between 1759 preterm-born cases
Overall 10.85 (9.23 to 12.47) and 2629 term-born controls. The de-
–30 –20 –10 0 10 20 30 mographic features and behavioral data
Weighted Mean Difference from these studies are summarized in
TABLE 3.6,23,25,27,28,30,32,35-43
The test for heterogeneity was significant (216 =33.65; P=.006). The weighted mean difference significantly
favors controls (z=13.14; P⬍.001). The size of the data marker corresponds to the weight of that study. Error
Children who were born preterm
bars represent 95% confidence intervals. showed increases in externalizing or in-
ternalizing behaviors in 13 (81%) of
these 16 studies. Ten (67%) of 15 stud-
Figure 2. Correlations Between Mean Cognitive Scores, Birth Weight, and Gestational Age
ies that assessed subjects for ADHD
130 130
found that the cases had a signifi-
Cases cantly higher prevalence of attention
Controls
Mean Cognitive Test Score
Mean Cognitive Test Score
120 120 problems compared with controls.
Similarly, 9 (69%) of 13 studies found
110 110 a significantly higher prevalence of ex-
ternalizing symptoms, while 9 (75%)
100 100
of 12 studies found a significantly
90 90 higher prevalence of internalizing
symptoms in the cases vs the controls.
80 80 Further analysis of the behavioral data
0 1000 2000 3000 4000 25 30 35 40
Mean Birth Weight, g Mean Gestational Age at Birth, wk was not possible due to the variety of
tools used to assess and report these be-
Correlations between each variable (birth weight and gestational age) and mean cognitive test scores were haviors in school-aged children.
significant (birth weight: R2 =0.51; P⬍.001; and gestational age: R2 =0.49; P⬍.001). The preterm-born chil-
dren scored lower on tests of cognition for both variables. Seven populations from 6 studies
were assessed by formally defined cri-
teria (DSM-III, DSM-III-R, or DSM-IV)
Taylor et al35 from this meta-analysis and the WMD between cases and con- to diagnose ADHD in cases and con-
2
( 15 =19.42; P=.20). The pooled WMD trols (R2 = 0.12 [R2 = −0.35]; P = .20). trols. These studies were selected for a
from remaining studies was 10.2 (95% There were no statistical differences be- random-effects meta-analysis to calcu-
CI, 9.0-11.5) in favor of controls tween the cognitive outcomes of US- late the RR of ADHD in children who
(z=16.11; P⬍.001). based populations vs those from other were born preterm (FIGURE 3). Cases
The mean cognitive test scores were countries (10.6 [95% CI, 6.5-14.8] vs had a pooled RR of 2.64 (95% CI, 1.85-
significantly correlated with the birth 10.2 [95% CI, 9.1-11.3]; P=.85) or be- 3.78) compared with controls (z=5.32;
weight (R2 =0.51; P⬍.001) and gesta- tween the studies that compared re- P⬍.001). The test for heterogeneity was
tion at birth (R 2 = 0.49; P⬍.001; gional cohorts with hospital-based not significant between these studies
FIGURE 2). There was no significant cor- populations (10.4 [95% CI, 9.3-11.6] ( 62 =2.60; P=.86). The pooled RR in the
relation between the age at evaluation vs 9.6 [95% CI, 7.3-11.8]; P =.68). cases was similar for the studies la-
732 JAMA, August 14, 2002—Vol 288, No. 6 (Reprinted) ©2002 American Medical Association. All rights reserved.
Downloaded from jama.ama-assn.org by guest on June 2, 2011
COGNITION AND BEHAVIOR OF CHILDREN BORN PRETERM
beled high quality vs low quality (2.5 We limited our search to English- term but were small for their gesta-
[95% CI, 1.4-4.3] vs 2.8 [95% CI, 1.7- language literature because of practical tional age and were not identified in the
4.4]; P=.86). The tests using methods difficulties in abstracting data from ar- description of their cohorts.
by Begg (P=.55) and Egger et al (P=.49) ticles published in other languages. Gre- Data on birth weight and gesta-
showed no significant publication bias. goire et al51 showed that in only 1 of 36 tional age were not always reported as
However, the small number of studies consecutive meta-analyses of random- mean (SD) or range (Table 1). For these
(n=6) makes these tests unreliable. ized clinical trials, the inclusion of non– control groups, we assumed a mean
English-language articles produced re- term gestation of 40 weeks56 and a mean
COMMENT sults different from the published meta- birth weight of 3200 g (50th percen-
Our meta-analysis shows that preterm analysis (with a change in pooled odds tile for age). Cases with severe neuro-
birth is associated with lower cogni- ratio from 0.70 to 0.67). Such compari- logical and cognitive disability were ex-
tive scores and increased risks for ADHD sons have not been published for meta- cluded in all but 3 of the studies
and other behaviors at school age com- analyses of observational studies simi- included in the meta-analysis, al-
pared with term-born controls. Lower lar to ours. Despite the exclusion of non– though the exact definition of severe
cognitive scores for the cases were noted English-language articles, our meta- disability varied between these stud-
in all the studies selected for this meta- analysis contains data from many ies. The studies that included cases with
analysis, and a WMD of greater than 10 countries and no significant differences severe neurological and cognitive dis-
between the cognitive scores of cases occurred in the cognitive outcomes of ability had the highest WMD between
and controls is likely to have signifi- children born preterm in the United the cases and controls (Figure 1).27,32,35
cant educational and social conse- States vs non-US cohorts. For the sake For the purposes of our analysis, we
quences.44 Lower birth weight and ges- of completeness, a repeat MEDLINE assumed that the cognitive scores from
tational age were significantly correlated search found only 4 non–English- the various tests were comparable be-
with decreases in cognitive test scores, language articles (with online abstracts cause of similar normative data for all
highlighting the developmental vul- in English) that were designed as case- the cognitive tests used (mean [SD], 100
nerability of the immature brain. Super- control studies with cognitive and/or be- [15]). Similarly, we assumed that the
imposed on this vulnerability are the havioral data for preterm or term-born different standardized assessments used
factors associated with severity of ill- school-aged children.52-55 Because of the for the diagnosis of ADHD had com-
ness in preterm neonates, their physi- limited information contained in each ab- parable sensitivity and specificity (DSM-
ological instability and exposure to early stract, we cannot say whether these stud- III, DSM-III-R, and DSM-IV). These as-
adverse experiences, which may have ies fulfilled all the inclusion and exclu- sumptions overlook the subtle
a persistent impact on brain develop- sion criteria for this meta-analysis. All 4 differences between the cognitive and
ment leading to these cognitive and of these studies reached conclusions that behavioral tests used, as well as the vari-
behavioral outcomes. are consistent with the results of our ability in administering these tests.
