Download as ppt, pdf, or txt
You might also like
- E-Book Smart Money SMCDocument33 pagesE-Book Smart Money SMCMfxMazprofx95% (354)
- MicrobiologyDocument6 pagesMicrobiologynoreplyneet46No ratings yet
- Doh Health ProgramsDocument21 pagesDoh Health Programsrgng_1880304067% (3)
- Biomechanics of GaitDocument27 pagesBiomechanics of Gaitsebastiao_est3197No ratings yet
- Cyriax IntroDocument14 pagesCyriax IntrodrrajmptnNo ratings yet
- Biomechanics Ankle PresentationDocument10 pagesBiomechanics Ankle Presentationx.cortez100% (1)
- Pathomechanics of Wrist: by G. Hema MaliniDocument20 pagesPathomechanics of Wrist: by G. Hema MaliniHema Malini100% (1)
- 2nd - Edition The Syrian Uprising and Signs of The Hour PDFDocument463 pages2nd - Edition The Syrian Uprising and Signs of The Hour PDFMfxMazprofxNo ratings yet
- Manual Therapy TechniquesDocument30 pagesManual Therapy TechniquesNistara Singh Chawla100% (1)
- Length Tension Testing Book 2, Upper Quadrant: A Workbook of Manual Therapy TechniquesFrom EverandLength Tension Testing Book 2, Upper Quadrant: A Workbook of Manual Therapy TechniquesRating: 1 out of 5 stars1/5 (1)
- Compartment Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandCompartment Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Length Tension Testing Book 1, Lower Quadrant: A Workbook of Manual Therapy TechniquesFrom EverandLength Tension Testing Book 1, Lower Quadrant: A Workbook of Manual Therapy TechniquesRating: 3.5 out of 5 stars3.5/5 (3)
- Neuro Developmental Treatment (NDT) Techniques: HistoryDocument3 pagesNeuro Developmental Treatment (NDT) Techniques: HistoryGafencu SergiuNo ratings yet
- Bio Mechanics and Pathomechanics of Ankle JointDocument35 pagesBio Mechanics and Pathomechanics of Ankle Joint56 Vignesh j 079No ratings yet
- Effectiveness of Mulligan's Mobilization Technique Versus Eccentric Exercises On Pain, Hand Grip Strength and Function in Subjects With Lateral EpicondylitisDocument8 pagesEffectiveness of Mulligan's Mobilization Technique Versus Eccentric Exercises On Pain, Hand Grip Strength and Function in Subjects With Lateral EpicondylitisInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Biomechanics & Pathomechanics of HandDocument81 pagesBiomechanics & Pathomechanics of HandAmrita L. Tomar67% (3)
- Brunnstrom's Movement Therapy: Concepts and PrinciplesDocument29 pagesBrunnstrom's Movement Therapy: Concepts and PrinciplesAlina ShaukatNo ratings yet
- Physiotherapy For PoliomyelitisDocument16 pagesPhysiotherapy For Poliomyelitisabdalsucs100% (1)
- McKenzie CONCEPT AnilDocument12 pagesMcKenzie CONCEPT AnilSOUMYADEEP BHUINYANo ratings yet
- Tennis Elbow ExerciseDocument2 pagesTennis Elbow Exercisedhirajkumar_1No ratings yet
- Pathomechanics of Knee JointDocument55 pagesPathomechanics of Knee JointAkhila SudheerbabuNo ratings yet
- The Patho-Mechanics of LBPDocument32 pagesThe Patho-Mechanics of LBPydp100% (1)
- Resisted ExerciseDocument29 pagesResisted ExerciseVaraNo ratings yet
- Mulligan Spinal Concept PDFDocument7 pagesMulligan Spinal Concept PDFRabbeya AltafNo ratings yet
