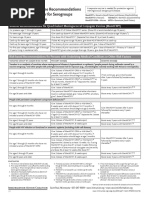
Vaccinations For Age 9 To 99
Vaccinations For Age 9 To 99
Download as pdf or txt
You might also like
- USMLE Step 3 Lecture Notes 2021-2022: Internal Medicine, Psychiatry, EthicsFrom EverandUSMLE Step 3 Lecture Notes 2021-2022: Internal Medicine, Psychiatry, EthicsRating: 5 out of 5 stars5/5 (9)
- Community Health Nursing (Pre-Test) : B. Fertilized Ascaris Lumbricoides OvaDocument2 pagesCommunity Health Nursing (Pre-Test) : B. Fertilized Ascaris Lumbricoides OvaSolsona Natl HS Maananteng100% (2)
- Philippine Childhood Immunization Schedule 2019Document8 pagesPhilippine Childhood Immunization Schedule 2019Linius Cruz67% (3)
- ChlorpromazineDocument2 pagesChlorpromazineevalyn dane50% (2)
- Asplenia ProtocolDocument5 pagesAsplenia ProtocolarjumandNo ratings yet
- Childhood Immunization Schedule 2019Document8 pagesChildhood Immunization Schedule 2019Maribel LutzNo ratings yet
- Immunization ScheduleDocument2 pagesImmunization ScheduleTracy100% (1)
- Expanded Program of ImmunizationDocument20 pagesExpanded Program of ImmunizationgwynNo ratings yet
- Pneumococcal Vaccine Timing For AdultsDocument4 pagesPneumococcal Vaccine Timing For AdultsNur Farhanah Zulkifli100% (1)
- IZSchedule0 6yrsDocument1 pageIZSchedule0 6yrsKaty ForemanNo ratings yet
- VaccinesDocument4 pagesVaccinesSam smithNo ratings yet
- Childhood Immunization 2Document7 pagesChildhood Immunization 2Dexter Carlo GutierrezNo ratings yet
- Splenectomy Updated Dec2019Document4 pagesSplenectomy Updated Dec2019Dessika ListiariniNo ratings yet
- Karla May C. Gentapan, M.D. Post-Graduate Medical Intern DMSFI Department of PediatricsDocument66 pagesKarla May C. Gentapan, M.D. Post-Graduate Medical Intern DMSFI Department of PediatricsCyril James Tagud BualNo ratings yet
- Mening Acwy RecsDocument1 pageMening Acwy Recsnlearn nNo ratings yet
- ImmunizationsDocument64 pagesImmunizationsLily BeltranNo ratings yet
- Published Assessment Report: VarilrixDocument4 pagesPublished Assessment Report: VarilrixkemalahmadNo ratings yet
- Finally Vaccine (Uw + MTB) By: ArakiDocument4 pagesFinally Vaccine (Uw + MTB) By: Arakikoki74No ratings yet
- Immunization in ChildrenDocument28 pagesImmunization in ChildrensaripjunayyahNo ratings yet
- CDC Healthcare Personnel Vaccination RecommendationsDocument1 pageCDC Healthcare Personnel Vaccination RecommendationsdocktpNo ratings yet
- Final - Back 1 PDFDocument2 pagesFinal - Back 1 PDFesbat07No ratings yet
- Childhood Immunizations: Department of PediatricsDocument17 pagesChildhood Immunizations: Department of PediatricsLyrah AlbertoNo ratings yet
- Iap Vaccination RecentDocument7 pagesIap Vaccination RecentDrNavya K UmeshNo ratings yet
- Name of Drug Classification Mechanism of Action Indication Contraindication Side Effects Nursing ResponsibilitiesDocument4 pagesName of Drug Classification Mechanism of Action Indication Contraindication Side Effects Nursing ResponsibilitiesMinaNo ratings yet
- Pneumo Vaccine TimingDocument4 pagesPneumo Vaccine TimingShenouty BNo ratings yet
- Immunisation Schedule Victoria-November 2021Document6 pagesImmunisation Schedule Victoria-November 2021Julie PanditNo ratings yet
- Splenectomy - Factsheet - For - Health - Professionals 2022 FinalDocument4 pagesSplenectomy - Factsheet - For - Health - Professionals 2022 Finalalpha.blocker11No ratings yet
- Vaccine QW5Document2 pagesVaccine QW5hajj2807No ratings yet
- Preventive PediatricsDocument111 pagesPreventive PediatricsPrincess Noreen SavellanoNo ratings yet