The results of this meta-analysis must meta-analysis. Based on these consider- The stringent application of our se-
be viewed in the light of its limita- ations, we propose that including the re- lection criteria resulted in the exclu-
tions. Multiple studies conducted over sults from non–English-language stud- sion of studies with poor methodo-
the decades have also demonstrated the ies would not have altered our results or logic quality (eg, attrition rate ⬎30%)
significant impact of demographic and conclusions. and poor generalizability (eg, reports of
environmental factors (such as age, sex, Furthermore, the included studies subgroup analyses57). Assessment of
race, and socioeconomic status) on the were published in an era when rapid ad- study quality for meta-analyses of ran-
trajectory of cognitive and behavioral vances were occurring in the field of fe- domized clinical trials has been ques-
development in both preterm39,45-48 and tal medicine and perinatology. There- tioned and may give misleading results
full-term12,49 infants. In a recent study fore, the care provided to these infants in meta-analyses.58 Specific criteria are
of 118 children at age 10 years who was not uniform and must have evolved widely accepted for assessing the qual-
were born preterm, family factors were over the period studied. The selected ity of randomized controlled trials (eg,
stronger predictors of school perfor- studies differed from one another in their randomization, double-blinding, drop-
mance than were perinatal complica- baseline characteristics, such as mean outs, or allocation concealment); how-
tions.50 All the studies included in our birth weight and gestational age. All neo- ever, similar criteria have not been de-
meta-analysis featured cases and con- nates with a gestational age of less than veloped for observational studies. We
trols matched for 1 or more demo- 37 weeks were defined as cases, and the devised a quality assessment tool spe-
graphic variables. Thus, we were un- data obtained from those who were born cifically for this meta-analysis, using the
able to determine the specific impact of full-term but were small for their ges- objective criteria listed in Table 1. The
demographic variables on the mea- tational age were excluded. It is pos- quality of the studies included in this
sured cognitive and behavioral out- sible, however, that some studies may meta-analysis was assessed indepen-
comes. have included those who were born full- dently by 2 of the authors, but showed
©2002 American Medical Association. All rights reserved. (Reprinted) JAMA, August 14, 2002—Vol 288, No. 6 733
Downloaded from jama.ama-assn.org by guest on June 2, 2011
COGNITION AND BEHAVIOR OF CHILDREN BORN PRETERM
Table 3. Case-Control Studies With Behavioral Data*
Years Gestational Mean Age at
Source Male, % White, % of Birth Birth Weight, g† Age, wk‡ Evaluation, y
Lloyd et al,23 1988
Cases (n = 44) 47 76 1975-1979 ⬍1500 (1302 [850-1500]) 32.1 (26-37) 7.2
Controls (n = 44) 47 77 1975-1978 NA 40 7
McDonald et al,25 1989
Cases (n = 16) NA NA NA ⬍2500; 1776 (510) ⬍35; 31.4 (3) 5
Controls (n = 18) NA NA NA 3359 (481) 40 5
Szatmari et al,37 1990
Cases (n = 82) 45 NA 1980-1982 500-1000; 835 (125) 27.4 (2.7) 5
Controls (n = 208) 51 NA 1980-1982 ⬎2500 40 5
Teplin et al,27 1991
Cases (n = 28) 50 46 1980 ⬍1000; 905 (86) 28 (1.5) 6
Controls (n = 26) NA NA 1980 NA ⬎37 6
Ross et al,38 1991
Cases (n = 88) 52 51 1978-1980 ⬍1500; 1192 (200) 29.3 (1.8) 7.5
Controls (n = 80) 51 50 1978-1980 NA 40 7.5
Hack et al,39 1992
Cases (n = 249) 50 44 1977-1979 ⬍1500; 1176.5 29.7 8
Controls (n = 363) NA 38 1977-1979 ⬎2500 40 8
Sommerfelt et al,6 1993
Cases (n = 29) 62 NA 1981-1982 ⬍1500; 1251 (166) 31 (2.6) 8
Controls (n = 29) 62 NA 1981-1982 3650 (490) 40 8
Levy-Shiff et al,28 1994
Cases (n = 90) NA NA NA ⬍1500; 1190 (209) 29 (2.3) 13
Controls (n = 90) NA NA NA ⬎2500; 3225 (334) 39 (1.2) 13
Sommerfelt et al,30 1995
Cases (n = 144) 51 NA 1986-1988 ⬍2000; 1555 (368) 32 (3) 5
Controls (n = 163) 51 NA 1986-1988 ⬎3000 ⬎37 5
Botting et al,40 1997
Cases (n = 138) NA NA 1980-1983 ⬍1500 NA 12
Controls (n = 148) NA NA 1980-1983 ⬎2500 40 12
Whitfield et al,41 1997
Cases (n = 90) NA 87 1974-1985 500-800; 730 (520-800) 26 (23-38) 8
Controls (n = 50) NA 64 1974-1985 3487.6 (2614-4706) 40 (38-42) 9
Horwood et al,42 1998
Cases (n = 77) 48 67 1986 ⬍1000; 823 (114) 27.1 (1.9) 7.5
Cases (n = 221) 48 67 1986 1000-1499; 1267 (147) 30 (2.2) 7.5
Controls (n = 1092) 51 86 1986 3360 (534) 39.6 (1.6) 8
Stevenson et al,43 1999
Cases (n = 167) NA NA 1980-1981 ⬍1500; 1259 (630-1500) 30.8 (26-37) 14
Controls (n = 167) NA NA 1980-1981 3352 (2098-4450) 40 14
Stjernqvist and Svenningsen,32 1999
Cases (n = 61) 41 NA 1985-1986 500-1480; 1042 (242) 27.1 (1.03) 10.5
Controls (n = 61) 43 NA 1985-1986 3648 (533) 40.1 (1.43) 10.6
Taylor et al,35 2000
Cases (n = 60) 32 55 1982-1986 500-1000; 665.6 (68) 25.7 (1.8) 11
Cases (n = 55) 31 51 1982-1986 1001-1500; ⬎1173.2 29.4 (2.4) 11
Controls (n = 49) 33 59 1982-1986 3300 (660) 40 11
Rickards et al,36 2001
Cases (n = 120) 54 NA 1980-1982 1167 (215) 29.3 (2) 14
Controls (n = 41) 61 NA 1980-1982 3417 (432) 39.9 (1) 14
*ADHD indicates attention-deficit/hyperactivity disorder; NA, data were not reported or not extractable; CBCL, Childhood Behavior Check List; DSM, Diagnostic and Statistical
Manual of Mental Disorders; DSM-IV, Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition; ANSER, Aggregate Neurobehavioral Student Health and Educational
Review; PIC, Personality Inventory of Childhood; and CAPA, Child and Adolescent Psychiatric Assessment.