- Disability Evaluation: Radhika ChintamaniDocument58 pagesDisability Evaluation: Radhika ChintamaniBhavya Amin0% (1)
- Bicipital TendonitisDocument2 pagesBicipital TendonitisJ Cheung100% (2)
- Biomechanics of Patellofemoral JointDocument44 pagesBiomechanics of Patellofemoral JointMaluNo ratings yet
- BobathDocument28 pagesBobathSaba SamimNo ratings yet
- Therapeutic Gymnasium PDFDocument45 pagesTherapeutic Gymnasium PDFPrabhat SharmaNo ratings yet
- Brunnstrom ApproachDocument33 pagesBrunnstrom ApproachAISHWARYA SWAMINATHANNo ratings yet
- Resisted Isometric TestingDocument15 pagesResisted Isometric TestingDr. Disha Rupareliya BhateNo ratings yet
- Types of Movement &, ExerciseDocument23 pagesTypes of Movement &, ExerciseAhmed50% (2)
- BFO-Ankle Foot Orthotics - Introduction and Biomechanical PrinciplesDocument9 pagesBFO-Ankle Foot Orthotics - Introduction and Biomechanical PrinciplesnovitaNo ratings yet
- PAE 1 Introduction To ElectrotherapyDocument37 pagesPAE 1 Introduction To ElectrotherapyHasnat AhmedNo ratings yet
- Physiotherapy Rehabilitation Guidelines - Lumbar DisectomyDocument6 pagesPhysiotherapy Rehabilitation Guidelines - Lumbar Disectomyalina4891No ratings yet
- Proprioceptive Neuromuscular FacilitationDocument7 pagesProprioceptive Neuromuscular Facilitationpsionx100% (1)
- Causes of Restriction of ROMDocument33 pagesCauses of Restriction of ROMRonak Patel100% (3)
- Suspension TherapyDocument52 pagesSuspension TherapyROJA MACHERLA0% (1)
- Manual Muscle Testing: Grade Value DescriptionDocument40 pagesManual Muscle Testing: Grade Value Descriptionjoanna gurtizaNo ratings yet
- Physiotherapy Management Plan PDFDocument3 pagesPhysiotherapy Management Plan PDFsunilbijlani100% (3)
- Pathomechanics of Wrist and HandDocument16 pagesPathomechanics of Wrist and Handsonali tushamerNo ratings yet
- Research Methodology: For All Physiotherapy and Allied Health Sciences StudentsDocument1 pageResearch Methodology: For All Physiotherapy and Allied Health Sciences StudentsProductivity 100100% (1)
- Functional Re-Education TrainingDocument24 pagesFunctional Re-Education Trainingtamilvanan3100% (2)
- Articular Neurophysiology: Presented by - Yogesh VyasDocument15 pagesArticular Neurophysiology: Presented by - Yogesh VyasvictoryvelavaNo ratings yet
- 3 Advantage of Free Ex 3Document13 pages3 Advantage of Free Ex 3Farrukh ShahzadNo ratings yet
- Role of Physiotherapy in Management of Polio..seminarDocument14 pagesRole of Physiotherapy in Management of Polio..seminarAmandeep SinghNo ratings yet
- 14 Biomechanics of Normal Human Gait PDFDocument26 pages14 Biomechanics of Normal Human Gait PDFDiego A. MezaNo ratings yet
- Schemes of ExercisesDocument12 pagesSchemes of Exercisesdnyanesh_23patilNo ratings yet
- Extensor Tendon InjuriesDocument18 pagesExtensor Tendon InjuriesaparnaNo ratings yet
- ICUDocument12 pagesICUNabilahNo ratings yet
- Joint MobilizationDocument35 pagesJoint Mobilizationkiran patil75% (4)
- Chapter 1 - Intro Current Concepts and Clinical Decision Making in Electrotherapy PDFDocument7 pagesChapter 1 - Intro Current Concepts and Clinical Decision Making in Electrotherapy PDFTracy Magpoc0% (1)
