Caries Risk Assesment and Caries Vaccine: K.Santoshi Mds Ii
Caries Risk Assesment and Caries Vaccine: K.Santoshi Mds Ii
Download as pptx, pdf, or txt
You might also like
- The Immediacy Concept: Treatment Planning from Analog to DigitalFrom EverandThe Immediacy Concept: Treatment Planning from Analog to DigitalNo ratings yet
- Color in Dentistry A Clinical Guide To Predictable EstheticsDocument1 pageColor in Dentistry A Clinical Guide To Predictable EstheticsGabriel LazarNo ratings yet
- Fixed Orthodontic Appliances: A Practical GuideFrom EverandFixed Orthodontic Appliances: A Practical GuideRating: 1 out of 5 stars1/5 (1)
- Textbook of Pediatric Dentistry-3rd EditionDocument18 pagesTextbook of Pediatric Dentistry-3rd EditionAnna NgNo ratings yet
- Mds SyllabusDocument78 pagesMds SyllabusFrancis PrathyushaNo ratings yet
- Lymph Nodes Normal and MalignantDocument12 pagesLymph Nodes Normal and MalignantMagzNo ratings yet
- Development of Tongue and PalateDocument79 pagesDevelopment of Tongue and PalateSanthoshi Reddy50% (2)
- Prescott Harley Klein's Microbiology 7th EditionDocument37 pagesPrescott Harley Klein's Microbiology 7th EditionJendri Mamangkey-kossoh25% (4)
- Growth Assessment ParametersDocument97 pagesGrowth Assessment ParametersAurthi ElamparithiNo ratings yet
- Assessment of Nicotine Dependence Among Adolescent and Young Adult SmokersDocument6 pagesAssessment of Nicotine Dependence Among Adolescent and Young Adult Smokersr4adenNo ratings yet
- International Caries Detection and Assessment System (ICDAS) PDFDocument4 pagesInternational Caries Detection and Assessment System (ICDAS) PDFKelvin Jaya AlamNo ratings yet
- Journal Laser and Its Use in Pediatric Dentistry A ReviewDocument5 pagesJournal Laser and Its Use in Pediatric Dentistry A ReviewTiaraNo ratings yet
- Prenatal and Postnatal Growth of Mandible and TMJ NewDocument133 pagesPrenatal and Postnatal Growth of Mandible and TMJ NewShraddha PatilNo ratings yet
- Biological Restorations in Children: January 2016Document4 pagesBiological Restorations in Children: January 2016Mel LlerenaNo ratings yet
- Book Reviews and Article Abstracts: Radiographic Cephalometry: From Basics To 3-D Imaging, 3rd EditionDocument1 pageBook Reviews and Article Abstracts: Radiographic Cephalometry: From Basics To 3-D Imaging, 3rd EditionRahma RahmaNo ratings yet
- Seminar15 Mid 180118092933Document89 pagesSeminar15 Mid 180118092933Aditee AgrawalNo ratings yet
- CHD LD FinalDocument129 pagesCHD LD FinalMounika KinjarapuNo ratings yet
- Sepsis: Sepsis and Septic ShockDocument22 pagesSepsis: Sepsis and Septic ShockWialda Dwi rodyahNo ratings yet
- MDS Pediatric and Preventive DentistryDocument61 pagesMDS Pediatric and Preventive DentistryfathimapedoNo ratings yet
- Caries VaccineDocument30 pagesCaries Vaccinemangesh andhare100% (1)
- Clinical Case PresentationDocument20 pagesClinical Case PresentationدرالجمانNo ratings yet
- Epidemiologi Dental CariesDocument21 pagesEpidemiologi Dental CariesSampahAjaNo ratings yet
- Diagnosis, Examination and Treatment PlanningDocument28 pagesDiagnosis, Examination and Treatment PlanningfitsumNo ratings yet
- Facial NerveDocument65 pagesFacial NerveHemangi100% (1)
- Management of Non-Carious Lesions Final 3.7.23Document88 pagesManagement of Non-Carious Lesions Final 3.7.23Shivani ParmarNo ratings yet
- Library Dissertation in Conservative Dentistry and EndodonticsDocument5 pagesLibrary Dissertation in Conservative Dentistry and EndodonticsWriteMyPersuasivePaperCanadaNo ratings yet
- Aae Systemic AntibioticsDocument8 pagesAae Systemic AntibioticsIulia CiobanuNo ratings yet
- Cyst of Jaws-RadiologyDocument60 pagesCyst of Jaws-RadiologyshabeelpnNo ratings yet
- Lasers in Pediatric Dentistry - 2Document82 pagesLasers in Pediatric Dentistry - 2Shameena KnNo ratings yet
- Nanotechnology-The Era of Molecular DentistryDocument14 pagesNanotechnology-The Era of Molecular DentistryAmar BimavarapuNo ratings yet
- Extraoral Radiography PDFDocument2 pagesExtraoral Radiography PDFJackNo ratings yet