†Values are expressed as “mean (SD [range])”; “mean; mean (SD)”; “mean (SD)”; “mean range; mean (SD)”; “mean”; “mean; mean”; “range; mean (range)”; or “range; mean (SD).”
‡Values are expressed as “mean (range)”; “mean”; “mean; mean (SD)”; or “mean (SD).”
§Refers to total problem score including both externalizing and internalizing behaviors.
㛳Refers to male subjects only.
734 JAMA, August 14, 2002—Vol 288, No. 6 (Reprinted) ©2002 American Medical Association. All rights reserved.
Downloaded from jama.ama-assn.org by guest on June 2, 2011
COGNITION AND BEHAVIOR OF CHILDREN BORN PRETERM
no differences in cognitive or behav-
ioral outcomes between high-quality and
Type of Behavior Mean
Type of Attention/ Quality low-quality studies.
Diagnostic Tool ADHD, % Externalizing Internalizing Hyperactivity Score This meta-analysis provides evi-
dence from a large number of subjects
Rutter NA Yes NA NA 6
that children who were born preterm
Rutter NA
are at significant risk for reduced cog-
CBCL NA No No No 5
nitive performance at school age and
CBCL NA
that gestational age and birth weight are
directly proportional to their mean cog-
DSM 15.9 No No Yes 5.5 nitive test scores. These robust differ-
DSM 6.9 ences should eliminate controversies
generated from the variable cognitive
ANSER and Connors NA NA NA No 6.5 outcomes reported by individual fol-
ANSER and Connors NA low-up studies. Is a mean difference of
10.9 points between the cognitive scores
DSM 18 NA NA Yes 8.5
of school-aged cases and controls clini-
DSM 7.5
cally significant? McCarton et al 44
CBCL NA Yes§ Yes§ Yes 7.5
argued that a 4-point difference between
CBCL NA
cognitive scores may not produce func-
tionally detectable differences between
PIC NA Yes㛳 Yes㛳 No 8.5 children, but on a group basis these dif-
PIC NA ferences will significantly alter the pro-
portion of children classified as “intel-
Connors NA NA NA Yes 7 lectually deficient and of borderline
Connors NA intelligence.” Children who were born
preterm or at LBW are 50% more likely
PIC NA Yes Yes Yes 8.5
to be enrolled in special education
PIC NA
classes compared with term-born chil-
CAPA 23 Yes Yes Yes 5.5
dren, which was conservatively esti-
CAPA 6
mated in 1988 to result in an incre-
mental cost of $370.8 million.59 Based
PIC and Stanford Binet NA No Yes No 10 on such projections, we propose that
PIC and Stanford Binet NA the cognitive differences reported in this
meta-analysis will have a significant
Rutter and Connors NA Yes Yes Yes 6.5 impact on the educational require-
Rutter and Connors NA Yes Yes Yes ments for children who were born pre-
Rutter and Connors NA term and may determine their future
socioeconomic potential.
Rutter 5 Yes Yes Yes 7
The perinatal course of these chil-
Rutter 2
dren may shed some light on the mecha-
CBCL and DSM-IV for ADHD 20 Yes Yes Yes 8
nisms underlying these differences. Pre-
CBCL and DSM-IV for ADHD 8
term neonates are at higher risk for
postnatal complications, such as intra-
CBCL and DuPaul 17 Yes§ Yes§ Yes 8.5 ventricular hemorrhage, sepsis, meta-
CBCL and DuPaul 6 Yes§ Yes§ bolic complications (eg, hypoglyce-
CBCL and DuPaul 4 mia), and chronic lung disease. They are
subjected to multiple painful proce-
CBCL and Connors NA No No No 7 dures and maternal separation for pro-
CBCL and Connors NA longed periods. Experimental evidence
from animal models shows that all these
factors can promote or precipitate neu-
ronal cell death in the immature brain.60
Increased rates of neuronal cell death
could lead to volumetric losses in spe-
©2002 American Medical Association. All rights reserved. (Reprinted) JAMA, August 14, 2002—Vol 288, No. 6 735
Downloaded from jama.ama-assn.org by guest on June 2, 2011
COGNITION AND BEHAVIOR OF CHILDREN BORN PRETERM
improved understanding of the under-
Figure 3. Random-Effects Meta-analysis for Studies Assessing Attention-Deficit/Hyperactivity
Disorder lying biological mechanisms, more fo-
cused therapeutic interventions can be
Relative Risk developed to decrease or prevent these
Source (95% CI) Favors Cases Favors Controls
long-term impairments following sur-
Szatmari et al,37 1990 2.36 (1.16-4.79) vival after preterm birth.
Ross et al,38 1991 2.42 (1.00-5.89)
Botting et al,40 1997 3.81 (1.89-7.70) Author Affiliations: Departments of Pediatrics (Drs
Stevenson,43 1999 1.75 (0.52-5.87) Bhutta, Cleves, Casey, Cradock, and Anand), Biosta-
Stjernqvist and Svenningsen,32 1999 2.40 (0.90-6.40) tistics (Dr Cleves), Anesthesiology (Dr Anand), Phar-
Taylor et al,35 2000
macology (Dr Anand), and Neurobiology (Dr Anand)
and Arkansas Center for Birth Defects Research and
Study 1 1.34 (0.23-7.67)
Prevention (Dr Cleves), University of Arkansas for
Study 2 4.08 (0.94-17.77)
Medical Sciences, Little Rock.
Author Contributions: Study concept and design:
Overall 2.64 (1.85-3.78)
Bhutta, Anand.
0.1 0.2 0.5 1.0 2 5 10 20 Acquisition of data: Bhutta, Anand.
Relative Risk
Analysis and interpretation of data: Bhutta, Cleves,
Casey, Cradock, Anand.
