Psoriasis & Psoriatic Arthritis: DR Prathibha J P
Psoriasis & Psoriatic Arthritis: DR Prathibha J P
Download as pptx, pdf, or txt
You might also like
- DOCU - MedA Charting GuidelinesDocument3 pagesDOCU - MedA Charting GuidelinesTee Wood50% (2)
- Liver CancerDocument8 pagesLiver CancerAlyssa Marie PepitoNo ratings yet
- Radiology Pediatric Bone TumorsDocument69 pagesRadiology Pediatric Bone Tumorsdrqazi777No ratings yet
- Total Hip Arthroplasty 243Document40 pagesTotal Hip Arthroplasty 243jefferyNo ratings yet
- Acute Appendicitis in Pediatric PatientsDocument16 pagesAcute Appendicitis in Pediatric PatientsIgnatius Rheza SetiawanNo ratings yet
- Skin Problems in RheumatologyDocument52 pagesSkin Problems in RheumatologyAyi Abdul BasithNo ratings yet
- 5 Psoriasis PDFDocument76 pages5 Psoriasis PDFWorku KifleNo ratings yet
- PsoriasisDocument54 pagesPsoriasisPriya GKNo ratings yet
- Presentation 1Document57 pagesPresentation 1Brian BeeNo ratings yet
- PsoriasisDocument32 pagesPsoriasisChirag VijayvargiyaNo ratings yet
- Skin Block: - Introduction To Diseases of The Skin - Acneiform, Alopecias, and Pigmentary DisordersDocument60 pagesSkin Block: - Introduction To Diseases of The Skin - Acneiform, Alopecias, and Pigmentary DisordershemihemaNo ratings yet
- The Rheumatological Exam: R Kadanoff M.D Loyola University Medical CenterDocument16 pagesThe Rheumatological Exam: R Kadanoff M.D Loyola University Medical CenterSherief MansourNo ratings yet
- Papulosquamous Diseases (Andrew's Dermatology)Document10 pagesPapulosquamous Diseases (Andrew's Dermatology)Xanthia CristobalNo ratings yet
- White Scaly Papules and Plaques On His Elbows, Extensor Arms, Knees, and ShinsDocument54 pagesWhite Scaly Papules and Plaques On His Elbows, Extensor Arms, Knees, and ShinsJohn Christopher LucesNo ratings yet
- Dermatology: Minci YazuminDocument48 pagesDermatology: Minci Yazuminminci senseiNo ratings yet
- CBT Ortho 1Document45 pagesCBT Ortho 1putri umepalNo ratings yet
- Psoriasis, Insect BitingDocument134 pagesPsoriasis, Insect Bitinggupta.keshav4385No ratings yet
- Seronegative-SpondyloarthropathiesDocument46 pagesSeronegative-SpondyloarthropathiesLaiba FatimaNo ratings yet
- JointsDocument43 pagesJointskamaluNo ratings yet
- Papulosquamous DisordersDocument51 pagesPapulosquamous DisordersleenaloveuNo ratings yet
- Approach To Joint PainDocument44 pagesApproach To Joint PainKavya Anoop100% (1)
- 106 - Arthritis - ELDocument92 pages106 - Arthritis - ELNick-Hugh WisdomNo ratings yet
- (K25) Path - Musculosceletal FK Part 2Document69 pages(K25) Path - Musculosceletal FK Part 2Virginia JawaNo ratings yet
- PsoriasisDocument36 pagesPsoriasisMiva AdhiamboNo ratings yet
- Rheumatology NotesDocument31 pagesRheumatology Noteskatherine nunnNo ratings yet
- Psoriasis Lecture Notes 2015Document17 pagesPsoriasis Lecture Notes 2015SaulNo ratings yet
- Orthopedic Infections, Osteomyelitis:Septic ArthritisDocument65 pagesOrthopedic Infections, Osteomyelitis:Septic ArthritisnhfbyqvgwhNo ratings yet
- Laporan Kasus Psoriasis: Disusun Oleh: Yusuf, S.Ked 201110401011016 Pembimbing: Dr. Firdausi N, SP - KKDocument39 pagesLaporan Kasus Psoriasis: Disusun Oleh: Yusuf, S.Ked 201110401011016 Pembimbing: Dr. Firdausi N, SP - KKGalihNo ratings yet
- Arthritis of The ForefootDocument54 pagesArthritis of The ForefootMax DocNo ratings yet
- Rheumatology Year 4Document90 pagesRheumatology Year 4Abdalla SamatarNo ratings yet
- PsoriasisDocument25 pagesPsoriasisTutor VirusNo ratings yet
- PsoriasisDocument30 pagesPsoriasisAbdul BasitNo ratings yet
- Papulosquamous Ds.Document70 pagesPapulosquamous Ds.CHALIE MEQU100% (1)
- Pathology Outlines - PsoriasisDocument1 pagePathology Outlines - PsoriasisCaryl DagamiNo ratings yet
