Azucares y metabolismo
Azucares y metabolismo
Uploaded by
Maria Fernanda Barros AnicharicoCopyright:
Available Formats
Azucares y metabolismo
Azucares y metabolismo
Uploaded by
Maria Fernanda Barros AnicharicoCopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Copyright:
Available Formats
Azucares y metabolismo
Azucares y metabolismo
Uploaded by
Maria Fernanda Barros AnicharicoCopyright:
Available Formats
Proceedings of the Nutrition Society (2019), 78, 246–256 doi:10.
1017/S0029665118002604
© The Authors 2018 First published online 23 October 2018
The Nutrition Society Irish Section Meeting was held at the University of Ulster, Coleraine on 20–22 June 2018
Conference on ‘Targeted approaches to tackling current nutritional issues’
Julie Wallace Medal Lecture
Dietary sugars, exercise and hepatic carbohydrate metabolism
Javier T. Gonzalez* and James A. Betts
Department for Health, University of Bath, Bath BA2 7AY, UK
Proceedings of the Nutrition Society
The present paper reviews the physiological responses of human liver carbohydrate metab-
olism to physical activity and ingestion of dietary sugars. The liver represents a central link
in human carbohydrate metabolism and a mechanistic crux point for the effects of dietary
sugars on athletic performance and metabolic health. As a corollary, knowledge regarding
physiological responses to sugar ingestion has potential application to either improve endur-
ance performance in athletes, or target metabolic diseases in people who are overweight,
obese and/or sedentary. For example, exercise increases whole-body glycogen utilisation,
and the breakdown of liver glycogen to maintain blood glucose concentrations becomes
increasingly important as exercise intensity increases. Accordingly, prolonged exercise at
moderate-to-high exercise intensity results in depletion of liver glycogen stores unless carbo-
hydrate is ingested during exercise. The exercise-induced glycogen deficit can increase insulin
sensitivity and blood glucose control, and may result in less hepatic lipid synthesis.
Therefore, the induction and maintenance of a glycogen deficit with exercise could be a
specific target to improve metabolic health and could be achieved by carbohydrate
(sugar) restriction before, during and/or after exercise. Conversely, for athletes, maintaining
and restoring these glycogen stores is a priority when competing in events requiring repeated
exertion with limited recovery. With this in mind, evidence consistently demonstrates that
fructose-containing sugars accelerate post-exercise liver glycogen repletion and could reduce
recovery time by as much as half that seen with ingestion of glucose (polymers)-only.
Therefore, athletes aiming for rapid recovery in multi-stage events should consider ingesting
fructose-containing sugars to accelerate recovery.
Glucose: Galactose: Fructose: Glycogen: Physical activity
The French physiologist Claude Bernard (1813–1878) is supply to the liver) has little to no glucose, whereas the
not only one of the first to propose blind experiments hepatic vein leaving the liver carries substantial quan-
to reduce bias(1) but also is credited with the discovery tities of glucose. This led Bernard to conclude that the
of glycogen in the liver, thus revealing the central role liver is a potential source of sugar. This capacity of the
of this organ in the homeostatic regulation of blood glu- liver to supply glucose to the systemic circulation is
cose concentrations (or milieu intérieur)(2,3). Bernard important when dietary carbohydrate intake is insuffi-
originally intended to study the metabolism of all types cient to meet the carbohydrate demands of tissues such
of foods, choosing to start with the putatively simple as the brain and muscles. Therefore, during fasting, exer-
metabolism of sugars. The complexities of sugar metab- cise or consumption of low-carbohydrate diets, the liver
olism led Bernard to focus on this area for more than 30 can supply glucose for peripheral tissues. Glucose pro-
years and, in understated fashion, he described this sys- duced by the liver is derived from two sources: the break-
tematic and meticulous undertaking as ‘research which down of stored glycogen (i.e. glycogenolysis), and the de
has not been wholly sterile’(4). During this time, he novo production of new glucose from precursors such as
found that the portal vein of dogs (the major blood lactate, glycerol, pyruvate, glucogenic amino acids,
Abbreviations: P, phosphate; UDP, uridine diphosphate.
*Corresponding author: Javier T. Gonzalez, email J.T.Gonzalez@bath.ac.uk
https://doi.org/10.1017/S0029665118002604 Published online by Cambridge University Press
Sugars and liver metabolism 247
fructose and galactose (i.e. gluconeogenesis)(5). The liver is rarely consumed alone, but rather is usually consumed
is the largest glycogen store in human subjects that can alongside fructose or lactose, or is consumed in polymer
be hydrolysed and release glucose into the circulation (non-sugar) form, such as maltodextrin and starch.
to sustain blood glucose concentrations, and is also the Accordingly, whilst this review will refer to the specific
tissue with the greatest capacity for gluconeogenesis. types of sugars utilised in studies (e.g. glucose only v.
Therefore, the ability for the liver to supply glucose fructose–glucose mixtures), it can be viewed that a non-
from both glycogenolysis and gluconeogenesis has fructose or non-galactose condition (such as glucose or
important consequences for maintaining metabolic con- maltodextrin ingestion) is physiologically representative
trol during exercise, and especially when dietary carbo- of non-sugar intake (i.e. maltodextrin, starch, etc.),
hydrate intake is restricted. whereas fructose–glucose and galactose–glucose co-
The liver also plays a central role in the postprandial ingestion represent the physiological responses to typical
metabolism of carbohydrates. Following intestinal sugar intake.
absorption, the liver is one of the first tissues exposed
to ingested carbohydrate. Whilst the intestine (and kid-
neys) can also metabolise some dietary sugar(6) and Hepatic metabolism of sugars at rest
undertake gluconeogenesis(7), these are quantitatively
less important than hepatic metabolism, at least in Glucose and galactose are primarily absorbed across the
human subjects(8). Various types of sugars are distinctly intestinal lumen via the transport protein sodium-
Proceedings of the Nutrition Society
metabolised by the liver, with potential implications for dependent GLUT2(14), whereas fructose is primarily
human health and performance(9,10). Accordingly, the absorbed via GLUT5(14). Once absorbed, these
aim of this narrative review is to describe the hepatic sugars are then metabolised very differently. Glucose is
metabolism of dietary sugars at rest and during exercise, preferentially metabolised by extra-splanchnic tissues
whilst considering potential implications for human such as skeletal muscle, the brain and cardiac mus-
health and (endurance) exercise performance. cle(15,16), whilst fructose and galactose are primarily
metabolised by the liver and to a lesser extent small
bowel enterocytes and proximal renal tubules(10,17).
Dietary sugars Peripheral tissues such as muscle are therefore only
exposed to relatively small amounts of fructose and
Common sugars in the human diet include the monosac- galactose(18,19).
charides: glucose, fructose and galactose; and the Compared with galactose, the metabolic fate of fructose
disaccharides: sucrose (fructose–glucose), lactose (galact- is relatively well characterised. At rest, the liver rapidly
ose–glucose) and maltose (glucose–glucose)(9). Dietary takes up and metabolises fructose into fructose-1-
sugars can be consumed from a variety of food sources, phosphate (P) via fructokinase (Km for fructose: about
which can influence resultant health effects. The WHO 0·5 mM and Vmax estimated at about 3 mM/min per g
classifies sugars into those which are intrinsic (e.g. human liver)(20–22). Fructose-1-P is then metabolised
incorporated within the structure of intact fruit and vege- into triose-P (C3 substrates) via aldolase B(23). At rest,
tables or lactose/galactose from milk) v. free sugars(11). the majority of fructose-derived triose-P is converted via
Free sugars are defined by the WHO as monosaccharides gluconeogenesis into glucose (about 50 %) and glycogen
and disaccharides added to foods and beverages by the (about 15–25 %), but some of triose-P can be metabolised
manufacturer, cook or consumer, along with sugars into pyruvate, then either oxidised within the liver or con-
naturally present in honey, syrups, fruit juices and fruit verted into lactate (about 25 %), which enters the systemic
juice concentrates. This classification system is useful circulation and can increase blood lactate concentra-
for distinguishing between food sources of sugar that tions(10,24). One other fate of ingested fructose is the con-
are energy dense (i.e. free sugars) and thus may contrib- version into fatty acids via the process known as de novo
ute to weight gain(11,12). However, this classification lipogenesis(25). It has been suggested that lactate is the pri-
system does not specifically distinguish between ingestion mary precursor to hepatic de novo lipogenesis with fruc-
of glucose-containing sugars and fructose- or galactose- tose intake(26), but the proportion of fructose that is
containing sugars in relation to health, nor does it con- ultimately converted into lipid is estimated at <1 % and
sider the physical activity status of the individual. This therefore represents a quantitatively minor pathway of
is interesting considering the fundamental differences in disposal(19). Nevertheless, the effects of ingested fructose
the intestinal absorption and hepatic metabolism of glu- on de novo lipogenesis may still be important for metabolic
cose, fructose and galactose, and how this metabolism is health(27).
