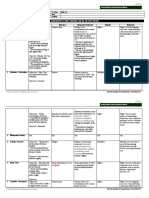
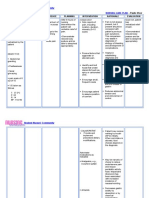
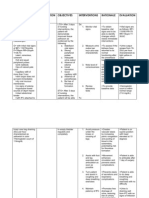
NCP 1
NCP 1
Download as pptx, pdf, or txt
You might also like
- Gordon's Bisaya VersionDocument2 pagesGordon's Bisaya VersionDanielle Valerie100% (1)
- The Katipunan and The Revolution: Memoirs of A General The Revolt of The Masses: The Story of Bonifacio and The KatipunanDocument11 pagesThe Katipunan and The Revolution: Memoirs of A General The Revolt of The Masses: The Story of Bonifacio and The KatipunanNestor Cabacungan100% (1)
- SP CSDocument4 pagesSP CSKhan HansNo ratings yet
- NCP Post Op PainDocument2 pagesNCP Post Op PainLiz Liwag0% (1)
- Gouty Arthritis-NcpDocument2 pagesGouty Arthritis-NcpJohn D100% (2)
- NCP EsrdDocument2 pagesNCP EsrdAziil LiizaNo ratings yet
- 4 Ways of Looking at ARTDocument1 page4 Ways of Looking at ARTAlexBobNo ratings yet
- 9a Gordon English and Filipino Version 2 PDFDocument8 pages9a Gordon English and Filipino Version 2 PDFAJ Imperial100% (1)
- NCP-Risk For InfectionDocument2 pagesNCP-Risk For InfectionJea Joel Mendoza100% (1)
- Tony Stark NCPDocument2 pagesTony Stark NCPNoha Jihan Nsouli100% (1)
- Physical AssessmentDocument8 pagesPhysical Assessmentjanelee2824No ratings yet
- Drug Study EditedDocument5 pagesDrug Study EditedfabtaciousVeelaNo ratings yet
- NCP and Fdar Wk2 Sarscov-19Document4 pagesNCP and Fdar Wk2 Sarscov-19Jamaica Malicdem0% (1)
- Cues Nursing Diagnosis Goals and Objectives Nursing Interventions Rationale Evaluation IndependentDocument3 pagesCues Nursing Diagnosis Goals and Objectives Nursing Interventions Rationale Evaluation Independentghelle183% (6)
- CBG RetdemDocument7 pagesCBG Retdemadd.bdrcNo ratings yet
- Teaching PlanDocument4 pagesTeaching PlanPagodNo ratings yet
- Peptic UlcerDocument3 pagesPeptic Ulcerdanica100% (1)
- Basic Interventions To Maintain Healthy LifestyleDocument13 pagesBasic Interventions To Maintain Healthy Lifestylehahahahaaaaaaa0% (1)
- Nursing Care Plan Assessment Nursing Diagnosis Background Knowledge Goal and Objectives Nursing Intervention and Rationale EvaluationDocument23 pagesNursing Care Plan Assessment Nursing Diagnosis Background Knowledge Goal and Objectives Nursing Intervention and Rationale EvaluationyusivileidyNo ratings yet
- NCP For Chronic PainDocument11 pagesNCP For Chronic PainRYAN SAPLADNo ratings yet
- Health Teaching PlanDocument7 pagesHealth Teaching PlanchloeNo ratings yet
- AppendectomyDocument4 pagesAppendectomyKyre LandinginNo ratings yet
- Nicu NCP (Neo - Pnia)Document3 pagesNicu NCP (Neo - Pnia)lorence_cachoNo ratings yet
- Functional Health PatternDocument3 pagesFunctional Health PatternGladys Pasaporte100% (1)
- NCP (Orif)Document13 pagesNCP (Orif)Jay Jay JayyiNo ratings yet
- Health Teaching Plan For DengueDocument8 pagesHealth Teaching Plan For DengueMae VisperasNo ratings yet
- Sleep Related Problems (GROUP 2)Document3 pagesSleep Related Problems (GROUP 2)april hortilanoNo ratings yet
