Prof. Dr. Dr. Rukiah Syawal, SPM (K)
Prof. Dr. Dr. Rukiah Syawal, SPM (K)
Download as ppt, pdf, or txt
You might also like
- MPO Assignment 1 (02000539)Document13 pagesMPO Assignment 1 (02000539)Aarkash Kannangara0% (1)
- Paused Rep Mastery: About The ProgramDocument3 pagesPaused Rep Mastery: About The ProgramDVM 700No ratings yet
- Uveitis Presentation Ridge HospitalDocument40 pagesUveitis Presentation Ridge Hospitalgideon A. owusuNo ratings yet
- Prof, DR, DR Rukiah Sawal SPM (K)Document37 pagesProf, DR, DR Rukiah Sawal SPM (K)inhaNo ratings yet
- UveeDocument38 pagesUveemihalceaNo ratings yet
- Refrat: Pembimbing: DR - Rahmad Syuhada SP.MDocument26 pagesRefrat: Pembimbing: DR - Rahmad Syuhada SP.MIzza TanzihulNo ratings yet
- Uveitis 2024Document13 pagesUveitis 2024Zahy ZahyNo ratings yet
- UveitisDocument10 pagesUveitisdykesu1806No ratings yet
- Feline UveitesDocument9 pagesFeline UveitesErick ConfickeerzNo ratings yet
- Optometry 355 12 Episcleritis ScleritisDocument67 pagesOptometry 355 12 Episcleritis ScleritisDavid NgNo ratings yet
- Pan Uveitis (Causes and MGT of Sympathetic Ophthalmitis)Document21 pagesPan Uveitis (Causes and MGT of Sympathetic Ophthalmitis)Edoga Chima EmmanuelNo ratings yet
- Prof, DR, DR Rukiah Sawal SPM (K)Document37 pagesProf, DR, DR Rukiah Sawal SPM (K)ULINo ratings yet
- Diseases of The Uveal Tract 09Document24 pagesDiseases of The Uveal Tract 09somebody_ma100% (7)
- Diseases of Uveal TractDocument62 pagesDiseases of Uveal TractIhsan HanifNo ratings yet
- Kuliah Uvea & Lensa InternasionalDocument183 pagesKuliah Uvea & Lensa InternasionalYusvina QrNo ratings yet
- Care of Clients With Sensory Problems Care of Clients With Sensory ProblemsDocument82 pagesCare of Clients With Sensory Problems Care of Clients With Sensory Problemssnpjavier100% (1)
- Diseases of The UveaDocument58 pagesDiseases of The Uveahenok biruk100% (1)
- The OrbitDocument38 pagesThe OrbitSarahNo ratings yet
- Ocular EmergenciesDocument4 pagesOcular EmergenciesJim Jose AntonyNo ratings yet
- Acute Anterior UveitisDocument3 pagesAcute Anterior UveitisnasibdinNo ratings yet
- Eye & ENTDocument12 pagesEye & ENTShandar SadafNo ratings yet
- Uveitis (Revised)Document60 pagesUveitis (Revised)chqxbqq56mNo ratings yet
- Kelainan Sel DarahDocument28 pagesKelainan Sel DarahAprilikkaearlyNo ratings yet
- Bilateral Endogenous Bacterial PanophthalmitisDocument5 pagesBilateral Endogenous Bacterial PanophthalmitisIgnasius HansNo ratings yet
- CURS 06 UveiteleDocument19 pagesCURS 06 Uveiteledennyyy175No ratings yet
- Anterior UveitisDocument65 pagesAnterior UveitisHardy vlogsNo ratings yet
- Uveitis PDFDocument17 pagesUveitis PDFkmiz85No ratings yet
- Mata KorneaDocument37 pagesMata KorneaRushdaNo ratings yet
- Prof, DR, DR Rukiah Sawal SPM (K)Document37 pagesProf, DR, DR Rukiah Sawal SPM (K)hfzNo ratings yet
- 15.10.10-Diseases of The Orbit (Pptminimizer)Document54 pages15.10.10-Diseases of The Orbit (Pptminimizer)Ronald Ariyanto Wiradirnata0% (1)
- Hipopion, Iridosiklitis, Iritis by MaulidaDocument24 pagesHipopion, Iridosiklitis, Iritis by MaulidaSirly NabiretaNo ratings yet
- Uveitis: Mshangila Barnabas MD, M.MedDocument28 pagesUveitis: Mshangila Barnabas MD, M.MedCharles AnthonyNo ratings yet
- PUK Vs Mooren Ulcer Presentasi FinalDocument35 pagesPUK Vs Mooren Ulcer Presentasi FinalRaissaNo ratings yet
- Care of The Patient With Anterior Uveitis: Quick Reference GuideDocument4 pagesCare of The Patient With Anterior Uveitis: Quick Reference GuideAkicaNo ratings yet