- Psychology in OrthodonticDocument11 pagesPsychology in OrthodonticPurwana NasirNo ratings yet
- Avulsion: DEFINITION: - Tooth Avulsion (Exarticulation) Implies Total Displacement of The ToothDocument39 pagesAvulsion: DEFINITION: - Tooth Avulsion (Exarticulation) Implies Total Displacement of The Toothshailesh_shenoyNo ratings yet
- Biomechanics of Edentulous StateDocument30 pagesBiomechanics of Edentulous StateManash Jyoti DekaNo ratings yet
- 5Document86 pages5Georgi GugicevNo ratings yet
- 5 - Calcium Hydroxide Vs Mineral Trioxide Aggregates For Partial Pulpotomy of Permanent Molars With Deep Caries PDFDocument6 pages5 - Calcium Hydroxide Vs Mineral Trioxide Aggregates For Partial Pulpotomy of Permanent Molars With Deep Caries PDFAbdul Rahman AlmishhdanyNo ratings yet
- Physical CarcinogenesisDocument3 pagesPhysical CarcinogenesisamaraadhithiyaNo ratings yet
- Abscess of THE PeriodontiumDocument57 pagesAbscess of THE PeriodontiumSandeep SunilNo ratings yet
- Anesthesia and Extraction in Children: Dr. Masar MohammedDocument46 pagesAnesthesia and Extraction in Children: Dr. Masar Mohammedscribfoerte100% (1)
- Good Morning.: @areebazainabDocument42 pagesGood Morning.: @areebazainabshabana waniNo ratings yet
- DetectionDocument8 pagesDetectionJanani GopalakrishnanNo ratings yet
- Burning Mouth SyndromeDocument4 pagesBurning Mouth SyndromeGhada AlqrnawiNo ratings yet
- Early Childhood CariesDocument35 pagesEarly Childhood Cariessandsiramesh100% (1)
- 1-Malignant Melanoma of The Oral Cavity A ReviewDocument3 pages1-Malignant Melanoma of The Oral Cavity A ReviewPaomo Zhixia EarlyNo ratings yet
- Dental ErosionDocument4 pagesDental ErosionmirfanulhaqNo ratings yet
- Role of A Pedodontist in Cleft Lip and Cleft Palate Rehabilitation - An OverviewDocument25 pagesRole of A Pedodontist in Cleft Lip and Cleft Palate Rehabilitation - An OverviewIJAR JOURNALNo ratings yet
- Dental AnxietyDocument3 pagesDental AnxietyLau Kien YeeNo ratings yet
- Orofacial Complications of Non Surgical Cancer TherapyDocument59 pagesOrofacial Complications of Non Surgical Cancer TherapyKassim OboghenaNo ratings yet
- Treatment Planning in Conservative DentistryDocument9 pagesTreatment Planning in Conservative DentistryteriusNo ratings yet
- Dentogingival UnitDocument53 pagesDentogingival Unitperiodontics0780% (5)
- CherubismDocument12 pagesCherubismSureeratPatima100% (1)
- Advanced Microbial Diagnostic Techniques in PeriodonticsDocument38 pagesAdvanced Microbial Diagnostic Techniques in PeriodonticsPiyusha Sharma100% (1)
- Medical Terminologies - RoqueDocument80 pagesMedical Terminologies - RoqueRaven Yu100% (1)
- What Is EBD?Document7 pagesWhat Is EBD?RATHEESH M. S.No ratings yet
- Third Bds Question PapersDocument2 pagesThird Bds Question PaperssoundharyaNo ratings yet
- Catch It Right - A Case Report On Occlusal SplintDocument6 pagesCatch It Right - A Case Report On Occlusal SplintSkAliHassanNo ratings yet
- Epithelial-Mesenchymal Signalling Regulating Tooth MorphogenesisDocument2 pagesEpithelial-Mesenchymal Signalling Regulating Tooth MorphogenesisalifNo ratings yet
- Maxillary Sinus (NXPowerLite) .PPT / Orthodontic Courses by Indian Dental AcademyDocument18 pagesMaxillary Sinus (NXPowerLite) .PPT / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- Minimally Invasive Periodontal Therapy: Clinical Techniques and Visualization TechnologyFrom EverandMinimally Invasive Periodontal Therapy: Clinical Techniques and Visualization TechnologyNo ratings yet
- My Dentist and the Tooth Fairy: Activity and Coloring BookFrom EverandMy Dentist and the Tooth Fairy: Activity and Coloring BookNo ratings yet
- Orofacial Pain: A Guide to Medications and ManagementFrom EverandOrofacial Pain: A Guide to Medications and ManagementGlenn T. ClarkNo ratings yet
- Profesionally Applied Topical Fluorides FinalDocument66 pagesProfesionally Applied Topical Fluorides FinalSanthoshi ReddyNo ratings yet
- Topical FluorideDocument106 pagesTopical FluorideSanthoshi Reddy100% (1)