- Joint PainDocument11 pagesJoint PainSandarekha PereraNo ratings yet
- Bone andDocument33 pagesBone andSuci MayveraNo ratings yet
- MSK Lecture 1-1Document53 pagesMSK Lecture 1-1seemabfarwauaeNo ratings yet
- SclerodermaDocument20 pagesSclerodermariskaicung100% (1)
- Rheumatology NotesDocument10 pagesRheumatology NotesBrandonRyanF.MosidinNo ratings yet
- Approach To Joint Pain-1Document49 pagesApproach To Joint Pain-1Shivangi LodhaNo ratings yet
- Psoriasis: For Health Officer Students Solomon H (MD, DVR)Document38 pagesPsoriasis: For Health Officer Students Solomon H (MD, DVR)Theo Grazila Ruva100% (1)
- PsoriasisDocument57 pagesPsoriasishometechonoNo ratings yet
- Oral Maxillofacial Pathology NotesDocument18 pagesOral Maxillofacial Pathology NotesJose TeeNo ratings yet
- Diabetic Foot Ulcer: DR Surein PrasadDocument43 pagesDiabetic Foot Ulcer: DR Surein PrasadNinaNo ratings yet
- Connective Tissue Diseases: Edward D. Buckingham, MD Byron J. Bailey, MDDocument88 pagesConnective Tissue Diseases: Edward D. Buckingham, MD Byron J. Bailey, MDcafemedNo ratings yet
- PsoriasisDocument27 pagesPsoriasisMishaNo ratings yet
- Medical ConditionDocument126 pagesMedical ConditionKayeNo ratings yet
- Osteomyelitis: Pediatric Surgery Department Andreev D.ADocument83 pagesOsteomyelitis: Pediatric Surgery Department Andreev D.AlimeddyNo ratings yet
- Rheumatology: Osteoarthritis Rheumatoid Arthritis: Dr. Meg-Angela Christi AmoresDocument25 pagesRheumatology: Osteoarthritis Rheumatoid Arthritis: Dr. Meg-Angela Christi AmoresNinaNo ratings yet
- NEBRAS RheumatologyDocument129 pagesNEBRAS Rheumatologyclang83No ratings yet
- AIR FlimDocument69 pagesAIR FlimRapid MedicineNo ratings yet
- Skenario A Blok 19Document9 pagesSkenario A Blok 19anonymousNo ratings yet
- Psoriasis Clinical FeaturesDocument37 pagesPsoriasis Clinical FeaturesVartika RatanNo ratings yet
- Skin and Systemic DiseasesDocument19 pagesSkin and Systemic DiseasesEman FatimaNo ratings yet
- 2 - 3.cutaneous Manifestation ofDocument31 pages2 - 3.cutaneous Manifestation ofdocanipaNo ratings yet
- PsoriasisDocument32 pagesPsoriasisEffah FestusNo ratings yet
- Oral Maxillofacial PathologyDocument18 pagesOral Maxillofacial Pathologyashleylaa05100% (10)
- Acute Septic Arthritis and OsteomyelitisDocument44 pagesAcute Septic Arthritis and OsteomyelitisAmr HassanNo ratings yet
- Physical Assessment As Screening ToolDocument35 pagesPhysical Assessment As Screening ToolKieran LeviNo ratings yet
- C.T DisDocument40 pagesC.T DisalhussaintariqNo ratings yet
- Approach To Acute Arthritis in Kids: Allyson Mcdonough, MD Baylor Scott & White Health Department of RheumatologyDocument35 pagesApproach To Acute Arthritis in Kids: Allyson Mcdonough, MD Baylor Scott & White Health Department of Rheumatologyromeoenny4154No ratings yet
- Approach To Arthritis PatientDocument20 pagesApproach To Arthritis Patientapi-3716867No ratings yet
- List of All The Railway Stations Between Bangalore and ChennaiDocument3 pagesList of All The Railway Stations Between Bangalore and ChennaijefferyNo ratings yet
- Little Deer and The Tra1Document5 pagesLittle Deer and The Tra1jefferyNo ratings yet
- Assignment of HypertensionDocument28 pagesAssignment of HypertensionjefferyNo ratings yet
- PDF To WordDocument193 pagesPDF To Wordjeffery0% (1)
- Coronary Circulation FDocument36 pagesCoronary Circulation FjefferyNo ratings yet
- Rajiv Gandhi University of Health Sciences, Karnataka: Registration No.Document2 pagesRajiv Gandhi University of Health Sciences, Karnataka: Registration No.jefferyNo ratings yet
- Cardiopulmonary ResuscitationDocument21 pagesCardiopulmonary ResuscitationjefferyNo ratings yet