Drafting of the manuscript: Bhutta, Cleves, Casey,
Diagnostic criteria used were based on the Diagnostic and Statistical Manual of Mental Disorders, Third Edi- Anand.
tion; Diagnostic and Statistical Manual of Mental Disorders, Revised Third Edition; or Diagnostic and Statis- Critical revision of the manuscript for important in-
tical Manual of Mental Disorders, Fourth Edition. An increased relative risk existed among cases for attention- tellectual content: Bhutta, Cleves, Casey, Cradock,
deficit/hyperactivity disorder (z=5.32; P⬍.001). The test for heterogeneity was not significant ( 62 = 2.60; P=.86). Anand.
CI indicates confidence interval, illustrated by the error bars. The size of the data marker corresponds to the Statistical expertise: Cleves.
weight of that study. Obtained funding: Anand.
Administrative, technical, or material support: Bhutta,
Anand.
Study supervision: Anand.
Funding/Support: Dr Anand received grant
cific brain regions and may at least par- preterm-born children,40,64 which may HD36484-02 from the National Institute for Child
tially explain the cognitive and behav- contribute to increased parenting stress Health and Human Development and grant 01-199
ioral abnormalities noted in these and maternal depression during early from the Blowitz-Ridgeway Foundation.
Acknowledgment: We gratefully acknowledge the
children. Volumetric measurements of childhood.65,66 help of Tracy L. Thurman, BS, for constructing the da-
brain regions in 8-year-old children born Could the impairment of preatten- tabase used for our study.
preterm showed disproportionately tional mechanisms (such as the sen-
smaller volumes of the sensorimotor cor- sory gating of paired stimuli67) lead to REFERENCES
tex, other cortical areas, the corpus cal- ADHD, which ultimately manifests as 1. Guyer B, Hoyert DL, Martin JA, Ventura SJ, Mac-
Dorman MF, Strobino DM. Annual summary of vital
losum, amygdala, hippocampus, and poor cognition at school age? Preterm- statistics—1998. Pediatrics. 1999;104:1229-1246.
basal ganglia, which were associated with born infants show differences in their 2. Wood NS, Marlow N, Costeloe K, Gibson AT,
significantly lower cognitive scores threshold for arousal, which supports Wilkinson AR, for the EPICure Study Group. Neuro-
logic and developmental disability after extremely pre-
(mean difference = 23.5) and an in- sustained attention and information en- term birth. N Engl J Med. 2000;343:378-384.
creased incidence of ADHD and other be- coding.68,69 Children who were born 3. Roussounis SH, Hubley PA, Dear PR. Five-year fol-
low-up of very low birthweight infants: neurological
havioral disorders.57 Similarly, an in- preterm have been shown to be less ca- and psychological outcome. Child Care Health Dev.
creased incidence of neurocognitive and pable of the selective attention states re- 1993;19:45-59.
4. Hack M, Taylor HG, Klein N, Eiben R, Schatschneider
behavioral abnormalities were corre- quired for learning.70 Thus, we pro- C, Mercuri-Minich N. School-age outcomes in chil-
lated with magnetic resonance imaging pose a series of testable hypotheses to dren with birth weights under 750 g. N Engl J Med.
abnormalities in the brains of 14-year- examine the pathogenesis of poor cog- 1994;331:753-759.
5. Saigal S, Szatmari P, Rosenbaum P, Campbell D,
old children who were born preterm.61 nition in children born preterm. King S. Cognitive abilities and school performance of
Since developing neurons are more vul- Proposals to test such hypotheses will extremely low birth weight children and matched term
control children at age 8 years: a regional study. Pe-
nerable to cell death during the perina- require the concerted efforts of clini- diatrics. 1991;118:751-760.
tal period,62,63 we propose that the bio- cians and neuroscientists to develop a 6. Sommerfelt K, Ellertsen B, Markestad T. Personality
and behaviour in eight-year-old, non-handicapped chil-
logical and environmental insults complete understanding of the biologi- dren with birth weight under 1500 g. Acta Paediatr.
associated with preterm birth may pro- cal, environmental, and psychosocial 1993;82:723-728.
7. Drillien CM, Thomson AJ, Burgoyne K. Low-
mote some of these anatomical differ- mechanisms responsible for these cog- birthweight children at early school-age: a longitudi-
ences. nitive and behavioral differences. Previ- nal study. Dev Med Child Neurol. 1980;22:26-47.
This meta-analysis further shows that ous research has demonstrated that psy- 8. Hack M, Klein NK, Taylor HG. Long-term devel-
opmental outcomes of low birth weight infants. Fu-
children born preterm have a 2.64- chosocial interventions with preterm ture Child. 1995;5:176-196.
fold risk for developing ADHD and fre- infants and their parents may improve 9. Aylward GP, Pfeiffer SI, Wright A, Verhulst SJ. Out-
come studies of low birth weight infants published in
quently manifest externalizing or in- cognitive and behavioral outcomes,44,71 the last decade: a meta-analysis. Pediatrics. 1989;
ternalizing behaviors during school age. whereas others report that socioeco- 115:515-520.
10. Escobar GJ, Littenberg B, Petitti DB. Outcome
Multiple studies report an increased nomic factors have minimal effects on among surviving very low birthweight infants: a meta-
prevalence of psychiatric disorders in neurodevelopmental outcomes.4 With an analysis. AJDC. 1991;66:204-211.
736 JAMA, August 14, 2002—Vol 288, No. 6 (Reprinted) ©2002 American Medical Association. All rights reserved.
Downloaded from jama.ama-assn.org by guest on June 2, 2011
COGNITION AND BEHAVIOR OF CHILDREN BORN PRETERM
11. Stroup DF, Berlin JA, Morton SC, et al, for the low-up of children born before 29 gestational weeks: 52. Evers-Embden B, Scholte EM. Leerprestaties en
Meta-analysis Of Observational Studies in Epidemi- health, cognitive development, behaviour and school neurologische status praesens van prematuren, pre-
ology (MOOSE) group. Meta-analysis of observa- achievement. Acta Paediatr. 1999;88:557-562. matue-dysmaturen en dysmaturen op 8-jarige leeftijd.
tional studies in epidemiology: a proposal for report- 33. Wolke D, Meyer R. Cognitive status, language at- Tijdschr Kindergeneeskunde. 1983;51:85-94.
ing. JAMA. 2000;283:2008-2012. tainment, and prereading skills of 6-year-old very pre- 53. Lubetzky O, Weitzman A, Gilat I, Tyano S. Pre-
12. Aylward GP. The relationship between environ- term children and their peers: the Bavarian Longitu- mature birth and cognitive functioning in adoles-
mental risk and developmental outcome. J Dev Be- dinal Study. Dev Med Child Neurol. 1999;41:94- cence [in Hebrew]. Harefuah. 1999;137:380-383.