altered during exercise(8–10). Quantitative estimates of the metabolic fate of galactose
Before describing the hepatic metabolism of carbohy- in human subjects are scarce. It has been suggested that
drates and sugars, it is important to clarify two points. the primary pathway for human galactose metabolism is
First, the hydrolysis of glucose polymers such as malto- the Leloir pathway, the enzymes of which show highest
dextrin and starch are typically not rate-limiting to intes- activity in the liver(17). This pathway involves four main
tinal absorption(13), and therefore (at least with regard steps: (1) phosphorylation of galactose by galactokinase
to hepatic metabolism) free glucose, maltose, maltodex- (Km for galactose: about 0·9 mM and Vmax estimated at
trin and starch can all be considered physiologically simi- about 1·4 mM/min per g human liver(28,29)) to yield galact-
lar stimuli. Secondly, in typical human diets, free glucose ose-1-P; (2) conversion of galactose-1-P and uridine
https://doi.org/10.1017/S0029665118002604 Published online by Cambridge University Press
248 J. T. Gonzalez and J. A. Betts
diphosphate (UDP) glucose to UDP galactose and for many weeks. However, utilising fat as a fuel has a
glucose-1-P by galactose-1-P uridyltransferase; (3) conver- number of limitations in the context of exercise perform-
sion of UDP-galactose to UDP-glucose by UDP-galact- ance. Fat is a relatively ‘slow’ fuel; the rate of ATP
ose-4-epimerase; and (4) conversion of UDP-glucose resynthesis with fat is at least half that when utilising
and diphosphate to glucose-1-P and uridine triphosphate muscle glycogen(42,43). Fat is also an inefficient fuel on
by UDP-glucose pyrophosphorylase(17). Of note, is an an oxygen basis, requiring about 10 % more oxygen con-
alternative pathway for step 2, known as the Isselbacher sumption for an equivalent energy yield as glucose(44).
pathway, whereby galactose-1-P and uridine triphosphate Consequently, during high-intensity exercise where
are converted to UDP-galactose and diphosphate by rapid ATP resynthesis is required and/or muscle oxygen
the enzymes UDP-galactose pyrophosphorylase and availability could be limiting, there are advantages to
UDP-glucose pyrophosphorylase(17). Some tracer studies oxidising carbohydrates over fats. Finally, recent evi-
have attempted to determine the metabolic fate of oral gal- dence implies that glycogen is more than just a fuel and
actose in human subjects, estimating that during ingestion is an important signalling molecule(45). Low glycogen
of galactose at a rate of 33 µmol/kg per min (about 135 g concentrations in the intramyofibrillar region are asso-
over 360 min), the splanchnic uptake of galactose is satur- ciated with impaired sarcoplasmic reticulum calcium
able at about 15 µmol/kg per min(30,31). At this rate of release rates and excitation contraction coupling(46).
ingestion, it is estimated that about 30–60 % of the ingested Therefore, specific depots of glycogen appear to play
galactose is converted into glucose(30), mostly via the direct important roles in both fuelling and regulating skeletal
Proceedings of the Nutrition Society
conversation of hexose to glucose (about 67 %), with some muscle contractile function, hence achieving high carbo-
converted via the indirect (hexose to C3 substrates to hydrate availability before and during competition is a
glucose) pathway (about 33 %)(31). Ultimately, the meta- goal for athletes competing in almost all endurance
bolic fate of ingested galactose in human subjects therefore sports(47,48).
remains incompletely understood, although it has been Low carbohydrate (glycogen) availability in muscle
speculated that liver glycogen synthesis is a major and liver is strongly associated with fatigue during pro-
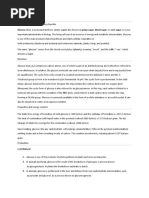
route(32,33) (Fig. 1). longed exercise(49,50). The amount of glycogen stored in
muscle and liver glycogen prior to single, or repeated
bouts of exercise positively correlate with subsequent exer-
Hepatic metabolism of carbohydrates with exercise cise capacity(49,50). A number of carbohydrate-related
adaptations occur in response to regular endurance train-
Exercise increases energy expenditure, which is predomin- ing that facilitate improvements in exercise performance.
antly met during prolonged (>30 min) exercise by increases Endurance-trained athletes have a greater capacity to
in both carbohydrate and fat oxidation compared with store muscle glycogen, and therefore display an increase
the resting state(34). The relative contributions of carbohy- in overnight-fasted muscle glycogen concentrations com-
drate v. fat to exercise metabolism are influenced by the pared with people who are less endurance trained(5,51).
intensity and mode of exercise(35), preceding nutritional This increase in basal muscle glycogen concentrations
status(36–38), endurance training status(39) and biological with endurance training is also exaggerated on a high-
sex(40). Specifically, higher carbohydrate oxidation rates carbohydrate diet(51), suggesting that endurance-trained
are seen with cycling v. running(35), higher v. lower exercise athletes can better tolerate high-carbohydrate diets by
intensity(34), prior carbohydrate feeding v. fasting(37), in appropriately storing the excess carbohydrate as muscle
individuals who are less v. more endurance-trained(39) glycogen. Interestingly, it seems that basal liver glycogen
and amongst men v. women(40). Of these predictive factors, content does not adapt with endurance training, as
the intensity of exercise seems to be the most potent in deter- endurance-trained athletes tend to exhibit similar liver
mining carbohydrate and fat utilisation(34,41). Even in glycogen concentrations to non-trained controls, when
highly trained athletes studied in the overnight fasted measured in the overnight fasted state(5). Whether this is
state, carbohydrates are the predominant fuel source also the case in the postprandial state remains to be
during moderate-to-high intensity (>50 % peak oxygen established.
consumption) exercise(34). Exercise is therefore a potent The increase in fasting muscle (but not liver) glycogen
modulator of carbohydrate metabolism, with implications concentrations with endurance training provides trained
for the fate of ingested carbohydrate. athletes with a larger depot of glycogen to utilise during
The primary sources of carbohydrate supporting exer- exercise and so postpones the point at which critically low
cise metabolism are muscle glycogen, and circulating glu- muscle glycogen concentrations initiate fatigue. In addition
cose and lactate(34). In the fasted state, almost all the to the greater storage capacity, trained athletes also utilise
circulating glucose is derived from hepatic glycogenolysis their muscle glycogen more conservatively during
and gluconeogenesis, with minor contributions from the exercise(51). This sparing of glycogen with endurance train-
kidneys and intestine(5). When compared with the cap- ing is not specific to muscle, as the rate of liver glycogen util-
acity to store fat, the relatively limited capacity for isation is also attenuated in endurance-trained athletes
human subjects to store carbohydrate has implications compared with controls, particularly at moderate-to-high
for the ability to sustain moderate-to-high-intensity exer- exercise intensities(5). Evidence regarding whether gluco-
cise(5). Even amongst lean individuals (about 10 % body neogenesis is altered with endurance training is currently
fat), sufficient energy is stored as fat in adipose tissue to equivocal, as some studies indicate endurance training is
theoretically sustain moderate-to-high-intensity exercise associated with an increase in absolute rates of hepatic
https://doi.org/10.1017/S0029665118002604 Published online by Cambridge University Press
Sugars and liver metabolism 249
Proceedings of the Nutrition Society
Fig. 1. (Colour online) Major metabolic pathways of glucose, fructose and galactose in the human liver. TCA, tricarboxylic acid cycle;
P, phosphate; UDP, uridine diphosphate. Based on(10, 17, 23–26, 30–33).
gluconeogenesis(52), whereas others have shown reductions Since low carbohydrate availability is associated with
in hepatic gluconeogenesis after endurance training(52). impaired exercise tolerance, athletes engaging in competi-
When pooling all the currently published studies that have tive endurance events regularly consume carbohydrates
concomitantly estimated hepatic glycogenolysis and gluco- during exercise(70). When ingesting glucose alone, the max-
neogenesis(52–66), it is clear that endurance training is asso- imal rate at which human subjects can digest, absorb and
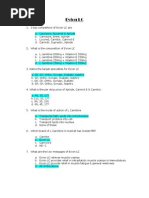
ciated with lower rates of glycogenolysis (Fig. 2(a), metabolise glucose is about 1 g/min(9), which typically
whereas any difference in gluconeogenesis with training sta- only represents about 44 % of total carbohydrate oxida-
tus and/or exercise intensity is relatively small and unlikely tion during exercise at moderate intensity (about 60 %
to be quantitatively important (Fig. 2(b). Furthermore, it is peak oxygen system) and is therefore insufficient to fully
apparent that hepatic glycogenolysis is the predominant meet the carbohydrate requirements of cycling-based exer-
source of blood glucose during exercise in an overnight cise(71). Consequently, oral ingestion of glucose is unable
fasted state, and the increase in endogenous glucose appear- to prevent muscle glycogen depletion during prolonged
ance with increasing exercise intensity is almost entirely met exercise(67). It is thought that the primary limitation to
by an increase in hepatic glycogenolysis, rather than gluco- the metabolism of orally ingested glucose lies in the
neogenesis (Fig. 2). splanchnic region, and intestinal absorption of glucose
Interactions between carbohydrate ingestion and exer- appears to be saturated at about 1 g/min(9). Ingesting glu-
cise occur on multiple levels and in both directions. cose at rates higher than 1 g/min during exercise is there-
Ingesting carbohydrates during exercise can increase fore likely to lead to accumulation of glucose in the gut
total carbohydrate oxidation and suppress net liver and cause gastrointestinal distress. Interestingly, combin-
glycogen utilisation and fat oxidation(67). Whereas even ing fructose with glucose appears to accelerate the diges-
modest exercise potently re-directs the metabolic fate of tion, absorption and utilisation of carbohydrate, such
orally ingested sugars. For example, 60 min cycling at that exogenous carbohydrate oxidation rates can reach
100 W performed 90 min after fructose ingestion diverts up to about 1·7 g/min, equating to about 70 % of total
more fructose away from storage (e.g. as glycogen) and carbohydrate oxidation(9,71). Under these conditions, the
increases fructose oxidation, without altering the conver- relative contribution from endogenous carbohydrate
sion of fructose to glucose(68). This may partly explain sources is therefore reduced from 100 % in the fasted
why daily exercise can completely prevent the increase state, to about 30 % with very high (2·5 g/min) carbohy-
in plasma TAG concentrations seen with high fructose drate ingestion rates(71). The primary mechanism by
intakes(69). Remarkably, the protection offered from which fructose–glucose mixtures can increase exogenous
exercise against fructose-induced hypertriglyceridemia is carbohydrate oxidation over glucose alone is thought to
seen independently from changes in net energy bal- be that intestinal fructose transport utilises a separate
ance(69), yet current recommendations for the health pathway than glucose. Specifically, whilst glucose absorp-
effects of dietary sugars rarely consider the context of tion via sodium dependent GLUT-1 is saturated at about
physical activity status. 1 g/min, fructose is primarily transported via GLUT5,
https://doi.org/10.1017/S0029665118002604 Published online by Cambridge University Press
250 J. T. Gonzalez and J. A. Betts
Fig. 2. (Colour online) Hepatic glycogenolysis (a) and gluconeogenesis (b) in endurance trained individuals and untrained
individuals. Each dot represents a group of participants or exercise intensity from a study, and error bars represent 95
Proceedings of the Nutrition Society
% CI (only calculated when published data were available to permit this). The shaded areas represent the 95 % CI of
the trend lines. Data are from(52–66).