- NCPDocument11 pagesNCPJaziel Remo100% (1)
- Nursing Care Plan Peptic UlcerDocument3 pagesNursing Care Plan Peptic UlcerJefferson Baluyot PalmaNo ratings yet
- IMCI Learning FeedbackDocument1 pageIMCI Learning Feedbackinah krizia lagueNo ratings yet
- Bioethics 3.02 Cooperation - Dr. QuinonesDocument2 pagesBioethics 3.02 Cooperation - Dr. QuinonesJennifer Pisco LiracNo ratings yet
- NCP - Ineffective Airway ClearanceDocument2 pagesNCP - Ineffective Airway ClearanceRosalie DelfinNo ratings yet
- Physical Assessment For Dengue..Document12 pagesPhysical Assessment For Dengue..Noeclaire Jamandre TulodNo ratings yet
- Concept Map - MumpsDocument4 pagesConcept Map - MumpsElleNo ratings yet
- Migraine NCPDocument5 pagesMigraine NCPJohn Dexter FranciscoNo ratings yet
- Impaired Tissue Integrity - Nursing Diagnosis & Care Plan PDFDocument15 pagesImpaired Tissue Integrity - Nursing Diagnosis & Care Plan PDFManar AbdallahNo ratings yet
- HTP FinalDocument3 pagesHTP Finalאורזלין לנזוןNo ratings yet
- NCP H MoleDocument5 pagesNCP H MoleJoule PeirreNo ratings yet
- Diarrhea (AGE)Document2 pagesDiarrhea (AGE)NursesLabs.com100% (1)
- Dengue Gordons OnlyDocument5 pagesDengue Gordons OnlyKelvin Pantaleon Ramasta100% (1)
- Chapter 11 Health EducationDocument12 pagesChapter 11 Health EducationJapaanNo ratings yet
- Cues Nursing Diagnosis Rationale Planning Nursing Intervention Rationale EvaluationDocument2 pagesCues Nursing Diagnosis Rationale Planning Nursing Intervention Rationale EvaluationErika Mae MananganNo ratings yet
- NCPDocument10 pagesNCPbabycheska08No ratings yet
- Assessment Diagnosis Planning Implementatio N Rationale Evaluation Short Term: Indipendent Short TermDocument2 pagesAssessment Diagnosis Planning Implementatio N Rationale Evaluation Short Term: Indipendent Short TermKenneth PoncialNo ratings yet
- Assessment Diagnosis Inference Planning Intervention Rationale EvaluationDocument2 pagesAssessment Diagnosis Inference Planning Intervention Rationale EvaluationMr. whiteNo ratings yet
- NCP For HemorrhoidsDocument3 pagesNCP For HemorrhoidsTADURAN RENE MAE ANGELLI F.No ratings yet
- Final Na PaDocument54 pagesFinal Na PaShiara Ruth EdrosoloNo ratings yet
- NCP Proper TahbsoDocument3 pagesNCP Proper TahbsoMiriam EstradaNo ratings yet
- Assignment 3 Chapter 10Document5 pagesAssignment 3 Chapter 10Emma Tangonan0% (2)
- Drug Study PonstanDocument1 pageDrug Study PonstanRainier IbarretaNo ratings yet
- NCP Acute PainDocument3 pagesNCP Acute PainAlex MarieNo ratings yet
- Gensurvey SJMCDocument2 pagesGensurvey SJMCMariKeith AcostaNo ratings yet
- Abdominal PainDocument3 pagesAbdominal PainReiciel Joy Gombio100% (2)
- Assessing AbdomenDocument1 pageAssessing AbdomenKeesha Mae Urgelles TimogNo ratings yet
- Gordon's Functional Health PatternsDocument2 pagesGordon's Functional Health Patternsserarrist100% (2)
- Nursingcrib Com NURSING CARE PLAN Spontaneous AbortionDocument2 pagesNursingcrib Com NURSING CARE PLAN Spontaneous AbortionMina RacadioNo ratings yet