hav Pediatr. 1992;13:222-229. 109. 54. Finnstrom O, Leijon I, Samuelsson S, et al. Skols-
13. Ornstein M, Ohlsson A, Edmonds J, Asztalos E. 34. Saigal S, Hoult LA, Streiner DL, Stoskopf BL, Rosen- varigheter vanliga hos barn med mycket lag fodelse-
Neonatal follow-up of very low birthweight/ baum PL. School difficulties at adolescence in a re- vikt: extra uppmarksamhet och stod behovs vid skol-
extremely low birthweight infants to school age: a criti- gional cohort of children who were extremely low birth start. Lakartidningen. 2000;97:3492-3495.
cal overview. Acta Paediatr. 1991;80:741-748. weight. Pediatrics. 2000;105:325-331. 55. Burguet A, Monnet E, Roth P, et al. Neurodevel-
14. Verloove-Vanhorick SP, Veen S, Ens-Dokkum MH, 35. Taylor HG, Klein N, Minich NM, Hack M. Middle- opmental outcome of premature infants born at less
Schreuder AM, Brand R, Ruys JH. Sex difference in dis- school-age outcomes in children with very low birth- than 33 weeks of gestational age and not cerebral palsy
ability and handicap at five years of age in children born weight. Child Dev. 2000;71:1495-1511. at the age of 5 years [in French]. Arch Pediatr. 2000;
at very short gestation. Pediatrics. 1994;93:576-579. 36. Rickards AL, Kelly EA, Doyle LW, Callanan C. Cog- 7:357-368.
15. Greenland S. Meta-analysis. In: Rothman K, Green- nition, academic progress, behavior and self-concept 56. Avery M, Richardson D. History and epidemiol-
land S, eds. Modern Epidemiology. 2nd ed. Philadel- at 14 years of very low birth weight children. J Dev ogy. In: Taeusch H, Ballard R, eds. Avery’s Diseases
phia, Pa: Lippincott-Raven; 1998:643-673. Behav Pediatr. 2001;22:11-18. of the Newborn. 7th ed. Philadelphia, Pa: WB Saun-
16. Laird NM, Mosteller F. Some statistical methods 37. Szatmari P, Saigal S, Rosenbaum P, Campbell D, ders; 1998:1-12.
for combining experimental results. Int J Technol As- King S. Psychiatric disorders at five years among chil- 57. Peterson BS, Vohr B, Staib LH, et al. Regional brain
sess Health Care. 1990;6:5-30. dren with birthweights less than 1000 g: a regional per- volume abnormalities and long-term cognitive out-
17. Galbraith RF. A note on graphical presentation of spective. Dev Med Child Neurol. 1990;32:954-962. come in preterm infants. JAMA. 2000;284:1939-
estimated odds ratios from several clinical trials. Stat 38. Ross G, Lipper EG, Auld PA. Educational status 1947.
Med. 1988;7:889-894. and school-related abilities of very low birth weight 58. Juni P. The hazards of scoring the quality of clini-
18. Thompson SG, Sharp SJ. Explaining heterogene- premature children. Pediatrics. 1991;88:1125-1134. cal trials for meta-analysis. JAMA. 1999;282:1054-
ity in meta-analysis: a comparison of methods. Stat 39. Hack M, Breslau N, Aram D, Weissman B, Klein 1060.
Med. 1999;18:2693-2708. N, Borawski-Clark E. The effect of very low birth weight 59. Chaikind S, Corman H. The impact of low birth-
19. Begg CB, Mazumdar M. Operating characteris- and social risk on neurocognitive abilities at school age. weight on special education costs. J Health Econ. 1991;
tics of a rank correlation test for publication bias. Bio- J Dev Behav Pediatr. 1992;13:412-420. 10:291-311.
metrics. 1994;50:1088-1101. 40. Botting N, Powls A, Cooke RW, Marlow N. Atten- 60. Bhutta AT, Anand KJS. Abnormal cognition and
20. Egger M, Davey Smith G, Schneider M, Minder tion deficit hyperactivity disorders and other psychiat- behavior in preterm neonates linked to smaller brain
C. Bias in meta-analysis detected by a simple, graphi- ric outcomes in very low birthweight children at 12 years. volumes. Trends Neurosci. 2001;24:129-132.
cal test. BMJ. 1997;315:629-634. J Child Psychol Psychiatry. 1997;38:931-941. 61. Stewart AL, Rifkin L, Amess PN, et al. Brain struc-
21. Lin LI. A concordance correlation coefficient to 41. Whitfield MF, Grunau RV, Holsti L. Extremely pre- ture and neurocognitive and behavioural function in
evaluate reproducibility. Biometrics. 1989;45:255- mature (⬍ or=800 g) schoolchildren: multiple areas adolescents who were born very preterm. Lancet. 1999;
268. of hidden disability. Arch Dis Child Fetal Neonatal Ed. 353:1653-1657.
22. Bland JM, Altman DG. Statistical methods for as- 1997;77:F85-F90. 62. Rabinowicz T, de Courten-Myers GM, Petetot JM,
sessing agreement between two methods of clinical 42. Horwood LJ, Mogridge N, Darlow BA. Cogni- Xi G, de los Reyes E. Human cortex development: es-
measurement. Lancet. 1986;1:307-310. tive, educational, and behavioural outcomes at 7 to timates of neuronal numbers indicate major loss late
23. Lloyd BW, Wheldall K, Perks D. Controlled study 8 years in a national very low birthweight cohort. Arch during gestation. J Neuropathol Exp Neurol. 1996;
of intelligence and school performance of very low- Dis Child Fetal Neonatal Ed. 1998;79:F12-F20. 55:320-328.
birthweight children from a defined geographical area. 43. Stevenson CJ, Blackburn P, Pharoah PO. Longi- 63. Mitani A, Watanabe M, Kataoka K. Functional
Dev Med Child Neurol. 1988;30:36-42. tudinal study of behaviour disorders in low birth- change of NMDA receptors related to enhancement
24. Portnoy S, Callias M, Wolke D, Gamsu H. Five- weight infants. Arch Dis Child Fetal Neonatal Ed. 1999; of susceptibility to neurotoxicity in the developing pon-
year follow-up study of extremely low-birthweight in- 81:F5-F9. tine nucleus. J Neurosci. 1998;18:7941-7952.