- Lecture On Anterior Uveitis NewDocument43 pagesLecture On Anterior Uveitis NewophthallnctNo ratings yet
- Uveitis EnglishDocument28 pagesUveitis EnglishGermanyNo ratings yet
- UveitisDocument28 pagesUveitisDr Arnav SaroyaNo ratings yet
- Kuliah InfeksiDocument88 pagesKuliah InfeksiuupupupNo ratings yet
- Diagnostic Considerations in Uveitis: AAO Reading Section 9Document43 pagesDiagnostic Considerations in Uveitis: AAO Reading Section 9evaNo ratings yet
- Modul 1Document23 pagesModul 1Niniek Iin FNo ratings yet
- Uvea (Hira fj'23)Document15 pagesUvea (Hira fj'23)Minahil ShahidNo ratings yet
- Okap Samson Uveitis PDFDocument12 pagesOkap Samson Uveitis PDFsharu4291No ratings yet
- OpthaDocument5 pagesOpthavarun2k6No ratings yet
- Ophthalmology 2Document9 pagesOphthalmology 2Cherry KolaNo ratings yet
- 14 - UveitisDocument4 pages14 - UveitisSpislgal PhilipNo ratings yet
- By: Amit Chandanshive F.Y.M.PHARM.: Guide: Mrs. Vijaya BhogaleDocument39 pagesBy: Amit Chandanshive F.Y.M.PHARM.: Guide: Mrs. Vijaya Bhogaleirfan fadilahNo ratings yet
- Uveitis: Preceptor: Dr. Rahmad Syuhada, SP.M Wulandari, S.Ked 17360077Document23 pagesUveitis: Preceptor: Dr. Rahmad Syuhada, SP.M Wulandari, S.Ked 17360077widya melianitaNo ratings yet
- Iritis 8Document14 pagesIritis 8Alvis KurniawanNo ratings yet
- Acc or Inti 2007Document6 pagesAcc or Inti 2007iwanNo ratings yet
- 2021-Conrady Et Al-Ocular Drug Delivery For Uveitis Pharmaceutics-13-01224-V2Document17 pages2021-Conrady Et Al-Ocular Drug Delivery For Uveitis Pharmaceutics-13-01224-V2Richard GabrielNo ratings yet
- Diseases of The ConjunctivaDocument80 pagesDiseases of The ConjunctivaRatu CarissaNo ratings yet
- Atypical Case of Presumed Ocular Tuberculosis Presenting As Unilateral Occlusive VasculitisDocument4 pagesAtypical Case of Presumed Ocular Tuberculosis Presenting As Unilateral Occlusive VasculitisInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Mata Merah Visus TurunDocument27 pagesMata Merah Visus TurunErinNo ratings yet
- Neuritis OptikusDocument23 pagesNeuritis Optikusjanty100% (1)
- Prepared by Getenet Shumet (BSC, MSC Student)Document64 pagesPrepared by Getenet Shumet (BSC, MSC Student)Getenet shumetNo ratings yet
- Uveitis 4th Year-1Document38 pagesUveitis 4th Year-1mbbs-20-13-056No ratings yet
- Uveitis 4th Year-1Document38 pagesUveitis 4th Year-1mbbs-20-13-056No ratings yet
- Uveitis: Winarto Sub Depart. of E.E.DDocument122 pagesUveitis: Winarto Sub Depart. of E.E.Dtesha kurniaNo ratings yet
- Graves 508Document6 pagesGraves 508VellaNo ratings yet
- Microbialkeratitisbhatti 160607231414Document56 pagesMicrobialkeratitisbhatti 160607231414RanveerNo ratings yet
- Acute Necrotizing Panophthalmitis in Seropositive Case of ChikungunyaDocument3 pagesAcute Necrotizing Panophthalmitis in Seropositive Case of ChikungunyaPratyushNo ratings yet
- Complications in UveitisFrom EverandComplications in UveitisFrancesco PichiNo ratings yet
- Treatment of Asymptomatic Hyperuricemia in Chronic Kidney DiseaseDocument4 pagesTreatment of Asymptomatic Hyperuricemia in Chronic Kidney DiseaseRonald Ariyanto WiradirnataNo ratings yet
- NIFLECDocument6 pagesNIFLECRonald Ariyanto WiradirnataNo ratings yet
- From Happy or Silent Hypoxemia To Acute Respiratory Syndrome in Covid 19 DiseaseDocument13 pagesFrom Happy or Silent Hypoxemia To Acute Respiratory Syndrome in Covid 19 DiseaseRonald Ariyanto WiradirnataNo ratings yet
- Fluid Resuscitation in SepsisDocument68 pagesFluid Resuscitation in SepsisRonald Ariyanto WiradirnataNo ratings yet
