Intro To EP
Intro To EP
Download as ppt, pdf, or txt
At a glance
Powered by AI
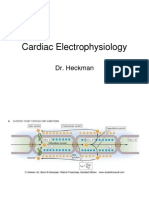
An EPS study can be used for diagnostic, prognostic and therapeutic purposes. It involves placing catheters in the heart to record electrical activity and induce arrhythmias.
Non-diagnostic initial evaluation of palpitations or syncope, unclear mechanism of arrhythmia, and sudden death risk stratification are some diagnostic indications for an EPS study.
Assess electrophysiological functions of the sinus node and conduction system, and evaluate arrhythmia induction are some aims of an EPS study.
You might also like
- Ibhre Prep 01 KeyDocument16 pagesIbhre Prep 01 Keyanon-747764100% (5)
- CMS Psychiatry 4 FormDocument48 pagesCMS Psychiatry 4 FormMina Maged Maher88% (8)
- Board Stiff ThreeDocument440 pagesBoard Stiff Threewin co100% (1)
- EKG Clep TestDocument13 pagesEKG Clep TestElissa LafondNo ratings yet
- 7.5.2016 IBHRE CCDS Physician 17 - FINAL PDFDocument8 pages7.5.2016 IBHRE CCDS Physician 17 - FINAL PDFAlexander Edo TondasNo ratings yet
- Eps Course Basic ElectrophysiologyDocument23 pagesEps Course Basic Electrophysiologytisya_endut2081100% (1)
- Cardiac Electrophysiology Technician or Electrophysiology TechniDocument2 pagesCardiac Electrophysiology Technician or Electrophysiology Techniapi-78900391No ratings yet
- Cardiac Pacing and ICD ReviewDocument21 pagesCardiac Pacing and ICD ReviewAlexander Edo Tondas100% (1)
- Advanced ICD Troubleshooting Part 2 PACE 2006 PDFDocument27 pagesAdvanced ICD Troubleshooting Part 2 PACE 2006 PDFSrajner PéterNo ratings yet
- PcicardDocument2 pagesPcicardWahdat100% (2)
- Cardiac Electrophysiology 2 An Advanced Visual Guide For Nurses Techs and Fellows 2EDocument294 pagesCardiac Electrophysiology 2 An Advanced Visual Guide For Nurses Techs and Fellows 2ETemptation100% (4)
- Basics of PacemakerDocument121 pagesBasics of Pacemakerjeenath justin doss100% (1)
- 7.5.2016 IBHRE CCDS Physician 17 - FINAL PDFDocument8 pages7.5.2016 IBHRE CCDS Physician 17 - FINAL PDFAlexander Edo TondasNo ratings yet
- CT BasicsDocument29 pagesCT Basicsusfcards100% (3)
- NCP: DysrhythmiasDocument12 pagesNCP: DysrhythmiasJavie100% (3)
- Essential Cardiac Electrophysiology: The Self-Assessment ApproachFrom EverandEssential Cardiac Electrophysiology: The Self-Assessment ApproachNo ratings yet
- EKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!From EverandEKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!No ratings yet
- Cardiac MappingFrom EverandCardiac MappingMohammad ShenasaNo ratings yet
- ECG & EKG Interpretation: How to interpret ECG & EKG, including rhythms, arrhythmias, and more!From EverandECG & EKG Interpretation: How to interpret ECG & EKG, including rhythms, arrhythmias, and more!No ratings yet
- Clinical Electrocardiography, Enhanced Edition: A TextbookFrom EverandClinical Electrocardiography, Enhanced Edition: A TextbookNo ratings yet
- Basic EP 01Document53 pagesBasic EP 01Hany100% (4)
- 12 Lead InterpretationDocument33 pages12 Lead InterpretationTodd CoxNo ratings yet
- 439 3 Electrophysiology & ECG BasicsDocument34 pages439 3 Electrophysiology & ECG Basicsjpoutre100% (1)