fants. Dev Med Child Neurol. 1988;30:590-598. 44. McCarton CM, Brooks-Gunn J, Wallace IF, et al. 64. Breslau N, Chilcoat HD, Johnson EO, Andreski P,
25. McDonald MA, Sigman M, Ungerer JA. Intelli- Results at age 8 years of early intervention for low- Lucia VC. Neurologic soft signs and low birthweight:
gence and behavior problems in 5-year-olds in rela- birth-weight premature infants: the Infant Health and their association and neuropsychiatric implications. Biol
tion to representational abilities in the second year of Development Program. JAMA. 1997;277:126-132. Psychiatry. 2000;47:71-79.
life. J Dev Behav Pediatr. 1989;10:86-91. 45. Escalona SK. Babies at double hazard: early de- 65. Singer LT, Salvator A, Guo S, Collin M, Lilien L,
26. Smith AE, Knight-Jones EB. The abilities of very velopment of infants at biologic and social risk. Pedi- Baley J. Maternal psychological distress and parent-
low-birthweight children and their classroom con- atrics. 1982;70:670-676. ing stress after the birth of a very low-birth-weight
trols. Dev Med Child Neurol. 1990;32:590-601. 46. Klebanov PK, Brooks-Gunn J, McCormick MC. infant. JAMA. 1999;281:799-805.
27. Teplin SW, Burchinal M, Johnson-Martin N, Classroom behavior of very low birth weight elemen- 66. Robson AL. Low birth weight and parenting stress
Humphry RA, Kraybill EN. Neurodevelopmental, health, tary school children. Pediatrics. 1994;94:700-708. during early childhood. J Pediatr Psychol. 1997;22:
and growth status at age 6 years of children with birth 47. Grantham-McGregor SM, Lira PI, Ashworth A, 297-311.
weights less than 1001 grams. Pediatrics. 1991;118: Morris SS, Assuncao AM. The development of low birth 67. Rasco L, Skinner RD, Garcia-Rill E. Effect of age
768-777. weight term infants and the effects of the environ- on sensory gating of the sleep state-dependent P1/
28. Levy-Shiff R, Einat G, Mogilner MB, Lerman M, ment in northeast Brazil. Pediatrics. 1998;132:661- P50 midlatency auditory evoked potential. Sleep Res
Krikler R. Biological and environmental correlates of de- 666. Online [serial online]. 2000;3:97-105.
velopmental outcome of prematurely born infants in 48. Resnick MB, Gueorguieva RV, Carter RL, et al. The 68. Gardner JM, Karmel BZ. Attention and arousal in
early adolescence. J Pediatr Psychol. 1994;19:63-78. impact of low birth weight, perinatal conditions, and so- preterm and full-term neonates. In: Field T, Sostek A,
29. Hall A, McLeod A, Counsell C, Thomson L, Mutch ciodemographic factors on educational outcome in kin- eds. Infants Born at Risk: Physiological, Perceptual and
L. School attainment, cognitive ability and motor func- dergarten [serial online]. Pediatrics. 1999;104:e74. Cognitive Processes. New York, NY: Grune & Strat-
tion in a total Scottish very-low-birthweight popula- 49. Sameroff AJ, Seifer R, Barocas R, Zax M, Greenspan ton; 1983:69-98.
tion at eight years: a controlled study. Dev Med Child S. Intelligence quotient scores of 4-year-old children: 69. Gladman G, Chiswick ML. Skin conductance and
Neurol. 1995;37:1037-1050. social-environmental risk factors. Pediatrics. 1987;79: arousal in the newborn. AJDC. 1990;65:1063-1066.
30. Sommerfelt K, Ellertsen B, Markestad T. Parental 343-350. 70. Langkamp DL, Brazy JE. Risk for later school prob-
factors in cognitive outcome of non-handicapped low 50. Gross SJ, Mettelman BB, Dye TD, Slagle TA. Im- lems in preterm children who do not cooperate for pre-
birthweight infants. Arch Dis Child Fetal Neonatal Ed. pact of family structure and stability on academic out- school developmental testing. Pediatrics. 1999;135:
1995;73:F135-F142. come in preterm children at 10 years of age. Pediat- 756-760.
31. Botting N, Powls A, Cooke RW, Marlow N. Cog- rics. 2001;138:169-175. 71. Brooks-Gunn J, McCarton CM, Casey PH, et al.
nitive and educational outcome of very-low- 51. Gregoire G, Derderian F, Le Lorier J. Selecting the Early intervention in low-birth-weight premature in-
birthweight children in early adolescence. Dev Med language of the publications included in a meta- fants: results through age 5 years from the Infant Health
Child Neurol. 1998;40:652-660. analysis: is there a Tower of Babel bias? J Clin Epide- and Development Program. JAMA. 1994;272:1257-