- 15.10.10-Diseases of The Orbit (Pptminimizer)Document54 pages15.10.10-Diseases of The Orbit (Pptminimizer)Ronald Ariyanto Wiradirnata0% (1)
- 13.10.10-Eyelid and Adnexal Disease 2, PPT Presentasi 23 Okt 2009Document51 pages13.10.10-Eyelid and Adnexal Disease 2, PPT Presentasi 23 Okt 2009Ronald Ariyanto Wiradirnata0% (1)
- Gofamint 3rd & 4th Quarters ManualsDocument115 pagesGofamint 3rd & 4th Quarters ManualsVictor AndyNo ratings yet
- Microsoft Visual Studio: An Integrated Windows Program Development EnvironmentDocument16 pagesMicrosoft Visual Studio: An Integrated Windows Program Development Environmentakirank1No ratings yet
- Chapter 13 IntaccDocument2 pagesChapter 13 IntaccJhuliane RalphNo ratings yet
- Manufacturing Step in Ginger Oil ProcessingDocument3 pagesManufacturing Step in Ginger Oil ProcessingmilindNo ratings yet
- GardeningDocument18 pagesGardeningAman shrivasNo ratings yet
- Course Guide or L 2013Document6 pagesCourse Guide or L 2013Asebaho BadrNo ratings yet
- Transformer Stations and Renewable Energy Equipment Res 2023Document72 pagesTransformer Stations and Renewable Energy Equipment Res 2023delmarlauranNo ratings yet
- Scientific Notation Project Extra CreditDocument4 pagesScientific Notation Project Extra CreditEman MohamedNo ratings yet
- Pekka Ervast-The Esoteric School of JesusDocument168 pagesPekka Ervast-The Esoteric School of JesusIG100% (2)
- Unit 7. Revision and ConclusionDocument5 pagesUnit 7. Revision and ConclusionAryla AdhiraNo ratings yet
- ULANGAN HARIAN INVITATION SeleseDocument6 pagesULANGAN HARIAN INVITATION SeleseJunior HamdanNo ratings yet
- Complete Lab ReportDocument16 pagesComplete Lab ReportAdlina SafuraNo ratings yet
- Newspaper TemplateDocument2 pagesNewspaper TemplateAndrew TavaresNo ratings yet
- Case Study: Mortgauge Loan Lending Process in BlockchainDocument5 pagesCase Study: Mortgauge Loan Lending Process in BlockchainRahul Desai100% (1)
- PPC Semiotic TheoryDocument17 pagesPPC Semiotic TheoryBEATphNo ratings yet
- 5: Spoon FeedingDocument2 pages5: Spoon FeedingM.SHOURYA VARDHANNo ratings yet
- KARAN KHODE RESUME E4yearsDocument2 pagesKARAN KHODE RESUME E4yearswooden makersNo ratings yet
- Buku Siswa 1Document6 pagesBuku Siswa 1srikhairunnisaNo ratings yet
- 21 00202 Proposed Construction of Basketball Court Roofing at Bugallon PlazaDocument84 pages21 00202 Proposed Construction of Basketball Court Roofing at Bugallon PlazaJN CNo ratings yet
- Chapter 3 Costing Methods The Costing of Resource Output 2015Document21 pagesChapter 3 Costing Methods The Costing of Resource Output 2015Amha SeyoumNo ratings yet
- Eng11 Q1 Mod1 Dimensionsofphilliteraryhistory v1Document14 pagesEng11 Q1 Mod1 Dimensionsofphilliteraryhistory v1Jonathan Olegario60% (5)
- Internship Report: Vidyalaxmi Group of InstitutionDocument19 pagesInternship Report: Vidyalaxmi Group of InstitutionRashmitha Bhandary100% (1)
- Lung Gom Pa RunnersDocument6 pagesLung Gom Pa RunnersJohnette Ricchetti50% (4)
- ChanakyaDocument24 pagesChanakyahotrev86No ratings yet
- Metropolitan Bank and Trust Company Vs Ba FinanceDocument1 pageMetropolitan Bank and Trust Company Vs Ba FinanceJENNY BUTACANNo ratings yet
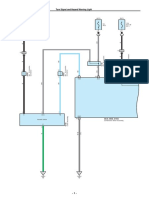
- Turn Signal and Hazard Warning Light: (BAT) (ACC) (BAT)Document6 pagesTurn Signal and Hazard Warning Light: (BAT) (ACC) (BAT)CLC 18C4No ratings yet
- Threshold 14Document192 pagesThreshold 14Vikshade100% (4)
- Tristan TaorminoDocument252 pagesTristan Taorminomaquis870% (1)