thereby taking advantage of this alternative pathway and intestinal absorption pathway to glucose, combining
delivering more total carbohydrate to the system(9). galactose and glucose ingestion is unlikely to provide
the same benefits for exogenous carbohydrate availability
and endurance performance as glucose–fructose co-
Potential implications and applications ingestion.
In addition to manipulating carbohydrate availability
Exercise performance during exercise, dietary sugars can also play an important
The health and performance implications of carbohy- role during post-exercise recovery, particularly in multi-
drate intake can be dependent on the specific pathways stage events such as the Tour de France and the
through which different dietary sugars are absorbed Marathon des Sables, where athletes are required to per-
and metabolised. In terms of endurance performance, form to the best of their ability with <24 h recovery.
the accelerated digestion, absorption and utilisation of Within these scenarios, the primary limiting factor to
fructose–glucose mixtures above glucose only, has poten- recovery time is glycogen storage rate(48,76). Even with
tial benefits with regard to sparing glycogen stores whilst high carbohydrate intakes, it is thought to take between
minimising gastrointestinal distress during exercise(9). 20 and 24 h to fully restore muscle glycogen concentra-
Gastrointestinal complaints are relatively common in tions after exhaustive exercise(77). Thus, on moderate
endurance events(72), which may directly impair perform- carbohydrate diet, muscle glycogen repletion can take
ance, but also limit the ability to ingest adequate nutri- up to 46 h(78). Therefore, intensive nutritional strategies
tion to fuel the demands of the exercise. It has recently can be applied to optimise muscle glycogen resynthesis
been demonstrated that the ingestion of either glucose post-exercise. Post-exercise muscle glycogen resynthesis
alone, or sucrose (glucose–fructose) can prevent liver rates display a biphasic response, with the most rapid
glycogen depletion during prolonged (3 h) cycling at a net synthesis seen within the first 30 min following exercise
moderate exercise intensity (55 % VO2max)(67). Whilst in an insulin-independent phase(79). Following this period,
there was no further benefit of ingesting sucrose com- muscle glycogen synthesis rates become insulin-dependent
pared with glucose with respect to net liver glycogen and can fall to at least half the rate of that seen within the
depletion, the prevention of liver glycogen depletion first 30 min post-exercise(79). Muscle glycogen resynthesis
with sucrose ingestion was attained with lower ratings rates are maximally stimulated with carbohydrate inges-
of both gut discomfort and perceived exertion, compared tion rates of ≥1 g/kg body mass per h(48,76), and this inges-
with glucose ingestion(67). Furthermore, when carbohy- tion rate is also associated with optimal restoration of
drates are ingested in large amounts during exercise endurance capacity during short-term (4 h) recovery peri-
(>1·4 g/min), the ingestion of glucose–fructose enhances ods(76). Therefore, athletes are advised to consume carbo-
endurance performance by about 1–9 % more than hydrate at a rate of 1–1·2 g carbohydrate/kg body mass per
when glucose is ingested alone(73). Conversely, galactose h during the early stages (4 h) of recovery(47,48) and, when
appears to display relatively low rates of exogenous these ingestion rates are not achievable, the addition of
carbohydrate oxidation during exercise (about 0·4 g/min certain (insulinotropic) proteins, such as milk proteins,
oxidised, when ingesting about 1·2 g/min), despite an to carbohydrate can potentially increase the efficiency of
apparent potential for faster intestinal absorption of gal- muscle glycogen resynthesis(80).
actose compared with glucose in perfusion studies(74,75). Current sports nutrition guidelines for recovery do not
Moreover, since galactose primarily shares a common specify whether the carbohydrate should be from a
https://doi.org/10.1017/S0029665118002604 Published online by Cambridge University Press
Sugars and liver metabolism 251
particular source of sugar (e.g. glucose v. fructose v.
galactose)(47,48), which is understandable given that
muscle glycogen resynthesis rates do not appear to differ
whether glucose or glucose–fructose mixtures are
ingested(9,81), yet overlooks the clear potential for sugars
to differentially affect liver glycogen resynthesis. Indeed,
when pooling all currently published data that compare
glucose with glucose–fructose mixtures in crossover
designs(50,81–85), it is apparent that post-exercise muscle
glycogen resynthesis rates do not differ between glucose
ingested alone v. glucose–fructose (sucrose) mixtures
(Fig. 3(a)). Extrapolating these data would suggest that
22 h are required to completely re-synthesise muscle
glycogen from a fully depleted state, when following cur-
rent sports nutrition guidelines, regardless of the type of
carbohydrate ingested (Fig. 3(a)). This indicates that
intestinal absorption of carbohydrate is not rate-limiting
to post-exercise muscle glycogen resynthesis. Conversely,
Proceedings of the Nutrition Society
liver glycogen resynthesis appears to be potently acceler-
ated by glucose–fructose co-ingestion compared with glu-
cose (polymers) alone (Fig. 3(b))(33,50,81), which may be
in part due to greater exogenous carbohydrate availabil-
ity and/or the specific hepatic metabolism of fructose.
A further interesting observation is that liver glycogen
resynthesis rates also appear to show a bi-phasic, time-
dependent response, albeit in the opposite direction to Fig. 3. (Colour online) Studies (specified by reference citations) that
skeletal muscle. Within the first 2 h post-exercise, net have directly compared glucose ingestion alone, with either
liver glycogen resynthesis rates are about 30–50 % slower fructose–glucose or galactose–glucose mixtures, and measure rates
than the 3–5 h period, independent of the type of carbo- of muscle (a) and liver (b) glycogen repletion post-exercise. Each
hydrate ingested (2 (SE 2) and 5 (SE 2) g/h in the 0–2 h circle represents a timepoint within a study. Error bars represent 95
post-exercise v. 4 (SE 2) and 8 (SE 2) g/h in the 2–5 h post- % CI, and the shaded areas represent the 95 % CI of the trend line.
exercise, with glucose and sucrose ingestion, respect- For complete recovery of muscle glycogen stores, 600 mM/kgDM
ively)(81). Furthermore, with high rates of carbohydrate was chosen on the basis that muscle glycogen concentrations at
ingestion, fructose–glucose mixtures can reduce ratings exhaustion is typically about 115 mM/kgDM and the maximal muscle
glycogen concentrations of relatively well-trained athletes (60–70/ml/
of gut discomfort during recovery from exercise, com-
kg per min) is between 600 and 800 mM/kgDM(51). For complete
pared with glucose ingestion alone(81). Extrapolating recovery of liver glycogen stores, 80 g was chosen on the basis that
these data (i.e. assuming that the first 6·5 h is representa- liver glycogen concentrations in the overnight fasted state are about
tive of a full 24 h period) indicates that when only glu- 280 mM/l. Assuming a liver volume of 1·8 litre and the molar mass of
cose is ingested, complete recovery of liver glycogen a glycosyl unit being 162 g/M, this equates to 80 g glycogen(5).
stores may take about 25 h (Fig. 3(b)). However, when
glucose–fructose mixtures are ingested, then liver glyco-
gen repletion could take as little at 11 h (Fig. 3(b)). metabolism, why is the liver glycogenic response to gal-
When considering that the time between ending a stage actose ingestion more comparable to fructose than to
and beginning the next stage in the Tour de France can glucose? With regard to generating useful data for
be about 15 h, the accelerated recovery of liver glycogen applied practice, there is a need to establish the optimal
stores with fructose–glucose mixtures is highly meaning- dose and mixture of sugars for rapid liver glycogen
ful from a practical standpoint. resynthesis and whether this translates into improved
Interestingly, fructose is not the only sugar that more endurance performance. Accordingly, dose–response
rapidly replenishes liver glycogen contents following studies and direct comparisons of combined galactose–
exercise than glucose alone. The addition of galactose fructose–glucose are warranted.