32. Stjernqvist K, Svenningsen NW. Ten-year fol- miol. 1995;48:159-163. 1262.
©2002 American Medical Association. All rights reserved. (Reprinted) JAMA, August 14, 2002—Vol 288, No. 6 737
Downloaded from jama.ama-assn.org by guest on June 2, 2011
You might also like
- Salaam BombayDocument5 pagesSalaam BombayArun DhitalNo ratings yet
- 2021 - Prediction of School-Age IQ, Academic Achievement, and Motor Skills in Children With Positional PlagiocephalyDocument6 pages2021 - Prediction of School-Age IQ, Academic Achievement, and Motor Skills in Children With Positional PlagiocephalyStanley YuNo ratings yet
- Brown (2001)Document13 pagesBrown (2001)Eunice_Pinto_1725No ratings yet
- Behavior Problems in Children of Parents With Anxiety DisordersDocument6 pagesBehavior Problems in Children of Parents With Anxiety DisordersRaquel de Azevedo de SouzaNo ratings yet
- Developmental Assessment in Children at Higher Likelihood For Developmental Delays - Comparison of Parent Report and Direct AssessmentDocument11 pagesDevelopmental Assessment in Children at Higher Likelihood For Developmental Delays - Comparison of Parent Report and Direct Assessmentbambinos.fisioterapiaNo ratings yet
- Use of Mobile Technology To Calm Upset Children: Associations With Social-Emotional DevelopmentDocument3 pagesUse of Mobile Technology To Calm Upset Children: Associations With Social-Emotional DevelopmentTowhid HasanNo ratings yet
- Insecure Attachment in Severely Asthmatic Preschool ChildrenDocument5 pagesInsecure Attachment in Severely Asthmatic Preschool ChildrenMatt Van VelsenNo ratings yet
- ESDMDocument9 pagesESDMVictória NamurNo ratings yet
- Four Year Prospective Study of BMI and Mental Health Problems in Young Children SawyerDocument10 pagesFour Year Prospective Study of BMI and Mental Health Problems in Young Children SawyerdidiNo ratings yet
- Peds 2009-2789 FullDocument12 pagesPeds 2009-2789 FullAunNo ratings yet
- ASD Recovery 2019Document5 pagesASD Recovery 2019verdantlaw100% (1)
- Trends in The Prevalence of Developmental Disabilities in US Children, 1997-2008Document11 pagesTrends in The Prevalence of Developmental Disabilities in US Children, 1997-2008Santiago Guarin RuedaNo ratings yet
- ESDMDocument9 pagesESDMAziz Karno KurniawanNo ratings yet
- Chen 2013Document8 pagesChen 2013RominaNo ratings yet
- Danckaerts2000 Article ANaturalHistoryOfHyperactivityDocument13 pagesDanckaerts2000 Article ANaturalHistoryOfHyperactivitymaksim6098No ratings yet
- Tratamiento temprano TEADocument14 pagesTratamiento temprano TEAaurora.ibizaNo ratings yet
- Agudelo 2016Document15 pagesAgudelo 2016rizmahNo ratings yet
- Zhou 2020Document5 pagesZhou 2020Daniel Ignacio Pérez ÁlvarezNo ratings yet
- Clinical Usefulness of Observational Assessment in The Diagnosis of DBD and ADHDDocument14 pagesClinical Usefulness of Observational Assessment in The Diagnosis of DBD and ADHDastrogliaNo ratings yet
- ASQ1Document14 pagesASQ1janakaNo ratings yet
- Nih Mri StudyDocument18 pagesNih Mri StudyJudit ZCNo ratings yet
- Child Neurodevelopmental and Behavioural Problems Are L28zsok4kmDocument8 pagesChild Neurodevelopmental and Behavioural Problems Are L28zsok4kmAgung IqbaalNo ratings yet
- ABAv EclecticDocument31 pagesABAv EclecticIcaro De Almeida VieiraNo ratings yet
- s10803 011 1242 9Document7 pagess10803 011 1242 9MERYEM TNo ratings yet
- Jamapediatrics Cheong 2017 Oi 160101Document7 pagesJamapediatrics Cheong 2017 Oi 160101YsagrimsNo ratings yet
- Brown (2001) PDFDocument13 pagesBrown (2001) PDFAna Catarina InácioNo ratings yet
- 2009 Pediatric Dawson y Rogers ESDMDocument9 pages2009 Pediatric Dawson y Rogers ESDMJu GuaniloNo ratings yet
- She Vell 2003Document15 pagesShe Vell 2003Ivan VeriswanNo ratings yet
- Evaluation of The Child With Global Developmental DelayDocument14 pagesEvaluation of The Child With Global Developmental DelaylauramwoodyardNo ratings yet
- Resilience and Vulnerability in Very Preterm 4-Year-Olds PDFDocument22 pagesResilience and Vulnerability in Very Preterm 4-Year-Olds PDFjuan RamosNo ratings yet
- Emotional and Behavioural Problems Among School Children in PakistanDocument6 pagesEmotional and Behavioural Problems Among School Children in PakistanSagacious MentorNo ratings yet
- APQ EspañolDocument9 pagesAPQ EspañolPaula DuranNo ratings yet
- 2018 - Adhd e VLBWDocument18 pages2018 - Adhd e VLBWdeborahpreitiNo ratings yet
- Impact of Executive Function Deficits and Attention-Deficit/Hyperactivity Disorder (ADHD) On Academic Outcomes in ChildrenDocument10 pagesImpact of Executive Function Deficits and Attention-Deficit/Hyperactivity Disorder (ADHD) On Academic Outcomes in ChildrenEunice_Pinto_1725No ratings yet
- Autism Spectrum Disorders in Extremely Preterm Children OriginalDocument9 pagesAutism Spectrum Disorders in Extremely Preterm Children Originalesteban_falcón_12No ratings yet
- Systematic Review and Meta-Analysis: The Prevalence of Mental Illness in Child and Adolescent Refugees and Asylum SeekersDocument10 pagesSystematic Review and Meta-Analysis: The Prevalence of Mental Illness in Child and Adolescent Refugees and Asylum SeekersdsfsdgfdgfdgNo ratings yet
- Noetzel and R.D. Sheth M. Shevell, S. Ashwal, D. Donley, J. Flint, M. Gingold, D. Hirtz, A. Majnemer, MDocument16 pagesNoetzel and R.D. Sheth M. Shevell, S. Ashwal, D. Donley, J. Flint, M. Gingold, D. Hirtz, A. Majnemer, MjoeunisaNo ratings yet
- 自闭症谱系障碍青少年的健康行为、心理社会因素和学术参与一项潜在类别分析 2022Document11 pages自闭症谱系障碍青少年的健康行为、心理社会因素和学术参与一项潜在类别分析 2022Phan Thiên LýNo ratings yet
- How Common Is Attention-Deficit/hyperactivity Disorder? Towards Resolution of The Controversy: Results From A Population-Based StudyDocument5 pagesHow Common Is Attention-Deficit/hyperactivity Disorder? Towards Resolution of The Controversy: Results From A Population-Based StudyDewi PrasetiaNo ratings yet
- 2013 Marlow - Preterm Birth and Childhood Psychiatric DisordersDocument8 pages2013 Marlow - Preterm Birth and Childhood Psychiatric DisordersdeborahpreitiNo ratings yet
- 2019 Article 1336Document6 pages2019 Article 1336Eduardo LimaNo ratings yet