- DDSTDocument61 pagesDDSTji pay0% (1)
- GitDocument302 pagesGitjgcriste100% (7)
- Gastro HistoryDocument4 pagesGastro HistoryAsma SikanderNo ratings yet
- Unlocking the Secrets of Abdominal Pain: The Art of History Taking by Dr. Lana Al-SabeDocument43 pagesUnlocking the Secrets of Abdominal Pain: The Art of History Taking by Dr. Lana Al-SabeDr. Lana Al-SabeNo ratings yet
- POLON, THAGREED BSN3D - KIDNEY DISORDERSDocument4 pagesPOLON, THAGREED BSN3D - KIDNEY DISORDERSThagreed PolonNo ratings yet
- GI Signs and SymptomsDocument40 pagesGI Signs and SymptomsJohnny BeeNo ratings yet
- Concepts of FunctionDocument30 pagesConcepts of FunctionNestor CabacunganNo ratings yet
- TCWD MidtermDocument21 pagesTCWD MidtermNestor Cabacungan100% (1)
- Lesson 7 Asian RegionalismDocument15 pagesLesson 7 Asian RegionalismNestor CabacunganNo ratings yet
- Lesson 6 - Global Divides The North-SouthDocument25 pagesLesson 6 - Global Divides The North-SouthNestor CabacunganNo ratings yet
- Vaginal Delivery DischargeDocument3 pagesVaginal Delivery DischargeNestor CabacunganNo ratings yet
- Care of AdolescentDocument32 pagesCare of AdolescentNestor Cabacungan100% (2)
- Lesson 8 Global Media CulturesDocument14 pagesLesson 8 Global Media CulturesNestor CabacunganNo ratings yet
- NCMA 219 RLE Course Practicum Unit 1Document3 pagesNCMA 219 RLE Course Practicum Unit 1Nestor Cabacungan100% (1)
- Natural LawDocument20 pagesNatural LawNestor CabacunganNo ratings yet
- The Pre-Hispanic Barangay GovernmentDocument5 pagesThe Pre-Hispanic Barangay GovernmentNestor CabacunganNo ratings yet
- The Katipunan and The Revolution: Memoirs of A General The Revolt of The Masses: The Story of Bonifacio and The KatipunanDocument11 pagesThe Katipunan and The Revolution: Memoirs of A General The Revolt of The Masses: The Story of Bonifacio and The KatipunanNestor Cabacungan0% (1)
- T Is A Document Written by Their SelvesDocument1 pageT Is A Document Written by Their SelvesNestor CabacunganNo ratings yet
- Introduction To Community Health NursingDocument54 pagesIntroduction To Community Health NursingNestor CabacunganNo ratings yet
- Initial Data Base 1Document4 pagesInitial Data Base 1Nestor CabacunganNo ratings yet
- Case Study1Document1 pageCase Study1Nestor CabacunganNo ratings yet
- Course TaskDocument1 pageCourse TaskNestor CabacunganNo ratings yet
- UoM Projectformat BSCITDocument27 pagesUoM Projectformat BSCITMathana SumanNo ratings yet
- Data Sheet TB 06A: Single-Seated Micro-Fl Ow Valve DIN-VersionDocument8 pagesData Sheet TB 06A: Single-Seated Micro-Fl Ow Valve DIN-VersionIgor NircaNo ratings yet
- WIDELINE Timber Entry Frames Standard SizeDocument1 pageWIDELINE Timber Entry Frames Standard SizeManasi SatbhaiNo ratings yet
- Best Quiet Dehumidifier For Basement Apartment - DeyeDocument4 pagesBest Quiet Dehumidifier For Basement Apartment - DeyeMtek Solar energyNo ratings yet
- ĐỀ ĐỀ XUẤT DHBB ANH 10Document17 pagesĐỀ ĐỀ XUẤT DHBB ANH 10jamNo ratings yet