to glucose also accelerates post-exercise liver glycogen Whilst the effects of fructose–glucose and galactose–
repletion when matched for total carbohydrate intake(33), glucose ingestion on glycogen resynthesis are interesting
and to a similar extent as fructose–glucose ingestion and likely to be important for athletic performance, this
(Fig. 3(b)). Since intestinal galactose–glucose absorption will remain speculative in the absence of empirical data.
should theoretically be slower than fructose–glucose Fortunately, a recent study compared the recovery of exer-
absorption, it is tempting to speculate that the mechan- cise capacity with glucose–maltodextrin ingestion v. fruc-
isms by which fructose and galactose enhance liver glyco- tose–maltodextrin ingestion(86). Since the maltodextrin
gen resynthesis relate to hepatic metabolism, rather than is hydrolysed, absorbed and oxidised as quickly as free
intestinal absorption. These data also raise the following glucose(9), it can be considered the glucose–maltodextrin
question: if the Leloir pathway (direct galactose–glucose is physiologically almost identical to ingesting pure glu-
conversion) is the primary pathway of human galactose cose. Athletes were first asked to run on a treadmill at
https://doi.org/10.1017/S0029665118002604 Published online by Cambridge University Press
252 J. T. Gonzalez and J. A. Betts
70 % V̇O2 max to exhaustion. Following this, the athletes insulin and TAG concentrations, and increase liver fat
ingested 90 g carbohydrate/h during a 4 h recovery period content, particularly in overweight/obese populations
as either a glucose–maltodextrin mixture, or fructose– and during positive energy balance(93,94). However,
maltodextrin mixture. After the recovery period, the some have shown that a positive energy balance and/or
athletes ran on the treadmill again at 70 % V̇O2 max to saturated fat intake are more potent drivers of liver fat
exhaustion. During the glucose–maltodextrin trial, the accumulation than specific effects of fructose over
second-bout capacity for these athletes to run was 61·4 glucose(95,96). The mechanisms underlying these meta-
(SE 9·6) min, whereas, when fructose–maltodextrin was bolic changes with fructose ingestion, are thought to
ingested in the recovery period, these athletes ran for include a suppression of hepatic insulin sensitivity to
81·4 (SE 22·3) min representing an improvement in glucose output, stimulation of de novo lipogenesis via
second-bout endurance capacity of about 30 %(86). This activation of pyruvate dehydrogenase (up-regulated
provides the first evidence that fructose–glucose ingestion when glycogen concentrations are high(97)), and a reduc-
accelerates recovery of exercise capacity. When considered tion in hepatic fatty acid oxidation, leading to increased
in light of the consistently reported acceleration of liver net lipid synthesis and VLDL-TAG production and
glycogen recovery, it may be sensible for athletes requiring secretion(10,69,94,98). This is consistent with data pertain-
rapid recovery during multi-stage events to consume fruc- ing to post-exercise glycogen resynthesis, since it is
tose–glucose mixtures rather than glucose only. In terms thought that insulin resistance to skeletal muscle glucose
of applying this in practice, it could mean the use of uptake (leading to hyperglycaemia) and de novo lipogen-
Proceedings of the Nutrition Society
fruit smoothies to supplement carbohydrate intake rather esis (leading to hypertriglyceridemia) are up-regulated
than the commonly held view that pasta is a preferable when glycogen stores are saturated(63,99,100). Furthermore,
choice for carbohydrate loading. during non-exercise conditions, the increase in postpran-
dial liver glycogen concentrations seen with a 7 d high-
glycaemic index diet occurs in tandem with increases in
Metabolic health liver fat content(101). The proposed relationship between
The impact of dietary sugars on hepatic metabolism also liver glycogen and lipid metabolism supports the idea
has potential metabolic health consequences. Public that regular exercise can obliterate the negative effects
health recommendations to limit intake of free sugars of fructose overfeeding in healthy men(8,69), since exercise
are primarily based on the effects of diets high in free results in rapid glycogen turnover, and there is clear
sugars on body weight and associations with dental car- evidence that the carbohydrate deficit from exercise is a
ies(11). However, distinct metabolic effects of fructose in key factor in exercise-induced increases in whole-body
particular receive much interest with respect to metabolic glucose control(102).
health. Metabolic health is typically characterised by the Whether exercise can be protective against fructose-
ability to maintain relatively stable blood glucose and induced hypertriglyceridaemia and changes in hepatic
lipid concentrations in the postprandial state(87), since insulin sensitivity in overweight and obese populations
high postprandial glucose and/or TAG concentrations remains to be established. Given the role of glycogen sta-
are associated with CVD(88,89). The ability to maintain tus in metabolic health, it could be speculated that, when
relatively stable circulating metabolite concentrations metabolic control is the primary aim, the avoidance of
with relatively little need for insulin represents an import- carbohydrates (and in particular fructose-containing
ant aspect of insulin sensitivity, which is thought to be a sugars) for periods before, during and/or after exercise
fundamental mechanism by which metabolic health is could better maintain some of the insulin-sensitising
sustained. Whilst insulin sensitivity is most commonly effects of exercise via greater liver glycogen depletion
associated with blood glucose control, the many regula- and delayed liver glycogen repletion (Fig. 3), but this
tory roles of insulin mean that insulin sensitivity is best has never been empirically assessed. Fructose can there-
considered with respect to the tissue of interest and func- fore induce changes that are associated with impaired
tion of interest. For example, insulin sensitivity of skel- metabolic health, but this appears to be primarily in sed-
etal muscle to glucose uptake, insulin sensitivity of the entary, overweight and obese individuals, and when in a
liver to glucose output, or insulin sensitivity of adipose positive energy balance. There is evidence that regular
tissue to lipolysis, etc. This is relevant when discussing exercise has the potential to protect against most (if not
the role of fructose in metabolic health as it is apparent all) of these metabolic effects, at least in healthy men.
that most of the metabolic effects of fructose occur in a Research is required to determine whether exercise can
tissue-specific manner. be protective against metabolic changes with fructose
The addition of fructose to other ingested nutrients supplementation in people at risk of metabolic disease,
can impact both postprandial glucose and lipid meta- and if so, then to characterise the lowest ‘dose’ of exercise
bolism. Low doses of fructose can in fact lower postpran- that is protective.
dial glycaemia via increased hepatic glucose disposal
secondary to fructose-1-P antagonisation of glucokinase
regulatory protein, and thereby enhanced hepatic gluco- Conclusions
kinase activity(90–92). However, compared with glucose
ingestion, fructose can enhance postprandial TAG con- The liver is a primary site of carbohydrate metabolism
centrations acutely(19) and supplementation of fructose and particularly the metabolism of fructose and
over days/weeks can increase fasting plasma glucose, galactose-containing sugars. Hepatic metabolism plays
https://doi.org/10.1017/S0029665118002604 Published online by Cambridge University Press
Sugars and liver metabolism 253
a key role in metabolic health and endurance exercise in young, healthy men that modest amounts of exercise
performance, by assisting in the maintenance of blood can completely protect against almost all of these poten-
glucose and lipid homeostasis during rapid changes in tially deleterious effects of high-fructose intakes, inde-
the supply and demand for energy, such as with fasting- pendent of energy balance. The protective effects of
feeding cycles and with physical activity. In the fasted exercise may be due to the carbohydrate deficit and/or
state, the liver provides almost all the glucose necessary glycogen turnover in the liver and skeletal muscle
to maintain blood glucose concentrations during exer- induced by physical activity. Accordingly, specifically
cise. As exercise intensity increases, thereby accelerating avoiding carbohydrates at key times: either before, dur-
the demand for glucose by skeletal muscle, the increase ing and/or after exercise to augment and preserve a
in liver glucose output is primarily met by releasing glycogen deficit could be a strategy to enhance metabolic
stored glucose from glycogen, rather than by increases health. However, it is not known if exercise can be
in de novo synthesis of glucose by gluconeogenesis. protective in populations at risk of metabolic disease,
Similarly, the reduction in liver glucose output during which should be a future research priority.
exercise seen in endurance-trained athletes compared
with untrained controls, is primarily driven by a
reduction in glycogenolysis, as opposed to changes in
gluconeogenesis. Therefore, prolonged exercise of a Financial Support
moderate-to-high intensity leads to a depletion of liver
Proceedings of the Nutrition Society
glycogen stores unless carbohydrate is ingested during J. T. G. has received research funding from The European
exercise, particularly in less-trained individuals. Society of Clinical Nutrition and Metabolism, The Rank
For endurance athletes who require rapid recovery for Prize Funds, The Physiological Society (UK), The
subsequent competitive events, restoration of skeletal Biotechnology and Biological Sciences Research
muscle and liver glycogen stores are a primary goal. Council (UK), The Medical Research Council (UK),
Carbohydrate ingestion is a requirement to replenish Arla Foods Ingredients, Lucozade Ribena Suntory and
glycogen stores within a 24 h timeframe, and ingesting Kenniscentrum Suiker and Voeding, and has acted as a
carbohydrate at a rate of about 1 g/kg body mass per h consultant to PepsiCo. J. A. B. has received research fund-
within the early (0–4 h) recovery period can assist in opti- ing from GlaxoSmithKline Nutritional Healthcare R&D,
mising this process. Whilst muscle glycogen repletion Lucozade Ribena Suntory and Kelloggs, has acted as a
appears to be largely unaffected by the specific presence consultant for Lucozade Ribena Suntory and PepsiCo
of fructose in ingested carbohydrates, liver glycogen and is a scientific advisor to the International Life
repletion rates are potently enhanced by the ingestion Sciences Institute Europe Task Force on Energy
of fructose- or galactose-containing sugars, when com- Balance. This research received no specific grant from
pared with glucose alone. There is evidence that the com- any funding agency, commercial or not-for-profit sectors.
plete restoration of liver glycogen stores after exhaustive
exercise could be accelerated by as much as 2-fold with
the ingestion of fructose–glucose mixtures, compared Conflict of Interest
with glucose-only carbohydrates. Therefore, athletes
with multiple competitive events within a 24 h period None.
should aim to consume about 1 g/kg body mass per h
carbohydrate with foods providing fructose and glucose.