- Role of Physiotherapy in Management of Burns-HshDocument25 pagesRole of Physiotherapy in Management of Burns-HshChristopher Chibueze Igbo100% (1)
- Applied Biomechanics Arthroplasty: DR Abda ShaikhDocument42 pagesApplied Biomechanics Arthroplasty: DR Abda ShaikhAbida ShaikhNo ratings yet
- 1 Peripheral Manipulation Lecture OneDocument13 pages1 Peripheral Manipulation Lecture Onebuhlembatha304No ratings yet
- Joint MobilizationDocument5 pagesJoint MobilizationnainiswathireddygmaiNo ratings yet
- Neuromyotonia Short EssayDocument7 pagesNeuromyotonia Short EssaySurat TanprawateNo ratings yet
- Icf C.P. AssessmentDocument5 pagesIcf C.P. AssessmentAnonymous cCy8GpNo ratings yet
- MPT PDFDocument141 pagesMPT PDFSWATHI G ANo ratings yet
- Passivce Range of Motion ExercisesDocument29 pagesPassivce Range of Motion Exercisesvidyasagar pagilla100% (1)
- Physiotherapy For Stroke Patients - Physiotherapy Remedies For Victims of StrokeDocument9 pagesPhysiotherapy For Stroke Patients - Physiotherapy Remedies For Victims of StrokeHumaira RahmanNo ratings yet
- Proprioceptive Neuromuscular Facilitation: Vicky S. WardlawDocument44 pagesProprioceptive Neuromuscular Facilitation: Vicky S. WardlawPraneetha Nouduri100% (1)
- Recent Advances in PhysiotherapyFrom EverandRecent Advances in PhysiotherapyCecily PartridgeNo ratings yet
- Blessed Dementia ScaleDocument3 pagesBlessed Dementia ScaleMfxMazprofxNo ratings yet
- Canadian Neurological ScaleDocument3 pagesCanadian Neurological ScaleMfxMazprofxNo ratings yet
- Sacroiliac JointDocument152 pagesSacroiliac JointMfxMazprofxNo ratings yet
- Lower Limb TendinopathyDocument8 pagesLower Limb TendinopathyMfxMazprofxNo ratings yet
- Sacroilliac JointDocument37 pagesSacroilliac JointMfxMazprofxNo ratings yet
- Manual Therapy RecoveryDocument263 pagesManual Therapy RecoveryMfxMazprofxNo ratings yet
- Ortho AssessmentDocument91 pagesOrtho AssessmentMfxMazprofxNo ratings yet
- Zaki NewDocument1 pageZaki NewMfxMazprofxNo ratings yet
- Marklist IX A History & Pol. Sci 2020-21Document5 pagesMarklist IX A History & Pol. Sci 2020-21MfxMazprofxNo ratings yet
- Marklist IX B Geography 2020-21Document4 pagesMarklist IX B Geography 2020-21MfxMazprofxNo ratings yet
- Forex Rider Premier EditionDocument40 pagesForex Rider Premier EditionMfxMazprofxNo ratings yet
- Breakout Trading Explanatory NotesDocument47 pagesBreakout Trading Explanatory NotesMfxMazprofxNo ratings yet
- Dat MT Gbpusd M1 2019Document6 pagesDat MT Gbpusd M1 2019MfxMazprofxNo ratings yet
- Dat MT Gbpusd M1 2018Document43 pagesDat MT Gbpusd M1 2018MfxMazprofxNo ratings yet
- Williams Basic Nutrition and Diet Therapy 14th Edition Nix Test BankDocument10 pagesWilliams Basic Nutrition and Diet Therapy 14th Edition Nix Test Bankjonathanmelendezscpjzgfikb100% (12)
- Nepal HazardAssessment Part1Document114 pagesNepal HazardAssessment Part1suman subediNo ratings yet
- Auricular Acupuncture - Master Points: Point Zero (Ear Center, Point of Support, Umbilical Cord, Solar Plexus)Document4 pagesAuricular Acupuncture - Master Points: Point Zero (Ear Center, Point of Support, Umbilical Cord, Solar Plexus)Carleta StanNo ratings yet