- Ventricular Arrhythmias: Robert J. Hariman, MDDocument51 pagesVentricular Arrhythmias: Robert J. Hariman, MDusfcardsNo ratings yet
- Cardiac Implantable Pacemakers: Rocio Rodriguez Advanced Engineering Materials Dr. HaiderDocument23 pagesCardiac Implantable Pacemakers: Rocio Rodriguez Advanced Engineering Materials Dr. HaiderChio Villarreal100% (1)
- Cardiac ElectrophysiologyDocument6 pagesCardiac Electrophysiologyareznik3007No ratings yet
- Pacing ManualDocument76 pagesPacing ManualMirela Sfaraiala Luculescu100% (1)
- Temporary Pacemakers-SICU's 101 PrimerDocument51 pagesTemporary Pacemakers-SICU's 101 Primerwaqas_xsNo ratings yet
- ICD Troubleshooting (Heart)Document13 pagesICD Troubleshooting (Heart)Prem KumarNo ratings yet
- Hemodynamics in The Cath Lab 2Document45 pagesHemodynamics in The Cath Lab 2usfcards100% (1)
- Guaranteed To Pass: Exam Tidbits in Easy To Digest, Bite Sized MorselsDocument2 pagesGuaranteed To Pass: Exam Tidbits in Easy To Digest, Bite Sized MorselsAmberNo ratings yet
- Pacemaker Timing & IntervalsDocument124 pagesPacemaker Timing & IntervalsNiranjan Reddy100% (1)
- Cardiac Resynchronization Therapy (Sep 19 2007) - (1841846376) - (CRC Press)Document337 pagesCardiac Resynchronization Therapy (Sep 19 2007) - (1841846376) - (CRC Press)Morozovschi VitalieNo ratings yet
- Guaranteed To Pass: Exam Tidbits in Easy To Digest, Bite Sized MorselsDocument2 pagesGuaranteed To Pass: Exam Tidbits in Easy To Digest, Bite Sized MorselsAmberNo ratings yet
- PaceMaker HAckingDocument14 pagesPaceMaker HAckingRemi BlanchetteNo ratings yet
- Classic M Mode Echocardiography ECHOCARDIOGRAPHY BOARD REVIEWDocument73 pagesClassic M Mode Echocardiography ECHOCARDIOGRAPHY BOARD REVIEWMande SamuelNo ratings yet
- Cardiac ElectrophysiologyDocument40 pagesCardiac Electrophysiologyashwinagrawal1995No ratings yet
- 4 5857477510681329907 PDFDocument290 pages4 5857477510681329907 PDFDeEo Ono100% (2)
- Revised AntiarrhythmicsDocument29 pagesRevised AntiarrhythmicsDang CuevasNo ratings yet
- Pacemaker Therapy: Attila Kónyi M.D., PH.D Heart Institute University of PécsDocument42 pagesPacemaker Therapy: Attila Kónyi M.D., PH.D Heart Institute University of PécsIbrahim Kimymaru ZuzuranNo ratings yet
- Cardiac Pacing For The SurgeonsDocument46 pagesCardiac Pacing For The SurgeonsRezwanul Hoque BulbulNo ratings yet
- 2d Speckle Tracking Echocardiography PDFDocument11 pages2d Speckle Tracking Echocardiography PDFYEAG92100% (1)
- 2024 Heart Failure Preserved Ejection Fraction LANCETDocument10 pages2024 Heart Failure Preserved Ejection Fraction LANCETAlirio Angulo QuinteroNo ratings yet
- PacemakersDocument69 pagesPacemakersdocjeevan89100% (1)
- Pacemaker Invasive Cardiac PacingDocument57 pagesPacemaker Invasive Cardiac PacingAhmad Khalil Ahmad Al-SadiNo ratings yet
- Pacemaker MalfunctionDocument23 pagesPacemaker MalfunctionsshansraNo ratings yet
- Adult Echocardiography Protocol 14 2Document10 pagesAdult Echocardiography Protocol 14 2api-349402240No ratings yet
- Braunwald Lecture Series #2Document33 pagesBraunwald Lecture Series #2usfcards100% (2)
- Ultrasound EchocardiographyDocument3 pagesUltrasound EchocardiographyDr. MLKNo ratings yet
- 123 Sonography Prosthetic Valves AssesmentDocument9 pages123 Sonography Prosthetic Valves AssesmentNavojit Chowdhury100% (1)