Not only does this enhance restoration of liver (and
therefore total body) glycogen stores, there is now evi- Authorship
dence that this can reduce the gut discomfort associated
with high-carbohydrate ingestion rates, and improve J. T. G. wrote the initial draft of the manuscript. Both
endurance running capacity. There is, however further authors read, edited and approved of the final
work required to establish the optimal dose and mixture manuscript.
of carbohydrates to be ingested to maximise post-exercise
liver glycogen recovery.
The rapid restoration of liver glycogen stores is rele-
vant mainly to a small minority of the population References
engaging in relatively extreme events. Most people are 1. Daston L (2005) Scientific error and the ethos of belief. Soc
more concerned about their health than competing in Res (New York) 72, 18.
an ultra-endurance event. However, the same knowledge 2. Young FG (1957) Claude Bernard and the discovery of
gained about the physiological responses to dietary glycogen: a century of retrospect. BMJ 1, 1431–1437.
sugars and exercise, particularly hepatic metabolism, 3. Bernard C (1855) Leçons de physiologie expérimentale
appliquée à la médecine, 1: faites au Collége de France.
can also be applied to improve metabolic health.
Chez J-B Baillière 1, 1–510.
Fructose-containing sugars have been implicated in indu- 4. Bernard C (1879) Leçons sur les phénomènes de la vie com-
cing hyperglycaemia, hypertriglyceridaemia, hepatic muns aux animaux et aux végétaux, vol. 2. Paris: Baillière.
insulin resistance and increases in liver fat content, par- 5. Gonzalez JT, Fuchs CJ, Betts JA et al. (2016) Liver glyco-
ticularly in overweight/obese populations and when in a gen metabolism during and after prolonged endurance-type
positive energy balance. Interestingly, there is evidence exercise. Am J Physiol Endocrinol Metab 311, E543–E553.
https://doi.org/10.1017/S0029665118002604 Published online by Cambridge University Press
254 J. T. Gonzalez and J. A. Betts
6. Jang C, Hui S, Lu W et al. (2018) The small intestine con- lipogenesis following carbohydrate consumption. Genome
verts dietary fructose into glucose and organic acids. Cell Biol 19, 79.
Metab 27, 351–361.e353. 28. Timson DJ & Reece RJ (2003) Functional analysis of
7. Mutel E, Gautier-Stein A, Abdul-Wahed A et al. (2011) disease-causing mutations in human galactokinase. Eur J
Control of blood glucose in the absence of hepatic glucose Biochem 270, 1767–1774.
production during prolonged fasting in mice: induction of 29. Sørensen M, Mikkelsen KS, Frisch K et al. (2011) Hepatic
renal and intestinal gluconeogenesis by glucagon. Diabetes galactose metabolism quantified in humans using
60, 3121–3131. 2-18F-fluoro-2-deoxy-D-galactose PET/CT. J Nucl Med
8. Gonzalez JT & Betts JA (2018) Dietary fructose metabol- 52, 1566–1572.
ism by splanchnic organs: size matters. Cell Metab 27, 30. Sunehag AL & Haymond MW (2002) Splanchnic galactose
483–485. extraction is regulated by coingestion of glucose in humans.
9. Gonzalez JT, Fuchs CJ, Betts JA et al. (2017) Glucose plus Metabolism 51, 827–832.
fructose ingestion for post-exercise recovery-greater than 31. Coss-Bu JA, Sunehag AL & Haymond MW (2009)
the sum of its parts? Nutrients 9, E344–E359. Contribution of galactose and fructose to glucose homeo-
10. Tappy L & Lê KA (2010) Metabolic effects of fructose and stasis. Metabolism 58, 1050–1058.
the worldwide increase in obesity. Physiol Rev 90, 23–46. 32. Niewoehner CB, Neil B & Martin T (1990) Hepatic uptake
11. World Health Organization (2015) Guideline: Sugars and metabolism of oral galactose in adult fasted rats. Am J
Intake for Adults and Children. Geneva: World health Physiol 259, E804–E813.
Organization. 33. Décombaz J, Jentjens R, Ith M et al. (2011) Fructose and
Proceedings of the Nutrition Society
12. Scientific Advisory Committee on Nutrition (2015) galactose enhance postexercise human liver glycogen
Carbohydrates and Health. London: TSO. synthesis. Med Sci Sports Exerc 43, 1964–1971.
13. Hawley JA, Dennis SC, Laidler BJ et al. (1991) High rates 34. van Loon LJ, Greenhaff PL, Constantin-Teodosiu D et al.
of exogenous carbohydrate oxidation from starch ingested (2001) The effects of increasing exercise intensity on muscle
during prolonged exercise. J Appl Physiol (1985) 71, fuel utilisation in humans. J Physiol 536, 295–304.
1801–1806. 35. Achten J, Venables MC & Jeukendrup AE (2003) Fat
14. Daniel H & Zietek T (2015) Taste and move: glucose and oxidation rates are higher during running compared with
peptide transporters in the gastrointestinal tract. Exp cycling over a wide range of intensities. Metabolism 52,
Physiol 100, 1441–1450. 747–752.
15. Kelley D, Mitrakou A, Marsh H et al. (1988) Skeletal mus- 36. Chen YC, Travers RL, Walhin JP et al. (2017) Feeding
cle glycolysis, oxidation, and storage of an oral glucose influences adipose tissue responses to exercise in overweight
load. J Clin Invest 81, 1563–1571. men. Am J Physiol Endocrinol Metab 313, E84–E93.
16. Ferrannini E, Bjorkman O, Reichard GA et al. (1985) The 37. Gonzalez JT, Veasey RC, Rumbold PL et al. (2013)
disposal of an oral glucose load in healthy subjects. A Breakfast and exercise contingently affect postprandial
quantitative study. Diabetes 34, 580–588. metabolism and energy balance in physically active
17. Williams CA (1986) Metabolism of lactose and galactose in males. Br J Nutr 110, 721–732.
man. Prog Biochem Pharmacol 21, 219–247. 38. Edinburgh RM, Hengist A, Smith HA et al. (2018)
18. Ercan N, Nuttall FQ, Gannon MC et al. (1993) Effects of Pre-exercise breakfast ingestion versus extended overnight
glucose, galactose, and lactose ingestion on the plasma glu- fasting increases postprandial glucose flux after exercise in
cose and insulin response in persons with non-insulin- healthy men. Am J Physiol – Endocrinol Metab Accepted-
dependent diabetes mellitus. Metabolism 42, 1560–1567. ahead-of-print doi: 10.1152/ajpendo.00163.
19. Chong MF, Fielding BA & Frayn KN (2007) Mechanisms 39. van Loon LJ, Jeukendrup AE, Saris WH et al. (1999)
for the acute effect of fructose on postprandial lipemia. Am Effect of training status on fuel selection during submaxi-
J Clin Nutr 85, 1511–1520. mal exercise with glucose ingestion. J Appl Physiol (1985)
20. Heinz F, Lamprecht W & Kirsch J (1968) Enzymes of 87, 1413–1420.
fructose metabolism in human liver. J Clin Invest 47, 40. Fletcher G, Eves FF, Glover EI et al. (2017) Dietary intake
1826–1832. is independently associated with the maximal capacity for
21. Adelman RC, Ballard FJ & Weinhouse S (1967) fat oxidation during exercise. Am J Clin Nutr 105, 864–872.
Purification and properties of rat liver fructokinase. 41. Romijn JA, Coyle EF, Sidossis LS et al. (1993) Regulation
J Biol Chem 242, 3360–3365. of endogenous fat and carbohydrate metabolism in relation
22. Hers HG & Kusaka T (1953) The metabolism of to exercise intensity and duration. Am J Physiol 265,
fructose-1-phosphate in the liver. Biochim Biophys Acta E380–E391.
11, 427–437. 42. Walter G, Vandenborne K, Elliott M et al. (1999) In vivo
23. Mayes PA (1993) Intermediary metabolism of fructose. Am ATP synthesis rates in single human muscles during high
J Clin Nutr 58, 754S–765S. intensity exercise. J Physiol 519, 901–910.
24. Björkman O, Gunnarsson R, Hagström E et al. (1989) 43. Hultman E & Harris RC (1988) Carbohydrate metabolism,
Splanchnic and renal exchange of infused fructose in Principles of Exercise Biochemistry. Basel, Switzerland: S.
insulin-deficient type 1 diabetic patients and healthy Karger.
controls. J Clin Invest 83, 52–59. 44. Jeukendrup AE & Wallis GA (2005) Measurement of sub-
25. Bar-On H & Stein Y (1968) Effect of glucose and fructose strate oxidation during exercise by means of gas exchange
administration on lipid metabolism in the rat. J Nutr 94, measurements. Int J Sports Med 26(Suppl. 1), S28–S37.
