Sama Notes Upper Limb
Sama Notes Upper Limb
Download as pdf or txt
You might also like
- LionsatLunchtime PDFDocument24 pagesLionsatLunchtime PDFIvonne Marina EsteveNo ratings yet
- 2 ArthrologyDocument30 pages2 ArthrologyAbhijith S. PNo ratings yet
- Joint Cavity Is PresentDocument9 pagesJoint Cavity Is PresentAlen OsmanovicNo ratings yet
- JointsDocument27 pagesJointsVarsha Mol MohananNo ratings yet
- BONEDocument30 pagesBONEsillythings300No ratings yet
- 5 - ArthrologyDocument26 pages5 - Arthrologydrshubhamvyas.08No ratings yet
- JointsDocument22 pagesJointswazzupwaleedNo ratings yet
- The Infrapatellar Fat Pad in The KneeDocument10 pagesThe Infrapatellar Fat Pad in The KneeDeogracias S. Espiritu IINo ratings yet
- Field of Study Concerned With The Study of Joints .: ArthrologyDocument32 pagesField of Study Concerned With The Study of Joints .: Arthrologyزين العابدين محمد عويشNo ratings yet
- 7 October, 2021. Thursday Biology JointsDocument17 pages7 October, 2021. Thursday Biology JointsOyasor Ikhapo AnthonyNo ratings yet
- JOINTSDocument14 pagesJOINTSyohanap741No ratings yet
- Articular System 1 Transcript - 4Document4 pagesArticular System 1 Transcript - 4estellasr00No ratings yet
- Classificationofjoints 140413054157 Phpapp01 161023170805Document49 pagesClassificationofjoints 140413054157 Phpapp01 161023170805Adu-danquah StephenNo ratings yet
- Lecture 3 Cartilage, Muscle and Joints.Document49 pagesLecture 3 Cartilage, Muscle and Joints.usaeed00000No ratings yet
- Module 3 Anatomy I ArthrologyDocument12 pagesModule 3 Anatomy I ArthrologyneannaNo ratings yet
- Revision 1Document18 pagesRevision 1John MwengweNo ratings yet
- Anatomy Sendi WebDocument10 pagesAnatomy Sendi WebazimahakimNo ratings yet
- Anatomy, Joints - StatPearls - NCBI BookshelfDocument9 pagesAnatomy, Joints - StatPearls - NCBI BookshelfDave FisherNo ratings yet
- JointsffffDocument19 pagesJointsffffrv9v7r6fjjNo ratings yet
- JointsDocument54 pagesJointsmdmasuahmed786No ratings yet
- Marrow Produce Red Blood Cells, White Blood Cells, and Platelets, A Process CalledDocument4 pagesMarrow Produce Red Blood Cells, White Blood Cells, and Platelets, A Process CalledIlyasroisulfahmiNo ratings yet
- Art HR OlogyDocument42 pagesArt HR OlogyjovinkasimirNo ratings yet
- JointsDocument5 pagesJointsSEAN JODI M. COSEPENo ratings yet
- Metaphysis of The Long Bone. at The Long Bones, The Greatest Dimension Is The Length They Are SituatedDocument3 pagesMetaphysis of The Long Bone. at The Long Bones, The Greatest Dimension Is The Length They Are SituatedbarbacumlaudeNo ratings yet
- Anatomy of JointsDocument5 pagesAnatomy of JointsJayson CastroNo ratings yet
- Joints Lecture 1Document12 pagesJoints Lecture 1Ahmed MohamedNo ratings yet
- The 3 Types of Joints in The BodyDocument3 pagesThe 3 Types of Joints in The BodyLhyn Liam-LameraNo ratings yet
- Type of JointsDocument51 pagesType of JointsZainab AshroffNo ratings yet
- m5 Skeletal SystemDocument33 pagesm5 Skeletal Systemapi-464344582100% (1)
- JointsDocument21 pagesJointsyoga karsendaNo ratings yet
- 689general and Systems 2023 اسنان عامDocument36 pages689general and Systems 2023 اسنان عامking111newNo ratings yet