- DR K Chan - Ecg For SVT Made EasyDocument66 pagesDR K Chan - Ecg For SVT Made Easyapi-346486620No ratings yet
- EDAN Holter System V1.2Document27 pagesEDAN Holter System V1.2Suciu FlorinNo ratings yet
- Mitral RegurgitationDocument6 pagesMitral RegurgitationMelfi Triani SiskaNo ratings yet
- Basics & Timing-PmDocument120 pagesBasics & Timing-PmWiwik Puji Lestari100% (3)
- Echocardiography: Pericardial Effusions & Cardiactamponade: David M. Whitaker, MDDocument43 pagesEchocardiography: Pericardial Effusions & Cardiactamponade: David M. Whitaker, MDusfcardsNo ratings yet
- Sinus Node DysfunctionDocument11 pagesSinus Node DysfunctionVasishta Nadella100% (1)
- Cath Lab Essentials: Basic Hemodynamics For The Cath Lab and ICUDocument38 pagesCath Lab Essentials: Basic Hemodynamics For The Cath Lab and ICUDr. TomNo ratings yet
- HBP C315HIS Implant Procedure-eLearnDocument35 pagesHBP C315HIS Implant Procedure-eLearnRichiNo ratings yet
- Basic Coronary Angiography - All Slides PDFDocument55 pagesBasic Coronary Angiography - All Slides PDFCarlos Arroyo50% (2)
- CARDIAC ELECTROPHYSIOLOGY AND THE ELECTROCARDIOGRAM - ClinicalKey PDFDocument40 pagesCARDIAC ELECTROPHYSIOLOGY AND THE ELECTROCARDIOGRAM - ClinicalKey PDFMelanie DascăluNo ratings yet
- Guiedline Newly Strial Fibrilation - ACP - 2005Document10 pagesGuiedline Newly Strial Fibrilation - ACP - 2005api-3765169No ratings yet
- Echocardiography: Pericardial Effusions & Cardiactamponade: David M. Whitaker, MDDocument43 pagesEchocardiography: Pericardial Effusions & Cardiactamponade: David M. Whitaker, MDusfcardsNo ratings yet
- Echocardiography - LV FunctionDocument35 pagesEchocardiography - LV Functionusfcards100% (5)
- Problems in Echocardiography 2Document50 pagesProblems in Echocardiography 2usfcards82% (11)
- Ventricular Arrhythmias: Robert J. Hariman, MDDocument51 pagesVentricular Arrhythmias: Robert J. Hariman, MDusfcardsNo ratings yet
- "Adjunctive Therapy" Non ST Segment Elevation ACS: DR M R Thomas King's College Hospital. Advanced Angioplasty 2002Document42 pages"Adjunctive Therapy" Non ST Segment Elevation ACS: DR M R Thomas King's College Hospital. Advanced Angioplasty 2002usfcardsNo ratings yet
- Thrombolytics: Interventional FellowDocument51 pagesThrombolytics: Interventional Fellowusfcards100% (1)
- Fractional Flow ReserveDocument44 pagesFractional Flow Reserveusfcards100% (2)
- Case#1Document7 pagesCase#1usfcardsNo ratings yet
- Case#2Document4 pagesCase#2usfcardsNo ratings yet
- Hemodynamics in The Cath Lab 2Document45 pagesHemodynamics in The Cath Lab 2usfcards100% (1)
- Daniel W Mason MD FACC FASEDocument38 pagesDaniel W Mason MD FACC FASEusfcardsNo ratings yet
- Intro To EPDocument48 pagesIntro To EPusfcards100% (2)
- Ventricular Tachycardia in The Ischemic HeartDocument57 pagesVentricular Tachycardia in The Ischemic Heartusfcards100% (3)
- Braunwald - UA and NSTEMIDocument49 pagesBraunwald - UA and NSTEMIusfcards100% (2)
- Braunwald Lecture Series #2Document33 pagesBraunwald Lecture Series #2usfcards100% (2)
- The Search For Syncope in A Young Athlete: E. Harrison, MDDocument20 pagesThe Search For Syncope in A Young Athlete: E. Harrison, MDusfcardsNo ratings yet