- H8 539 ExtendedDocument916 pagesH8 539 ExtendedNixon Maldonado100% (1)
- ISSN: 2471-6774: Juniper Publishers Juniper Journals 3700 Park View LN #12B, Irvine, California 92612, USADocument37 pagesISSN: 2471-6774: Juniper Publishers Juniper Journals 3700 Park View LN #12B, Irvine, California 92612, USAsamuel gemedaNo ratings yet
- MRT Rom Programmer 3Document8 pagesMRT Rom Programmer 3Sergio OrtegaNo ratings yet
- NIPONGGODocument15 pagesNIPONGGOCaracciolo CulinaryNo ratings yet
- SYD110GF DatasheetsDocument6 pagesSYD110GF Datasheetsedinson loboNo ratings yet
- Dot Net Interview QuestionDocument143 pagesDot Net Interview QuestionBlack JackNo ratings yet
- Criminology Board Exam Reviewer: EvidenceDocument7 pagesCriminology Board Exam Reviewer: EvidenceAbra RabacNo ratings yet
- Woman and Adbusters Revision BookletDocument27 pagesWoman and Adbusters Revision Bookletapi-620007552No ratings yet
- The AceDocument9 pagesThe Aceeugen66No ratings yet
- Tiger. Quentin Trollip PDFDocument22 pagesTiger. Quentin Trollip PDFrodrigo barraza100% (2)
- Caldina ECUDocument4 pagesCaldina ECUYudi Maulidiansyah100% (1)
- Google Advanced Data AnalyticsDocument1 pageGoogle Advanced Data AnalyticsTalha KhanNo ratings yet
- How To Understand Sri KrishnaDocument3 pagesHow To Understand Sri KrishnaKumar Ayeshwar ReangNo ratings yet
- Button' Reimagines F. Scott Fitzgerald: Film Uses Fresh Canvas To Capture Writer's MagicDocument2 pagesButton' Reimagines F. Scott Fitzgerald: Film Uses Fresh Canvas To Capture Writer's MagicSantiago WoollandsNo ratings yet
- NTUDA EBODE-Tire - A - Part - MelangesDocument27 pagesNTUDA EBODE-Tire - A - Part - MelangesStéphane KENDJO TCHOUMBONo ratings yet
- Analysis For Fault Detection of Vector-Controlled Permanent Magnet Synchronous Motor With Permanent Magnet DefectDocument4 pagesAnalysis For Fault Detection of Vector-Controlled Permanent Magnet Synchronous Motor With Permanent Magnet DefectkkarthiksNo ratings yet
- Alexander The Great: The Mathematical Genius GrothendieckDocument8 pagesAlexander The Great: The Mathematical Genius GrothendieckLoki OdinsonNo ratings yet
- Lesson 4: Listening and Reading: Prepared by Kinsley NG Sen Fa, Segi College Penang, Program DECEDocument23 pagesLesson 4: Listening and Reading: Prepared by Kinsley NG Sen Fa, Segi College Penang, Program DECEKinsley Ng Sen FaNo ratings yet
- Om Bio Science & Pharma College Haridwar, U.KDocument8 pagesOm Bio Science & Pharma College Haridwar, U.KVasu ThakurNo ratings yet
- Fluids and ElectrolytesDocument15 pagesFluids and ElectrolytesTrisha UmaliNo ratings yet
- Profile BacklinksDocument4 pagesProfile BacklinksVishal RohillaNo ratings yet
- Differential Equations Pyqs Based On Degree and OrderDocument32 pagesDifferential Equations Pyqs Based On Degree and Orderanitadevi7379No ratings yet
- Contracted PelvisDocument48 pagesContracted Pelviskalpana shona100% (4)
- TRF Blank FormDocument5 pagesTRF Blank FormMary Ann RanayNo ratings yet