95–105. 45. Ørtenblad N, Westerblad H & Nielsen J (2013) Muscle
26. Carmona A & Freedland RA (1989) Comparison among glycogen stores and fatigue. J Physiol 591, 4405–4413.
the lipogenic potential of various substrates in rat hepato- 46. Ørtenblad N & Nielsen J (2015) Muscle glycogen and cell
cytes: the differential effects of fructose-containing diets function – location, location, location. Scand J Med Sci
on hepatic lipogenesis. J Nutr 119, 1304–1310. Sports 25(Suppl. 4), 34–40.
27. Sanders FWB, Acharjee A, Walker C et al. (2018) Hepatic 47. Thomas DT, Erdman KA & Burke LM (2016) American
steatosis risk is partly driven by increased de novo college of sports medicine joint position statement.
https://doi.org/10.1017/S0029665118002604 Published online by Cambridge University Press
Sugars and liver metabolism 255
Nutrition and athletic performance. Med Sci Sports Exerc 65. Emhoff CA, Messonnier LA, Horning MA et al. (2013)
48, 543–568. Gluconeogenesis and hepatic glycogenolysis during exer-
48. Burke LM, van Loon LJC & Hawley JA (2017) cise at the lactate threshold. J Appl Physiol (1985) 114,
Postexercise muscle glycogen resynthesis in humans. 297–306.
J Appl Physiol (1985) 122, 1055–1067. 66. Webster CC, Noakes TD, Chacko SK et al. (2016)
49. Bergström J, Hermansen L, Hultman E et al. (1967) Diet, Gluconeogenesis during endurance exercise in cyclists habi-
muscle glycogen and physical performance. Acta Physiol tuated to a long-term low carbohydrate high fat diet. J
Scand 71, 140–150. Physiol 594, 4389–4405.
50. Casey A, Mann R, Banister K et al. (2000) Effect of 67. Gonzalez JT, Fuchs CJ, Smith FE et al. (2015) Ingestion of
carbohydrate ingestion on glycogen resynthesis in human glucose or sucrose prevents liver but not muscle glycogen
liver and skeletal muscle, measured by (13)C MRS. Am J depletion during prolonged endurance-type exercise in
Physiol Endocrinol Metab 278, E65–E75. trained cyclists. Am J Physiol Endocrinol Metab 309,
51. Areta JL & Hopkins WG (2018) Skeletal muscle glycogen E1032–E1039.
content at rest and during endurance exercise in humans: a 68. Egli L, Lecoultre V, Cros J et al. (2016) Exercise performed
meta-analysis. Sports Med 48, 2091–2102. immediately after fructose ingestion enhances fructose oxi-
52. Bergman BC, Horning MA, Casazza GA et al. (2000) dation and suppresses fructose storage. Am J Clin Nutr 103,
Endurance training increases gluconeogenesis during rest 348–355.
and exercise in men. Am J Physiol Endocrinol Metab 278, 69. Egli L, Lecoultre V, Theytaz F et al. (2013) Exercise pre-
E244–E251. vents fructose-induced hypertriglyceridemia in healthy
Proceedings of the Nutrition Society
53. Wahren J, Felig P, Ahlborg G et al. (1971) Glucose young subjects. Diabetes 62, 2259–2265.
metabolism during leg exercise in man. J Clin Invest 50, 70. Saris WH, van Erp-Baart MA, Brouns F et al. (1989) Study
2715–2725. on food intake and energy expenditure during extreme sus-
54. Ahlborg G, Felig P, Hagenfeldt L et al. (1974) Substrate tained exercise: the Tour de France. Int J Sports Med 10
turnover during prolonged exercise in man. Splanchnic (Suppl. 1), S26–S31.
and leg metabolism of glucose, free fatty acids, and 71. Jentjens RL, Achten J & Jeukendrup AE (2004) High oxi-
amino acids. J Clin Invest 53, 1080–1090. dation rates from combined carbohydrates ingested during
55. Sestoft L, Trap-Jensen J, Lyngsooe J et al. (1977) exercise. Med Sci Sports Exerc 36, 1551–1558.
Regulation of gluconeogenesis and ketogenesis during rest 72. Pfeiffer B, Stellingwerff T, Hodgson AB et al. (2012)
and exercise in diabetic subjects and normal men. Clin Nutritional intake and gastrointestinal problems during
Sci Mol Med 53, 411–418. competitive endurance events. Med Sci Sports Exerc 44,
56. Stanley WC, Wisneski JA, Gertz EW et al. (1988) Glucose 344–351.
and lactate interrelations during moderate-intensity exer- 73. Rowlands DS, Houltham S, Musa-Veloso K et al. (2015)
cise in humans. Metabolism 37, 850–858. Fructose-glucose composite carbohydrates and endurance
57. Friedlander AL, Casazza GA, Horning MA et al. (1997) performance: critical review and future perspectives.
Training-induced alterations of glucose flux in men. Sports Med 45, 1561–1576.
J Appl Physiol (1985) 82, 1360–1369. 74. Holdsworth CD & Dawson AM (1964) The absorption of
58. Friedlander AL, Casazza GA, Horning MA et al. (1998) monosaccharides in man. Clin Sci 27, 371–379.
Training-induced alterations of carbohydrate metabolism 75. Cook GC (1977) Rates and mechanisms of glucose, galact-
in women: women respond differently from men. J Appl ose, and xylose absorption in man in vivo. Scand J
Physiol (1985) 85, 1175–1186. Gastroenterol 12, 733–737.
59. Lavoie C, Ducros F, Bourque J et al. (1997) Glucose 76. Alghannam AF, Gonzalez JT & Betts JA (2018)
metabolism during exercise in man: the role of insulin Restoration of muscle glycogen and functional capacity:
and glucagon in the regulation of hepatic glucose produc- role of post-exercise carbohydrate and protein co-ingestion.
tion and gluconeogenesis. Can J Physiol Pharmacol 75, Nutrients 10, E253–E280.
26–35. 77. Coyle EF (1991) Timing and method of increased carbohy-
60. Trimmer JK, Schwarz JM, Casazza GA et al. (2002) drate intake to cope with heavy training, competition and
Measurement of gluconeogenesis in exercising men by recovery. J Sports Sci 9, 29–51; discussion 51–22.
mass isotopomer distribution analysis. J Appl Physiol 78. Piehl K (1974) Time course for refilling of glycogen stores
(1985) 93, 233–241. in human muscle fibres following exercise-induced glycogen
61. Roef MJ, Kalhan SC, Reijngoud DJ et al. (2002) Lactate depletion. Acta Physiol Scand 90, 297–302.
disposal via gluconeogenesis is increased during exercise 79. Price TB, Rothman DL, Taylor R et al. (1994) Human mus-
in patients with mitochondrial myopathy due to complex cle glycogen resynthesis after exercise: insulin-dependent
I deficiency. Pediatr Res 51, 592–597. and -independent phases. J Appl Physiol (1985) 76, 104–111.
62. Roef MJ, de Meer K, Kalhan SC et al. (2003) 80. Betts JA & Williams C (2010) Short-term recovery from
Gluconeogenesis in humans with induced hyperlactatemia prolonged exercise: exploring the potential for protein
during low-intensity exercise. Am J Physiol Endocrinol ingestion to accentuate the benefits of carbohydrate supple-
Metab 284, E1162–E1171. ments. Sports Med 40, 941–959.
63. Petersen KF, Price TB & Bergeron R (2004) Regulation of 81. Fuchs CJ, Gonzalez JT, Beelen M et al. (2016) Sucrose
net hepatic glycogenolysis and gluconeogenesis during ingestion after exhaustive exercise accelerates liver, but not
exercise: impact of type 1 diabetes. J Clin Endocrinol muscle glycogen repletion compared with glucose ingestion
Metab 89, 4656–4664. in trained athletes. J Appl Physiol (1985) 120, 1328–1334.
64. Huidekoper HH, Ackermans MT, Koopman R et al. 82. Blom PC, Høstmark AT, Vaage O et al. (1987) Effect of
(2013) Normal rates of whole-body fat oxidation and glu- different post-exercise sugar diets on the rate of muscle
coneogenesis after overnight fasting and moderate-intensity glycogen synthesis. Med Sci Sports Exerc 19, 491–496.
exercise in patients with medium-chain acyl-CoA dehydro- 83. Bowtell JL, Gelly K, Jackman ML et al. (2000) Effect of
genase deficiency. J Inherit Metab Dis 36, 831–840. different carbohydrate drinks on whole body carbohydrate
https://doi.org/10.1017/S0029665118002604 Published online by Cambridge University Press
256 J. T. Gonzalez and J. A. Betts
storage after exhaustive exercise. J Appl Physiol (1985) 88, decreases insulin sensitivity in overweight/obese humans.
1529–1536. J Clin Invest 119, 1322–1334.