- JC 5Document33 pagesJC 5Santhoshi ReddyNo ratings yet
- Remineralizing Agents: Remineralizatio N Action Buffering ActionDocument1 pageRemineralizing Agents: Remineralizatio N Action Buffering ActionSanthoshi ReddyNo ratings yet
- Green DentistryDocument2 pagesGreen DentistrySanthoshi ReddyNo ratings yet
- Srujana PosterDocument1 pageSrujana PosterSanthoshi ReddyNo ratings yet
- Fear Anxity PhobiaDocument77 pagesFear Anxity PhobiaSanthoshi ReddyNo ratings yet
- Morphology of Primary Dentition PPT 1Document29 pagesMorphology of Primary Dentition PPT 1Santhoshi ReddyNo ratings yet
- Danger Area of Face: K.Santoshi I Mds Department of PedodonticsDocument10 pagesDanger Area of Face: K.Santoshi I Mds Department of PedodonticsSanthoshi Reddy100% (1)
- K.Santoshi 1 Year PG: BiostatisticsDocument60 pagesK.Santoshi 1 Year PG: BiostatisticsSanthoshi ReddyNo ratings yet
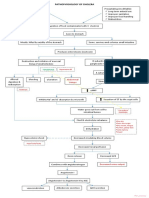
- Pathophysiology of Cholera PDFDocument1 pagePathophysiology of Cholera PDFRameshKrishnanNo ratings yet
- Proper Excreta Disposal, Food Safety Sanitation-Video LecDocument15 pagesProper Excreta Disposal, Food Safety Sanitation-Video LecEden LacsonNo ratings yet
- 18.1-FAMILY ENTEROBACTERIACEAE and TESTSDocument2 pages18.1-FAMILY ENTEROBACTERIACEAE and TESTSJesette KhoNo ratings yet
- Antigen Antibody & ReactionsDocument68 pagesAntigen Antibody & ReactionsUmar R KhanNo ratings yet
- Abzymes/ Catalytic AntibodiesDocument24 pagesAbzymes/ Catalytic AntibodiesRamuNo ratings yet
- IBV Variant Italian-O2Document5 pagesIBV Variant Italian-O2vetvetNo ratings yet
- Kostis William - ACE Inhibitor-Induced Angioedema - A ReviewDocument7 pagesKostis William - ACE Inhibitor-Induced Angioedema - A ReviewluongcongthucNo ratings yet
- Biruh T Workeneh Hyponatremia Demystified IntegratingDocument17 pagesBiruh T Workeneh Hyponatremia Demystified IntegratingsaqqarazoserNo ratings yet
- Example of An Interview EssayDocument7 pagesExample of An Interview Essayafhbebseg100% (2)
- Deoxyribo Virus and RibovirusDocument5 pagesDeoxyribo Virus and RibovirusAlyssa MercadoNo ratings yet
- Biology 2081-03-01Document3 pagesBiology 2081-03-01brabimpratap999No ratings yet
- RBC MorphologyDocument9 pagesRBC MorphologybiancsNo ratings yet
- Answers To Virology MCQ Paper 1Document8 pagesAnswers To Virology MCQ Paper 1Idrissa ContehNo ratings yet
- Lymph Node PathologyDocument4 pagesLymph Node PathologyGerardLum0% (1)
- Bacterial ClassificationDocument7 pagesBacterial ClassificationAsimNo ratings yet
- Seed Coating With The Synthetic ConsortiumDocument10 pagesSeed Coating With The Synthetic Consortiumwaheed akramNo ratings yet
- STR2B Sandaga Soriano - Final PaperDocument34 pagesSTR2B Sandaga Soriano - Final Papersenior highNo ratings yet
- Medicinal Properties of Pleurotus Species (Oyster Mushroom) : A ReviewDocument13 pagesMedicinal Properties of Pleurotus Species (Oyster Mushroom) : A ReviewEdward Marques de SouzaNo ratings yet
- A Guide To The Management of Acute Rhinosinusitis in Primary CareDocument4 pagesA Guide To The Management of Acute Rhinosinusitis in Primary CarecubillahhNo ratings yet
- Cambridge O Level: Biology 5090/11Document20 pagesCambridge O Level: Biology 5090/11Hasnat AhsanNo ratings yet
- Para ReviewerDocument10 pagesPara ReviewerStephanie Kate ArriolaNo ratings yet
- AAGP2 enDocument3 pagesAAGP2 enLince WijoyoNo ratings yet
- Innate & Adaptive ImmunityDocument14 pagesInnate & Adaptive ImmunityGde Angga JNo ratings yet
- Immunology ExamDocument9 pagesImmunology ExamNICHOLAS KAUMBANo ratings yet
- HEMATOLOGY 1 WEEK 7 PrintDocument4 pagesHEMATOLOGY 1 WEEK 7 PrintRose Neil LapuzNo ratings yet
- Cap 2019 04 01 PDFDocument58 pagesCap 2019 04 01 PDFRajeev PareekNo ratings yet
- Unit 3 Monera KingdomDocument6 pagesUnit 3 Monera KingdomYolanda Fernández VelascoNo ratings yet
- PuerperiumDocument16 pagesPuerperiumLi FaungNo ratings yet
- Biology Genetic Mutation NotesDocument1 pageBiology Genetic Mutation NotesTiffany Gallina100% (2)