- Braunwald: Chronic Coronary Artery DiseaseDocument122 pagesBraunwald: Chronic Coronary Artery Diseaseusfcards100% (1)
- POBA Vs BMSDocument64 pagesPOBA Vs BMSusfcardsNo ratings yet
- Thrombolytics: Interventional FellowDocument51 pagesThrombolytics: Interventional Fellowusfcards100% (1)
- Braunwald - UA and NSTEMIDocument49 pagesBraunwald - UA and NSTEMIusfcards100% (2)
- Braunwalds PCI For AMIDocument44 pagesBraunwalds PCI For AMIusfcards100% (1)
- ECG Short Note Chula EP PDFDocument62 pagesECG Short Note Chula EP PDFKhuniok SixcoNo ratings yet
- Pathophysiology On ArrhythmiaDocument34 pagesPathophysiology On ArrhythmiaYhr Yh100% (1)
- WPW With Af Case ReportDocument4 pagesWPW With Af Case Report王怡君No ratings yet
- Spesifikasi-Alat-UM-Prosim 8 User Manual + SPO2 Module + YSIDocument6 pagesSpesifikasi-Alat-UM-Prosim 8 User Manual + SPO2 Module + YSIBayu FebriandNo ratings yet
- 50 Emergency DrugsDocument70 pages50 Emergency DrugsderizNo ratings yet
- ELECTROCARDIOGRAPHYDocument75 pagesELECTROCARDIOGRAPHYMeliaNo ratings yet
- Pharmacology Exam 4 ReviewDocument8 pagesPharmacology Exam 4 ReviewAnonymous 0Yvbef1xNo ratings yet
- Superimposed ECG PDFDocument93 pagesSuperimposed ECG PDFEdalyn CapiliNo ratings yet
- 10 Steps To Learn ECG InterpretationDocument5 pages10 Steps To Learn ECG InterpretationMohammadNo ratings yet
- Neonatal Medication Protocols: Drug: Digoxin PresentationDocument1 pageNeonatal Medication Protocols: Drug: Digoxin Presentation-Yohanes Firmansyah-No ratings yet
- ArythmiaDocument345 pagesArythmiaMuhammad ArifinNo ratings yet
- Pharmacology Nursing Mnemonics & Tips - NurseslabsDocument19 pagesPharmacology Nursing Mnemonics & Tips - Nurseslabsmaniz442100% (4)
- Disorders of Cardiac RhythmDocument66 pagesDisorders of Cardiac RhythmslyfoxkittyNo ratings yet
- Pci To Cto - Copy SssDocument238 pagesPci To Cto - Copy SssSohil3100% (1)
- Case Study 29Document2 pagesCase Study 29Edna MooreNo ratings yet
- Nursing Care PlanDocument22 pagesNursing Care Planaln00550% (2)
- Artigo 1 Physical Principles of The DefibrillatorDocument2 pagesArtigo 1 Physical Principles of The DefibrillatorLucas Martins FelipeNo ratings yet
- SyllabusDocument96 pagesSyllabusBS NishanthNo ratings yet
- Catheter Ablation For AFDocument12 pagesCatheter Ablation For AFPeny Ruth Jessica DamanikNo ratings yet
- Implementation of Low Delay Dual Chamber Pacemaker Using VerilogDocument4 pagesImplementation of Low Delay Dual Chamber Pacemaker Using VerilogMeghanand KumarNo ratings yet
- DefibrillatorDocument10 pagesDefibrillatorMakhanVermaNo ratings yet
- Cardiac Disease in PregnancyDocument44 pagesCardiac Disease in PregnancyNariska Cooper100% (1)
- Hemodynamic Unstable Patient Following ArrhythmiaDocument30 pagesHemodynamic Unstable Patient Following Arrhythmialew chin hongNo ratings yet
- ECG ArrythemiaDocument79 pagesECG ArrythemiaMahadevNo ratings yet
- BSU College of Nursing Assessment FormDocument17 pagesBSU College of Nursing Assessment FormLucille Allen100% (32)
- Cardiac RehabilitationDocument28 pagesCardiac Rehabilitationshivalingam20No ratings yet
- Omron M3 Intellisense (HEM-7051-E) Manual PDFDocument38 pagesOmron M3 Intellisense (HEM-7051-E) Manual PDFZee Eagle100% (1)