84. Wallis GA, Hulston CJ, Mann CH et al. (2008) Postexercise 94. Lecoultre V, Egli L, Carrel G et al. (2013) Effects of fruc-
muscle glycogen synthesis with combined glucose and fruc- tose and glucose overfeeding on hepatic insulin sensitivity
tose ingestion. Med Sci Sports Exerc 40, 1789–1794. and intrahepatic lipids in healthy humans. Obesity (Silver
85. Trommelen J, Beelen M, Pinckaers PJ et al. (2016) Spring) 21, 782–785.
Fructose coingestion does not accelerate postexercise mus- 95. Johnston RD, Stephenson MC, Crossland H et al. (2013)
cle glycogen repletion. Med Sci Sports Exerc 48, 907–912. No difference between high-fructose and high-glucose
86. Maunder E, Podlogar T & Wallis GA (2018) Postexercise diets on liver triacylglycerol or biochemistry in healthy
fructose-maltodextrin ingestion enhances subsequent overweight men. Gastroenterology 145, 1016–1025.e1012.
endurance capacity. Med Sci Sports Exerc 50, 1039–1045. 96. Luukkonen PK, Sädevirta S, Zhou Y et al. (2018)
87. Edinburgh RM, Betts JA, Burns SF et al. (2017) Saturated fat is more metabolically harmful for the
Concordant and divergent strategies to improve postpran- human liver than unsaturated fat or simple sugars.
dial glucose and lipid metabolism. Nutrition Bulletin 42, Diabetes Care 41, 1732–1739.
113–122. 97. Kiilerich K, Gudmundsson M, Birk JB et al. (2010) Low
88. Nordestgaard BG, Benn M, Schnohr P et al. (2007) muscle glycogen and elevated plasma free fatty acid modify
Nonfasting triglycerides and risk of myocardial infarction, but do not prevent exercise-induced PDH activation in
ischemic heart disease, and death in men and women. J Am human skeletal muscle. Diabetes 59, 26–32.
Med Assoc 298, 299–308. 98. Park OJ, Cesar D, Faix D et al. (1992) Mechanisms of
Proceedings of the Nutrition Society
89. Ning F, Zhang L, Dekker JM et al. (2012) Development of fructose-induced hypertriglyceridaemia in the rat. Activation
coronary heart disease and ischemic stroke in relation to of hepatic pyruvate dehydrogenase through inhibition of
fasting and 2-hour plasma glucose levels in the normal pyruvate dehydrogenase kinase. Biochem J 282, 753–757.
range. Cardiovasc Diabetol 11, 76. 99. Rabøl R, Petersen KF, Dufour S et al. (2011) Reversal of
90. Van Schaftingen E, Detheux M & Veiga da Cunha M muscle insulin resistance with exercise reduces postprandial
(1994) Short-term control of glucokinase activity: role of hepatic de novo lipogenesis in insulin resistant individuals.
a regulatory protein. FASEB J 8, 414–419. Proc Natl Acad Sci USA 108, 13705–13709.
91. Donmoyer CM, Ejiofor J, Lacy DB et al. (2001) Fructose 100. Nolte LA, Gulve EA & Holloszy JO (1994)
augments infection-impaired net hepatic glucose uptake Epinephrine-induced in vivo muscle glycogen depletion
during TPN administration. Am J Physiol Endocrinol enhances insulin sensitivity of glucose transport. J Appl
Metab 280, E703–E711. Physiol (1985) 76, 2054–2058.
92. Sievenpiper JL, Chiavaroli L, de Souza RJ et al. (2012) 101. Bawden S, Stephenson M, Falcone Y et al. (2017)
‘Catalytic’ doses of fructose may benefit glycaemic control Increased liver fat and glycogen stores after consumption
without harming cardiometabolic risk factors: a small of high versus low glycaemic index food: a randomized
meta-analysis of randomised controlled feeding trials. Br crossover study. Diabetes Obes Metab 19, 70–77.
J Nutr 108, 418–423. 102. Taylor HL, Wu CL, Chen YC et al. (2018) Post-exercise
93. Stanhope KL, Schwarz JM, Keim NL et al. (2009) carbohydrate-energy replacement attenuates insulin sensi-
Consuming fructose-sweetened, not glucose-sweetened, tivity and glucose tolerance the following morning in
beverages increases visceral adiposity and lipids and healthy adults. Nutrients 10, E123–E134.
https://doi.org/10.1017/S0029665118002604 Published online by Cambridge University Press
You might also like
- Lee Your Pocketbook Guide To The Ultimate Gym Workout 2020Document156 pagesLee Your Pocketbook Guide To The Ultimate Gym Workout 2020Angel Caméléon100% (2)
- 101 - Ways PDF Yuri ElkainDocument208 pages101 - Ways PDF Yuri ElkainStudentMadHouse100% (4)
- Liverglycogen Metabolism ExerciseDocument11 pagesLiverglycogen Metabolism ExerciseGabriela SolanoNo ratings yet
- The-Nutrition-X-Change-Vol.-4-Carbohydrate-Intake-During-ExerciseDocument12 pagesThe-Nutrition-X-Change-Vol.-4-Carbohydrate-Intake-During-ExercisepeppesmatheusNo ratings yet
- Post Exercice Repletion of Muscle Energy Stores With Fructose or Glucose in Mixed MealsDocument9 pagesPost Exercice Repletion of Muscle Energy Stores With Fructose or Glucose in Mixed MealsLeonardo PinheiroNo ratings yet
- Ajcn 138214Document9 pagesAjcn 138214Gustavo AlmeidaNo ratings yet
- 44 Effect of Different Carbohydrate Drinks On Whole BodyDocument8 pages44 Effect of Different Carbohydrate Drinks On Whole BodyFerroBemNo ratings yet
- Fundamentals of Glycogen.Document17 pagesFundamentals of Glycogen.Kevin VillaNo ratings yet
- HMS 4601 Case 3Document4 pagesHMS 4601 Case 3stijn.berkmortel1No ratings yet
- Def Ronzo 2016Document32 pagesDef Ronzo 2016RachmatBimanjayaNo ratings yet
- The Glucose Fatty-Acid Cycle. Its Role In... (Randle1963) Randle CycleDocument5 pagesThe Glucose Fatty-Acid Cycle. Its Role In... (Randle1963) Randle CycleFilip ZaleskiNo ratings yet
- The Role of Liver in Metabolism An Updated ReviewDocument6 pagesThe Role of Liver in Metabolism An Updated Reviewرشاد خالد عماد Rashad Khaled EmadNo ratings yet
- bsr036e416Document15 pagesbsr036e416Amina MiminaNo ratings yet
- JA - 477 - Botezelli Et Al 2010Document8 pagesJA - 477 - Botezelli Et Al 2010jailtongpNo ratings yet
- Carbohidratos en La Nutrición Humana Por La FaoDocument8 pagesCarbohidratos en La Nutrición Humana Por La Faomarco antonioNo ratings yet
- Vi. Metabolic Effects of Carbohydrate and Fiber in Type 2 Diabetes A. Single Meal StudiesDocument10 pagesVi. Metabolic Effects of Carbohydrate and Fiber in Type 2 Diabetes A. Single Meal StudiesFelix Radivta Ginting100% (1)
- Abastecendo o Atleta Com Diabetes Tipo 1Document7 pagesAbastecendo o Atleta Com Diabetes Tipo 1josiNo ratings yet
- Effect of Insulin On Carbohydrate MetabolismDocument3 pagesEffect of Insulin On Carbohydrate MetabolismfrnksusNo ratings yet
- Carbohydrates-Structure-metabolism-and-biochemistryDocument7 pagesCarbohydrates-Structure-metabolism-and-biochemistryVarun KaushikNo ratings yet
- CarbohidratosduranteEjercicio PDFDocument9 pagesCarbohidratosduranteEjercicio PDFTuning El EquipoNo ratings yet
- Training The Gut For AthletesDocument10 pagesTraining The Gut For AthletesJULIETANo ratings yet
- Glycogen Storage Capacity and de Novo Iipogenesis During Massive Carbohydrate Overfeeding in ManDocument9 pagesGlycogen Storage Capacity and de Novo Iipogenesis During Massive Carbohydrate Overfeeding in ManSalvio EspositoNo ratings yet
- Insulin Action in Hyperthyroidism - Doc (Biokom)Document16 pagesInsulin Action in Hyperthyroidism - Doc (Biokom)Suwantin Indra SariNo ratings yet
- Polydextrose and Weight ManagementDocument4 pagesPolydextrose and Weight Managementchef Sergio rojasNo ratings yet
- Rat Hepatocyte Glucose Metabolism Is Affected by Caloric Restriction But Not by Litter Size ReductionDocument8 pagesRat Hepatocyte Glucose Metabolism Is Affected by Caloric Restriction But Not by Litter Size ReductionSabrina JonesNo ratings yet
- jcinvest00138-0019Document9 pagesjcinvest00138-0019JagadeeshNo ratings yet
- Kuliah Biokimia Blok 2.4.1Document44 pagesKuliah Biokimia Blok 2.4.1Prajna PNo ratings yet
- Group 7 - HW No.4Document4 pagesGroup 7 - HW No.4MoreartiNo ratings yet
- Glycogen Storage Capacity and de Novo Lipogenesis During Massive Carbohydrate Overfeeding in ManDocument8 pagesGlycogen Storage Capacity and de Novo Lipogenesis During Massive Carbohydrate Overfeeding in ManmarkymarknyNo ratings yet
- Carbohydrate 3Document43 pagesCarbohydrate 3mahiaddis2112No ratings yet