- Classification of Joints-Dr - GosaiDocument10 pagesClassification of Joints-Dr - GosaiDr.B.B.GosaiNo ratings yet
- Arthrology: DR N. ChikumbaDocument50 pagesArthrology: DR N. ChikumbaNatty ChikumbaNo ratings yet
- Anatomy, Joints - StatPearls - NCBI BookshelfDocument10 pagesAnatomy, Joints - StatPearls - NCBI BookshelfNirmalasari AnirNo ratings yet
- Art HR OlogyDocument67 pagesArt HR Ologyvalenzuelamc.numoaNo ratings yet
- JOINTSDocument39 pagesJOINTSAnushaNo ratings yet
- Lecture 4 (Joints)Document8 pagesLecture 4 (Joints)Άγγελος ΧαβέλαςNo ratings yet
- TYPES OF JOINTS_119c6416bbad51cfb147d2850adac20eDocument2 pagesTYPES OF JOINTS_119c6416bbad51cfb147d2850adac20ejingerlucieNo ratings yet
- Bones and JointsDocument15 pagesBones and JointsRegina AlcaideNo ratings yet
- College of Physical and Respiratory Therapy S.Y. 2016-2017: Bernardo Tayaban JR., PTRP Maverick Kaypee Colet, PTRPDocument7 pagesCollege of Physical and Respiratory Therapy S.Y. 2016-2017: Bernardo Tayaban JR., PTRP Maverick Kaypee Colet, PTRPVanessa Yvonne GurtizaNo ratings yet
- Joints NotesDocument2 pagesJoints NotesDeva ChiruNo ratings yet
- Anotomy AssignmentDocument11 pagesAnotomy Assignmentutube.id02No ratings yet
- Type of Joints: Group MembersDocument21 pagesType of Joints: Group MembersBeni Ram RawalNo ratings yet
- HumanDocument3 pagesHumanshifa nasrinNo ratings yet
- ARTHROLOGYDocument10 pagesARTHROLOGYAlina MoiseNo ratings yet
- 6 JointDocument11 pages6 Jointيزن الحارثيNo ratings yet
- Notes - Intro To JointsDocument3 pagesNotes - Intro To JointsbeanNo ratings yet
- Chapter 13 Ana LabDocument15 pagesChapter 13 Ana LabJyrus Quim CrusperoNo ratings yet
- Pna Midterm Prep: Joints Classification of Joints:: Synovial Cavity Connective Tissue Fibrous JointsDocument4 pagesPna Midterm Prep: Joints Classification of Joints:: Synovial Cavity Connective Tissue Fibrous JointsaamenaNo ratings yet
- 4.3 Bone TissueDocument80 pages4.3 Bone TissueManjunathNo ratings yet
- Musculoskeletal System L4Document39 pagesMusculoskeletal System L4BoazNo ratings yet
- Bones in The Body 1. Skull: Skeletal SystemDocument12 pagesBones in The Body 1. Skull: Skeletal SystemSolemnly SwearrNo ratings yet
- Arthrology by Dr. FarrukhDocument51 pagesArthrology by Dr. FarrukhFarrukh ShahzadNo ratings yet
- A. Interrupted/discontinuous JunctionsDocument5 pagesA. Interrupted/discontinuous JunctionsAlan TayNo ratings yet
- Lecture 9 - JointsDocument50 pagesLecture 9 - JointsberhanuNo ratings yet
- Introduction to the Anatomy (1)Document17 pagesIntroduction to the Anatomy (1)hmady62005No ratings yet
- Less Synd of The TrunkDocument39 pagesLess Synd of The TrunkcallmeowaiseeNo ratings yet
- Body JointsDocument28 pagesBody JointsAlban Presley R. SangmaNo ratings yet
- Joints 9.9.2021Document16 pagesJoints 9.9.202121120072No ratings yet
- Skeletal SystemDocument6 pagesSkeletal SystemAngel MoncadaNo ratings yet
- Encyclopaedia Britannica, 11th Edition, Volume 15, Slice 5 "Joints" to "Justinian I."From EverandEncyclopaedia Britannica, 11th Edition, Volume 15, Slice 5 "Joints" to "Justinian I."No ratings yet