- Intracellular Protein TraffickingDocument22 pagesIntracellular Protein TraffickingAsad IslamNo ratings yet
- Mapping The Antigenic and Genetic Evolution of in Uenza VirusDocument7 pagesMapping The Antigenic and Genetic Evolution of in Uenza Virusaleisha97No ratings yet
- Ebook Comprehensive Clinical Nephrology PDF Full Chapter PDFDocument67 pagesEbook Comprehensive Clinical Nephrology PDF Full Chapter PDFlloyd.odell127100% (39)
- Ouabain - The Optimal Solution For The Problem of Myocardial InfarctionDocument20 pagesOuabain - The Optimal Solution For The Problem of Myocardial InfarctionredsbooksNo ratings yet
- Presentation Minor Discomfort .Document20 pagesPresentation Minor Discomfort .Leena BaderNo ratings yet
- Nancy Leys Stepan Picturing Tropical NatureDocument285 pagesNancy Leys Stepan Picturing Tropical NatureAnonymous c89ovl62rcNo ratings yet
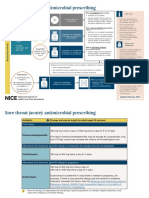
- Sore Throat Acute in Adults Antimicrobial Prescribing Visual SummaryDocument3 pagesSore Throat Acute in Adults Antimicrobial Prescribing Visual Summaryzobi2020No ratings yet
- Container GardeningDocument3 pagesContainer GardeningnevadablueNo ratings yet
- Prevalence of Hypertension and Associated Risk Factors Among University Students: Comparative StudyDocument9 pagesPrevalence of Hypertension and Associated Risk Factors Among University Students: Comparative StudyChristabella Natalia WijayaNo ratings yet
- Principles of Writing Good EnglishDocument2 pagesPrinciples of Writing Good EnglishTooba shafiq100% (1)
- Day 6 - APPEC 2021Document406 pagesDay 6 - APPEC 2021GaurieNo ratings yet
- Noi Dung On Tap hk2 Anh 6 - 144202323Document7 pagesNoi Dung On Tap hk2 Anh 6 - 144202323Đình ĐứcNo ratings yet
- Zincum MetallicumDocument3 pagesZincum MetallicumSuhas IngaleNo ratings yet
- Fitness Form Hospital ListDocument21 pagesFitness Form Hospital ListAshishNo ratings yet
- What Is A Delusion?Document10 pagesWhat Is A Delusion?Nadeem IqbalNo ratings yet
- NCP Submucous MyomaDocument1 pageNCP Submucous MyomaRichmon VillaminNo ratings yet
- Effects of Raw Vegan Diet On Periodontal and Dental ParametersDocument6 pagesEffects of Raw Vegan Diet On Periodontal and Dental ParametersKarolis KNo ratings yet
- TOEFL Test (Reading)Document10 pagesTOEFL Test (Reading)Misbahul MunirNo ratings yet
- Sample Proposal # Sample Proposal # Sample ProposalDocument6 pagesSample Proposal # Sample Proposal # Sample ProposalahmadbuneryNo ratings yet
- DefibrillatorPacemakers, Implantable ResynchronizationDocument110 pagesDefibrillatorPacemakers, Implantable ResynchronizationAbu OdaiNo ratings yet
- Vitamins, Minerals & FluidsDocument32 pagesVitamins, Minerals & FluidsEzekiel ReyesNo ratings yet
- Topper 2 110 7 1 Biology Solution Up201711171731 1510920087 7445Document7 pagesTopper 2 110 7 1 Biology Solution Up201711171731 1510920087 7445UMANo ratings yet
- MyelographyDocument22 pagesMyelographyKarylleNo ratings yet
- 191 - XBHA2103 - Human Anatomy and Physiology Lab ManualDocument10 pages191 - XBHA2103 - Human Anatomy and Physiology Lab ManualNajib Roslan100% (1)
- Irr Ra 11712Document11 pagesIrr Ra 11712Learsi Afable100% (2)