- New Perspectives On Nutritional Interventions To Augment Lipid Utilisation During ExerciseDocument12 pagesNew Perspectives On Nutritional Interventions To Augment Lipid Utilisation During ExerciseDani Prado GamboaNo ratings yet
- Gluconeogenesis & Cori CycleDocument25 pagesGluconeogenesis & Cori CyclecimdesadesuNo ratings yet
- GlycogenesisDocument11 pagesGlycogenesisinsanwijaya15No ratings yet
- METABOLISM (Academic Notes)Document6 pagesMETABOLISM (Academic Notes)ryanescueta090702No ratings yet
- Glycogen Replenishment After Exhaustive ExerciseDocument3 pagesGlycogen Replenishment After Exhaustive ExercisePOP CRISTIANNo ratings yet
- Basics in Clinical Nutrition: Carbohydrate Metabolism: Luc TappyDocument4 pagesBasics in Clinical Nutrition: Carbohydrate Metabolism: Luc Tappymarliana100% (1)
- DMJ 2021 0280Document23 pagesDMJ 2021 0280Helder CarvalhoNo ratings yet
- Book Chapter Carbohydrate Storage and MetabolismDocument16 pagesBook Chapter Carbohydrate Storage and Metabolismq8laNo ratings yet
- Ingles 2 Carbohidratos PDFDocument4 pagesIngles 2 Carbohidratos PDFIsabela OrihuelaNo ratings yet
- SEM-11-Starvation Saudek Felig 1976Document10 pagesSEM-11-Starvation Saudek Felig 1976TomasNo ratings yet
- Week 9 10. MetabolismDocument37 pagesWeek 9 10. MetabolismKatherine bundalianNo ratings yet
- محاظره ٦ كيمياDocument5 pagesمحاظره ٦ كيمياbzqgx7nnf7No ratings yet
- TS 1 PART 1 and 2 Carbohydrate Metabolism Calculation of Energy Balance English VersionDocument13 pagesTS 1 PART 1 and 2 Carbohydrate Metabolism Calculation of Energy Balance English Versionyacinebou10No ratings yet
- Document 6Document9 pagesDocument 6mraza17No ratings yet
- _.....Gluconeogenesis is & - Copy (1)Document21 pages_.....Gluconeogenesis is & - Copy (1)ibroo9395No ratings yet
- 8glycogen Metabolism2013 PDFDocument90 pages8glycogen Metabolism2013 PDFNazeer Baig MogalmearjaNo ratings yet
- The FEBS Journal - 2020 - Zhang - Beyond Energy Storage Roles of Glycogen Metabolism in Health and DiseaseDocument12 pagesThe FEBS Journal - 2020 - Zhang - Beyond Energy Storage Roles of Glycogen Metabolism in Health and Diseasecahyamasita14No ratings yet
- Fasting As Therapy - A Review: Senior Lecturer, MAHSA University, Selangor, MalaysiaDocument12 pagesFasting As Therapy - A Review: Senior Lecturer, MAHSA University, Selangor, Malaysialaiba ansariNo ratings yet
- Proses Pembentukan Energi Pada Saat Puasa: Zefanya Merryani 102012308Document18 pagesProses Pembentukan Energi Pada Saat Puasa: Zefanya Merryani 102012308Zefanya MNo ratings yet
- Beyond Weight Loss A Review of The Therapeutic Uses of Very-Low-Carbohydrate (Ketogenic) DietsDocument8 pagesBeyond Weight Loss A Review of The Therapeutic Uses of Very-Low-Carbohydrate (Ketogenic) DietsmrsilvNo ratings yet
- Insulin ResponseDocument7 pagesInsulin ResponsechloethefasionqueenNo ratings yet
- Carbohydrates ERTDocument10 pagesCarbohydrates ERTCharlotte WhiteNo ratings yet
- Glucose (GLC), A Monosaccharide (Or Simple Sugar) Also Known As Grape Sugar, Blood Sugar, or Corn Sugar, Is A VeryDocument4 pagesGlucose (GLC), A Monosaccharide (Or Simple Sugar) Also Known As Grape Sugar, Blood Sugar, or Corn Sugar, Is A VeryHak Gwaye100% (1)
- GluconeogenesisDocument9 pagesGluconeogenesisPankaj Singh PatelNo ratings yet
- Regulation of Hepatic Glucose Metabolism in Health and DiseaseDocument36 pagesRegulation of Hepatic Glucose Metabolism in Health and DiseaseMohammad Hadi SahebiNo ratings yet
- 3. L-arabinose co-ingestion delays glucose absorption derived from sucrose in healthy men and women a double-blind, randomised crossover trialDocument10 pages3. L-arabinose co-ingestion delays glucose absorption derived from sucrose in healthy men and women a double-blind, randomised crossover trialxinyun.gkbiomyNo ratings yet
- Carbohydrates PDFDocument8 pagesCarbohydrates PDFWrigley PatioNo ratings yet
- Effects of Carbohydrate Branched Chain ADocument11 pagesEffects of Carbohydrate Branched Chain AFelipe FerreiraNo ratings yet
- Different Glycemic Indexes of Breakfast Cereals Are Not Due To Glucose Entry Into Blood But To Glucose Removal by TissueDocument7 pagesDifferent Glycemic Indexes of Breakfast Cereals Are Not Due To Glucose Entry Into Blood But To Glucose Removal by TissueMaria Julia Ogna EgeaNo ratings yet
- Carbohydrates Metabolism (Med @2015)Document151 pagesCarbohydrates Metabolism (Med @2015)mulatu.it.dtuNo ratings yet
- Review Glucocorticoids and Fatty Acid Metabolism in Humans: Fuelling Fat Redistribution in The Metabolic SyndromeDocument16 pagesReview Glucocorticoids and Fatty Acid Metabolism in Humans: Fuelling Fat Redistribution in The Metabolic SyndromeCorona FingerNo ratings yet
- 2016 Quarterly Nutrition Program Accomplishment Report Olongapo CityDocument8 pages2016 Quarterly Nutrition Program Accomplishment Report Olongapo CityJohn Arbrith Esposo100% (1)
- Chapathi With Underutilized Seeds and Food WasteDocument70 pagesChapathi With Underutilized Seeds and Food WasteRuby JayaseelanNo ratings yet
- BMI Girl TableDocument7 pagesBMI Girl TableVienny Widhyanti RosaryaNo ratings yet
- Ch03 NutritionDocument12 pagesCh03 NutritionShelly-ann Richards-FrancisNo ratings yet
- Nutrition in PlantsDocument4 pagesNutrition in PlantsAaron Dave CanteroNo ratings yet
- Konseling PD Anak ObesitasDocument6 pagesKonseling PD Anak Obesitasage prasetyoNo ratings yet
- Microbialqualityofyoughurts AmeJFSNRes 26 2015Document9 pagesMicrobialqualityofyoughurts AmeJFSNRes 26 2015Cut MutiaNo ratings yet
- Pepf02 Revised Module 2Document19 pagesPepf02 Revised Module 2Reymar CabreraNo ratings yet
- Lifestyle and Weight Management Pe9Document39 pagesLifestyle and Weight Management Pe9Bea Valerie GrislerNo ratings yet
- CSEC Human and Social Biology Paper 2 2014Document3 pagesCSEC Human and Social Biology Paper 2 2014jules blancoNo ratings yet
- Mengantisipasi Regulasi Seputar Allergen (BPOM)Document21 pagesMengantisipasi Regulasi Seputar Allergen (BPOM)ARdian RizkyNo ratings yet
- Complementary FeedingDocument53 pagesComplementary FeedingWilliam C ChishaNo ratings yet
- Smoking Meat and PoultryDocument2 pagesSmoking Meat and PoultryurieoNo ratings yet
- 12 Home Science EMDocument8 pages12 Home Science EMZara KhanNo ratings yet
- Health Nutrition and Safety Prefinals 2Document2 pagesHealth Nutrition and Safety Prefinals 2yvhannieNo ratings yet
- Egg NOTESDocument4 pagesEgg NOTESReal AnNo ratings yet
- TAURINE The Key To Restoring Metabolic Function - Ray Peat ForumDocument12 pagesTAURINE The Key To Restoring Metabolic Function - Ray Peat ForumDarci Hall100% (1)
- Nutritional Surveillance ModuleDocument57 pagesNutritional Surveillance ModuleDwi Ayu Lestari100% (1)
- Balanced Diet For A Lactating MotherDocument30 pagesBalanced Diet For A Lactating MotherD. Melba S.S ChinnaNo ratings yet
- Annual Plan - Biology - Igcse Level-1 (2023-24)Document6 pagesAnnual Plan - Biology - Igcse Level-1 (2023-24)omanokello4No ratings yet
- Nutrition Throughout The Life CycleDocument87 pagesNutrition Throughout The Life Cyclealsuwaidi5No ratings yet
- Evion LC Q & A For E-MultiplierDocument2 pagesEvion LC Q & A For E-Multiplierknk761987No ratings yet
- Manila Police District (MPD) As of January 2022: Action PNCO, DSTU OIC, Training Section C, DPRMDDocument15 pagesManila Police District (MPD) As of January 2022: Action PNCO, DSTU OIC, Training Section C, DPRMDShan Dave TupasNo ratings yet
- Evidence-Based Interventions For Improving Maternal and Child NutritionDocument19 pagesEvidence-Based Interventions For Improving Maternal and Child Nutritionarc08No ratings yet
- Enfamil® Liquid Human Milk Fortifier High ProteinDocument13 pagesEnfamil® Liquid Human Milk Fortifier High ProteinMarioNo ratings yet
- What Is A Healthy Lifestyle?Document3 pagesWhat Is A Healthy Lifestyle?MahmutKolaNo ratings yet
- Soal 7Document10 pagesSoal 7aripin12011988No ratings yet
- Chapter 1 (DL JACKFRUIT) NEW 1Document5 pagesChapter 1 (DL JACKFRUIT) NEW 1Leane Enero DarayNo ratings yet