- HIC Vaccination Summary - C A R T E LDocument3 pagesHIC Vaccination Summary - C A R T E Lali khaledNo ratings yet
- Preventing and Treating Infections in Children With Asplenia or HypospleniaDocument5 pagesPreventing and Treating Infections in Children With Asplenia or HypospleniaAmélieNo ratings yet
- IMUNISASI2Document29 pagesIMUNISASI2RatnaSuryatiNo ratings yet
- Immunizations in Autoimmune Inflammatory Rheumatic Disease in AdultsDocument6 pagesImmunizations in Autoimmune Inflammatory Rheumatic Disease in Adultsmxg3merNo ratings yet
- Immunization Routine Table1Document11 pagesImmunization Routine Table1javiNo ratings yet
- CHS Recommended VaccinesDocument1 pageCHS Recommended Vaccineslonzell.brantleyNo ratings yet
- Do Patients Who Received Only Two Doses of Hepatitis B Vaccine Need A BoosterDocument3 pagesDo Patients Who Received Only Two Doses of Hepatitis B Vaccine Need A Boostertsiko111No ratings yet
- Altered Immunocompetence: UpdatesDocument27 pagesAltered Immunocompetence: UpdatestrishnaNo ratings yet
- DR Solis - Midterms - Preventive Pediatrics 1&2 & HandoutsDocument12 pagesDR Solis - Midterms - Preventive Pediatrics 1&2 & HandoutschristianNo ratings yet
- Raymund Christopher R. Dela Peña, RN, RM, MAN UNP-College of NursingDocument32 pagesRaymund Christopher R. Dela Peña, RN, RM, MAN UNP-College of NursingrnrmmanphdNo ratings yet
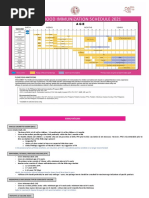
- Childhood Immunization Schedule 2021 EditedDocument11 pagesChildhood Immunization Schedule 2021 EditedPatricia Bernadette PalenciaNo ratings yet
- bexsero-epar-product-information_enDocument38 pagesbexsero-epar-product-information_ensiriteanubiatriceNo ratings yet
- COVID 19 Immunization Schedule Ages 6months OlderDocument6 pagesCOVID 19 Immunization Schedule Ages 6months OlderAlvin EvangelistaNo ratings yet
- 1 CombineDocument726 pages1 CombineSong Hành Vạn KiếpNo ratings yet
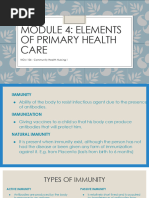
- Module 4 - Elements of Primary Health CareDocument12 pagesModule 4 - Elements of Primary Health CareAllyza Pholette DistorNo ratings yet
- Summary Document For Interim Clinical ConsiderationsDocument2 pagesSummary Document For Interim Clinical Considerationssaurabh pandey0% (1)
- Immunization and VaccinationDocument7 pagesImmunization and VaccinationRoyce GonzagaNo ratings yet
- Pneumococcal VaccineDocument1 pagePneumococcal VaccineSarah :-)No ratings yet
- Pneumococcal Vaccines: Lakshay TyagiDocument30 pagesPneumococcal Vaccines: Lakshay TyagiLakshay TyagiNo ratings yet
- 7-18yr Schedule For Immunizations, CDC 2008Document1 page7-18yr Schedule For Immunizations, CDC 2008Tracy100% (1)
- Childhood Immunization Schedule 2021Document11 pagesChildhood Immunization Schedule 2021Paula QuiñonesNo ratings yet
- Week 4 Peer ResponseDocument3 pagesWeek 4 Peer ResponseMayumi BalmesNo ratings yet
- Adult Immunization Schedule by Vaccine and Age Group - CDCDocument17 pagesAdult Immunization Schedule by Vaccine and Age Group - CDCCamacaro Arevalo JoseNo ratings yet
- Pneumonia VaccinesDocument4 pagesPneumonia Vaccinesapi-237094717No ratings yet
- Vaccine Timing CDCDocument40 pagesVaccine Timing CDCanindita.prasidha.parameswariNo ratings yet
- Ijn 26 7Document8 pagesIjn 26 7Alex WayneNo ratings yet
- Vibriosis Vaccine (Inactivated) For Sea BassDocument2 pagesVibriosis Vaccine (Inactivated) For Sea BassaymenbiogalenicNo ratings yet
- Vaccination SchedDocument9 pagesVaccination SchedDaihachi DaimeNo ratings yet