- Thermotherapy: by Brillya BhaskarDocument16 pagesThermotherapy: by Brillya BhaskarjefferyNo ratings yet
- 4th To 8th WeekDocument48 pages4th To 8th WeekjefferyNo ratings yet
- Congenital Heart Disease (CHD)Document89 pagesCongenital Heart Disease (CHD)jefferyNo ratings yet
- 0 - Cervical Spine Assessment-1Document48 pages0 - Cervical Spine Assessment-1jeffery100% (1)
- FNP Predictor Study 64 Complete Questions and Answers Graded ADocument12 pagesFNP Predictor Study 64 Complete Questions and Answers Graded Aobitajoy06No ratings yet
- Infection Basics: Biology 4310 Virology Spring 2020Document49 pagesInfection Basics: Biology 4310 Virology Spring 2020Robin SinghNo ratings yet
- 4.daftar Pustaka Artikel BagusDocument5 pages4.daftar Pustaka Artikel BagusJono ParmiNo ratings yet
- Oncology, Palliative Geriatric NursingDocument6 pagesOncology, Palliative Geriatric Nursingminoshipeiris28No ratings yet
- Bullets CDDocument2 pagesBullets CDJonas Marvin AnaqueNo ratings yet
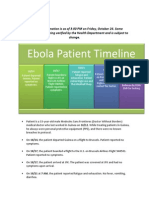
- DOHMH Patient Timeline 10-24-14Document3 pagesDOHMH Patient Timeline 10-24-14ahawkins8223No ratings yet
- Hemiplegic MigraineDocument2 pagesHemiplegic MigrainegungdeNo ratings yet
- NON-ALCOHOLIC FATTY LIVEr DISEASE (NAFLD) - NASHDocument4 pagesNON-ALCOHOLIC FATTY LIVEr DISEASE (NAFLD) - NASHJason FooNo ratings yet
- 5 Paragraph Expository Essay OutlineDocument3 pages5 Paragraph Expository Essay Outlineb71bpjha100% (2)
- Health and Travel Alert Updated Travel RequirementsDocument3 pagesHealth and Travel Alert Updated Travel RequirementsShani Mur.No ratings yet
- Bibliography About The Effectiveness of COVID-19 Preventive Measures in Luzon, PhilippinesDocument5 pagesBibliography About The Effectiveness of COVID-19 Preventive Measures in Luzon, PhilippinesIVAN LUIS MARTINEZNo ratings yet
- Puppy Vaccination ScheduleDocument2 pagesPuppy Vaccination ScheduleCecilia SanchezNo ratings yet
- WHO Health DefinitionDocument36 pagesWHO Health Definitionhinakaminari100% (1)
- Afp Surveillance 21st Century 0Document25 pagesAfp Surveillance 21st Century 0cavmichaelNo ratings yet
- Ho CocDocument48 pagesHo Cocmehadi100% (1)
- The Prevalence of Metabolic Syndrome in Latin AmerDocument13 pagesThe Prevalence of Metabolic Syndrome in Latin AmercarolinaNo ratings yet
- Lupus Nephritis1Document45 pagesLupus Nephritis1Lingga Gumelar100% (1)
- Levels of PreventionDocument23 pagesLevels of Preventionkuruvagadda sagar100% (1)
- Definición de La DepresiónDocument7 pagesDefinición de La Depresiónewacyp4f100% (1)
- Nursing Care Process Assessment Nursing Diagnosis ObjectiveDocument6 pagesNursing Care Process Assessment Nursing Diagnosis ObjectiveKMNo ratings yet
- The Issue The Speaker's Stand The Problem The Proposed SolutionDocument2 pagesThe Issue The Speaker's Stand The Problem The Proposed SolutionJuan Jaylou AnteNo ratings yet
- Dialogue About TuberculosisDocument2 pagesDialogue About TuberculosisPutri WidiasihNo ratings yet
- MEDTEST04062024 KannadaDocument24 pagesMEDTEST04062024 Kannadakushalhr162005No ratings yet
- Acute Disseminated Encephalomyelitis After Rabies Vaccination: One Case ReportDocument4 pagesAcute Disseminated Encephalomyelitis After Rabies Vaccination: One Case ReportIJAR JOURNALNo ratings yet
- DiabeticRetPPP2014 SummaryBenchmarkPagesDocument2 pagesDiabeticRetPPP2014 SummaryBenchmarkPageskomite medikNo ratings yet
- Summaries of Medically Important Fungi: Fungi Causing Cutaneous & Subcutaneous Mycoses (CHAPTER 48)Document3 pagesSummaries of Medically Important Fungi: Fungi Causing Cutaneous & Subcutaneous Mycoses (CHAPTER 48)Rana SabNo ratings yet
- CHN - Case Study No. 2 Marco Ray VelaDocument5 pagesCHN - Case Study No. 2 Marco Ray VelaMarco VelaNo ratings yet