- The Organizational Structure of UnileverDocument4 pagesThe Organizational Structure of UnileverTrang ĐoanNo ratings yet
- Ophthalmology Question BankDocument45 pagesOphthalmology Question BankVsmfhjn50% (2)
- Module 8 RationaleDocument3 pagesModule 8 RationaleG INo ratings yet
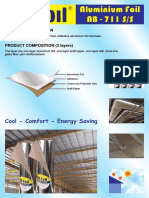
- Aluminium Foil AB - 711 S/S: Cool - Comfort - Energy SavingDocument2 pagesAluminium Foil AB - 711 S/S: Cool - Comfort - Energy SavingcandraNo ratings yet
- Static Transfer Switches - STS30Document2 pagesStatic Transfer Switches - STS30Mohan RajNo ratings yet
- Light, Sound and Hearing - ExercisesDocument11 pagesLight, Sound and Hearing - ExercisesLim Kok PingNo ratings yet
- Read The Following Passage and Mark The Letter A, B, C, or D On Your Answer Sheet To Indicate The Correct Answer To Each of The QuestionsDocument6 pagesRead The Following Passage and Mark The Letter A, B, C, or D On Your Answer Sheet To Indicate The Correct Answer To Each of The QuestionsThai Thi Hong LoanNo ratings yet
- Application Form Smaw NC IiDocument3 pagesApplication Form Smaw NC IiAlcantara CastilloNo ratings yet
- Paper Manufacturing Technology by VoithDocument76 pagesPaper Manufacturing Technology by VoithMarcWorldNo ratings yet
- MS 01 140Document68 pagesMS 01 140salalahNo ratings yet
- Developemental Disturbances of Oral and Paraoral TissuesDocument209 pagesDevelopemental Disturbances of Oral and Paraoral TissuesMailoud AlnaileNo ratings yet
- Wvs 730-2240 GBDocument8 pagesWvs 730-2240 GBSuministros Lago Suministros LagoNo ratings yet
- New - Brosur Bahasa Inggris - Ghana - NewDocument2 pagesNew - Brosur Bahasa Inggris - Ghana - NewGreen Leaf IndonesiaNo ratings yet
- Income Statement Problems With AnswersDocument6 pagesIncome Statement Problems With AnswerskoftaNo ratings yet
- Chemistry 1 - 11 - Q1 - M4Document14 pagesChemistry 1 - 11 - Q1 - M4Deez NutsNo ratings yet
- New Agriways PreviewDocument2 pagesNew Agriways Previewmohammadibraheem8620No ratings yet
- Department of Education: Republic of The PhilippinesDocument1 pageDepartment of Education: Republic of The PhilippinesJestoni SalvadorNo ratings yet
- Class 11 CH 3Document27 pagesClass 11 CH 3Dhruv AgarwalNo ratings yet
- Chip ResistorDocument61 pagesChip ResistorAli Raza100% (1)
- Avaliacao 3 AnoDocument3 pagesAvaliacao 3 AnoGeraldo AlmeidaNo ratings yet
- War On DrugsDocument18 pagesWar On DrugsMark Jessie Panopio Magsaysay100% (3)
- Espironolactona en DiálisisDocument11 pagesEspironolactona en DiálisisMaria Juliana ValenzuelaNo ratings yet
- Look Back in AngerDocument2 pagesLook Back in AngerBoniamin HossainNo ratings yet
- QUIZZ3Document3 pagesQUIZZ3FatimaNo ratings yet
- 7XG22 2RMLGDocument12 pages7XG22 2RMLGAshish JainNo ratings yet
- Class Presentation As 469288Document72 pagesClass Presentation As 469288Lawrence Kevin FrencillanoNo ratings yet
- Thomas Warren BurbankAirportDocument2 pagesThomas Warren BurbankAirporttpwarren23No ratings yet
- Mechanical SystemsDocument3 pagesMechanical SystemsonspsnonsNo ratings yet
- 41-51 Case DigestDocument8 pages41-51 Case DigestCarmela Paola R. DumlaoNo ratings yet