- Pediatria Integral XIX 9 - WEB PDFDocument98 pagesPediatria Integral XIX 9 - WEB PDFIvan BurgosNo ratings yet
- Artikel 1Document3 pagesArtikel 1Dieni Rhdezscpecjthor UnityNo ratings yet
- The Routine Immunisation ScheduleDocument10 pagesThe Routine Immunisation ScheduleJamesWaitonNo ratings yet
- Table I IAP Immunization Schedule 2016 FinalDocument7 pagesTable I IAP Immunization Schedule 2016 FinalVaishnavi AgrawalNo ratings yet
- A Statistical Inquiry Into the Nature and Treatment of EpilepsyFrom EverandA Statistical Inquiry Into the Nature and Treatment of EpilepsyNo ratings yet
- Blood TransfusionDocument8 pagesBlood TransfusionAlthea AlcalaNo ratings yet
- Neonatal JaundiceDocument5 pagesNeonatal JaundiceIzwan KyNo ratings yet
- Epidemiology and Pathophysiology of Colonic Diverticular DiseaseDocument8 pagesEpidemiology and Pathophysiology of Colonic Diverticular DiseaseAnonymous Hz5w55No ratings yet
- Conversation Between ProfessionsDocument3 pagesConversation Between ProfessionsHeryani AnikNo ratings yet
- Pubic Health SurvilanceDocument28 pagesPubic Health Survilanceteklay100% (2)
- Cardiology - Video - Slides KaplanDocument51 pagesCardiology - Video - Slides KaplanAishwarya RaghuramNo ratings yet
- Drugs Acting On CNSDocument32 pagesDrugs Acting On CNSjustin rodrigoNo ratings yet
- HIVand Texas LawDocument2 pagesHIVand Texas LawForfamNo ratings yet
- Workshop On Early Warning Score System - Ali HaedarDocument61 pagesWorkshop On Early Warning Score System - Ali HaedarGede Kevin Adhitya SaputraNo ratings yet
- Keys Shah - SCI CW Genetics Project Research 114 - 15721804Document3 pagesKeys Shah - SCI CW Genetics Project Research 114 - 15721804keysha31No ratings yet
- Urinary Incontinence in Older Adults.25Document6 pagesUrinary Incontinence in Older Adults.25citraNo ratings yet
- Twinrix Product MonographDocument27 pagesTwinrix Product Monographandy175No ratings yet
- Ebook StrokeDocument195 pagesEbook StrokeLaurenz KilmanunNo ratings yet
- Biofeedback Therapy in Pune - Dr. Rupali Bandgar-JankarDocument3 pagesBiofeedback Therapy in Pune - Dr. Rupali Bandgar-JankardrrupalibandgarNo ratings yet
- Thyroid Disorder: by DR - Wael MetwalyDocument9 pagesThyroid Disorder: by DR - Wael MetwalysardashtiNo ratings yet
- Ramadan Guide For DiabetesDocument9 pagesRamadan Guide For DiabetesUjwal TickooNo ratings yet
- 103057Document49 pages103057ohridiftNo ratings yet
- This Patient Have A Hemorrhagic StrokeDocument7 pagesThis Patient Have A Hemorrhagic StrokeMario ARNo ratings yet
- Berra 2020Document12 pagesBerra 2020Indri AswariNo ratings yet
- 2015 - October - PD Mind and Memory With FlyersDocument53 pages2015 - October - PD Mind and Memory With Flyersapi-280025964No ratings yet
- Cranium 3Document26 pagesCranium 3giant nitaNo ratings yet
- Mind MapsDocument5 pagesMind MapsMaahin IbrahimNo ratings yet
- COVID 19 Ab Fact SheetDocument4 pagesCOVID 19 Ab Fact Sheet10tenharmonyNo ratings yet
- RPP MfaDocument10 pagesRPP MfaIZZAT DANAZZATNo ratings yet
- Case Presentation On Acute Infectious Diarrhea By: Francis B. Aquino Som - IiiDocument10 pagesCase Presentation On Acute Infectious Diarrhea By: Francis B. Aquino Som - IiiCalingalan Hussin CaluangNo ratings yet
- HysterectomyDocument24 pagesHysterectomypt.mahmoudNo ratings yet
- Prescription J d8z c2jjm56sUcPPQmHsPxI216ZuVp2dT3jXJWSBHrFMo69w6N3I92ftygTLEXDocument2 pagesPrescription J d8z c2jjm56sUcPPQmHsPxI216ZuVp2dT3jXJWSBHrFMo69w6N3I92ftygTLEXafreensiddique1771No ratings yet
- List of BacteriaDocument3 pagesList of BacteriaSol T. ParedesNo ratings yet