- Statistical Learning Is Associated With Autism Symptoms and Verbal Abilities in Young Children With AutismDocument12 pagesStatistical Learning Is Associated With Autism Symptoms and Verbal Abilities in Young Children With AutismangieNo ratings yet
- Pudmed 1Document11 pagesPudmed 1Eni PurwantiNo ratings yet
- Brief ReportDocument6 pagesBrief Reportsebastoto778No ratings yet
- 0 Practice Parameter For The Assessment and Treatment of C and A With ASDDocument21 pages0 Practice Parameter For The Assessment and Treatment of C and A With ASDDaniNo ratings yet
- Nivens2023 - ACE + Developmenta DelayDocument6 pagesNivens2023 - ACE + Developmenta DelayKaren CárcamoNo ratings yet
- Kaminski Clausse (2017)Document24 pagesKaminski Clausse (2017)Nuria Moreno RománNo ratings yet
- Artigo para ResumirDocument12 pagesArtigo para ResumirDaniela MarquesNo ratings yet
- NIH Public AccessDocument15 pagesNIH Public AccessSofía SciglianoNo ratings yet
- Clark 2016Document12 pagesClark 2016LORENA MONSERRAT MANCERA - HERNANDEZNo ratings yet
- Kim 2022 Evaluating The Use of Self-Reported Measures in Autistic Individuals in The Context of Psychiatric Assessment A Systematic ReviewDocument21 pagesKim 2022 Evaluating The Use of Self-Reported Measures in Autistic Individuals in The Context of Psychiatric Assessment A Systematic ReviewDayna DamianiNo ratings yet
- Child Psychology Psychiatry - 2022 KazdaDocument9 pagesChild Psychology Psychiatry - 2022 KazdaespacioreconectarNo ratings yet
- Article Psicometria PDFDocument14 pagesArticle Psicometria PDFEstela RecueroNo ratings yet
- As MaDocument10 pagesAs MaOsdatillaEsaPutriNo ratings yet
- Mellon2013 PDFDocument22 pagesMellon2013 PDFSipi SomOfNo ratings yet
- Verhulst et al 1992 6 yearsDocument8 pagesVerhulst et al 1992 6 yearscecilialeung.sssNo ratings yet
- Moffitt2015 PDFDocument11 pagesMoffitt2015 PDFRaul Morales VillegasNo ratings yet
- A National Profile of Childhood Epilepsy and Seizure DisorderDocument11 pagesA National Profile of Childhood Epilepsy and Seizure DisorderYovan FabianNo ratings yet
- A Descriptive Study of Behavioral Problems in Schoolgoing ChildrenDocument5 pagesA Descriptive Study of Behavioral Problems in Schoolgoing ChildrenGirlie Faith Morales BrozasNo ratings yet
- Kelly 2019Document17 pagesKelly 2019Sergio A. Dávila SantanaNo ratings yet
- Diagnosis and Treatment of Children With Autism Spectrum DisordersFrom EverandDiagnosis and Treatment of Children With Autism Spectrum DisordersRating: 5 out of 5 stars5/5 (1)
- Brain-Rules-For-Baby-Posters-Small 2Document7 pagesBrain-Rules-For-Baby-Posters-Small 2Fabricio TessaroloNo ratings yet
- All About GermanyDocument10 pagesAll About GermanyBlessie AgananNo ratings yet
- Designing Streets For KidsDocument216 pagesDesigning Streets For KidsJulia MoraisNo ratings yet
- Plan International Nigeria-VacanciesDocument2 pagesPlan International Nigeria-VacanciesABDULLAHI MUSTAPHANo ratings yet
- Bravekidz 11Document5 pagesBravekidz 11prince ahmadNo ratings yet
- Parent Information Booklet 2017Document20 pagesParent Information Booklet 2017marjat.mmNo ratings yet
- Resolution To OperateDocument2 pagesResolution To OperateJodonah Fontanilla100% (1)
- G11 Q2lo2Document15 pagesG11 Q2lo2Jingle CabusasNo ratings yet
- POFL Unit 1 Status QUO pp.1-37Document38 pagesPOFL Unit 1 Status QUO pp.1-37AruNo ratings yet
- Stress Catcher: Catch Some Great Coping Strategies and Skills For Managing StressDocument2 pagesStress Catcher: Catch Some Great Coping Strategies and Skills For Managing StressBrett FieldsNo ratings yet
- Child-Protection-Case-Management-Training-Manual MalawiDocument148 pagesChild-Protection-Case-Management-Training-Manual MalawiRomeo Mali ChahekaNo ratings yet
- Heaven On Earth ShariffaDocument32 pagesHeaven On Earth ShariffaAmandaCostaNo ratings yet
- Absensi Kegiatan UPT Puskesmas Sentosa BaruDocument40 pagesAbsensi Kegiatan UPT Puskesmas Sentosa BarukalistaNo ratings yet
- Sensory Profile 2 (SP2) : Age Range: Time To AdministerDocument3 pagesSensory Profile 2 (SP2) : Age Range: Time To Administer宗轶烜No ratings yet
- Nihms 921772Document20 pagesNihms 921772Yussika FernandaNo ratings yet
- Group-13-III-reseach CHAPTER 3Document13 pagesGroup-13-III-reseach CHAPTER 3gabriellesevilla40No ratings yet
- Guide QuestionsDocument4 pagesGuide QuestionsMicah YapNo ratings yet
- Beauty Standards and Their Relation To Child DevelopmentDocument14 pagesBeauty Standards and Their Relation To Child Developmentapi-618121022No ratings yet
- Accomplishment Report TemplateDocument11 pagesAccomplishment Report TemplateRhea grace OnganonNo ratings yet
- Chore Chart For KidsDocument16 pagesChore Chart For KidsSara Pimentel100% (3)
- PHIL. VAL. SYSTEM-Emotional Closeness and Security in A FamilyDocument4 pagesPHIL. VAL. SYSTEM-Emotional Closeness and Security in A FamilyRhea Bulaga Lisondra100% (1)
- RBT Lev El Assessment Technique: Performance Standards Learning Competencies Highest Thinking Skill To AssessDocument5 pagesRBT Lev El Assessment Technique: Performance Standards Learning Competencies Highest Thinking Skill To AssessGemma Joy Sugue AlforqueNo ratings yet
- Movement Lesson PlanDocument2 pagesMovement Lesson Planapi-601585033No ratings yet
- FINAL Food Insecurity Letter To Governor Oct 2020Document5 pagesFINAL Food Insecurity Letter To Governor Oct 2020ZacharyEJWilliamsNo ratings yet
- CHILD - Impact of Screen Viewing On Cognitive Development - For Circulation DigitalDocument4 pagesCHILD - Impact of Screen Viewing On Cognitive Development - For Circulation DigitalyunielescazNo ratings yet
- Northwestern Medicine NICU Breast Pump Usage NMHDocument5 pagesNorthwestern Medicine NICU Breast Pump Usage NMHFayrouz EssawiNo ratings yet
- Asq Asqse ReportDocument2 pagesAsq Asqse Reportapi-710021174No ratings yet
- Opinion - Children, Reading Stories Vs Watching TV or Playing Computer GamesDocument2 pagesOpinion - Children, Reading Stories Vs Watching TV or Playing Computer GamesNgọc LinhNo ratings yet
- BKC CertificateDocument1 pageBKC Certificateapi-430954731No ratings yet