Module 6B
Module 6B
Download as pptx, pdf, or txt
You might also like
- Textbook of Diabetes 6th Ed 2024Document1,229 pagesTextbook of Diabetes 6th Ed 2024ricardoisrael1084100% (8)
- IMCI Guideline-2023 HeshamElsayedDocument57 pagesIMCI Guideline-2023 HeshamElsayedMalak Rageh100% (2)
- STUDENT-Sepsis - Fundamental - Reasoning Fillable-1Document5 pagesSTUDENT-Sepsis - Fundamental - Reasoning Fillable-1Laura PoultneyNo ratings yet
- Uncontrolled Blood Sugar NCPDocument4 pagesUncontrolled Blood Sugar NCPRawan KhateebNo ratings yet
- Module 6B - ITC ComplicationsDocument36 pagesModule 6B - ITC ComplicationsDexter MasongsongNo ratings yet
- Severe Acut MalnutritionDocument29 pagesSevere Acut Malnutritionniken maretasariNo ratings yet
- Care For The Child in Hospital: How To Identify and Treat Children Who Need Urgent CareDocument22 pagesCare For The Child in Hospital: How To Identify and Treat Children Who Need Urgent CareDahrren Grace JalonNo ratings yet
- Acute GastroenteritisDocument6 pagesAcute GastroenteritisSalman KhanNo ratings yet
- Chapter 71: Acute Gastroenteritis: Is The Child in Shock? Any Child With Shock Go Straight To Treatment Plan CDocument5 pagesChapter 71: Acute Gastroenteritis: Is The Child in Shock? Any Child With Shock Go Straight To Treatment Plan CKalichandren ArumugamNo ratings yet
- Acute GastroenteritisDocument38 pagesAcute GastroenteritisMuhammad khairul afizal RohimNo ratings yet
- Who Ten Step Management of Severe MalnutritionDocument4 pagesWho Ten Step Management of Severe MalnutritionShely Karma Astuti50% (4)
- Chapter 71: Acute Gastroenteritis: Is The Child in Shock? Any Child With Shock Go Straight To Treatment Plan CDocument7 pagesChapter 71: Acute Gastroenteritis: Is The Child in Shock? Any Child With Shock Go Straight To Treatment Plan CKalichandren ArumugamNo ratings yet
- Pediatric OSCEs 2016 ModifiedDocument113 pagesPediatric OSCEs 2016 ModifiedAbdulKhaleq AlkadimiNo ratings yet
- Neonatal HypoglyDocument31 pagesNeonatal HypoglyAli FalihNo ratings yet
- SC GuidlinesDocument54 pagesSC GuidlinesShafaat HussainNo ratings yet
- Childhood EmergenciesDocument39 pagesChildhood EmergenciessharonoyemNo ratings yet
- Control of Diarrhoeal Diseases, Acute Diarrhoeal DiseasesDocument60 pagesControl of Diarrhoeal Diseases, Acute Diarrhoeal DiseasesSamarjeet KaurNo ratings yet
- Diarrhoea in ChildrenDocument22 pagesDiarrhoea in ChildrenSoujanya SharmaNo ratings yet
- Principles of Managing Severe Acute MalnutritionDocument31 pagesPrinciples of Managing Severe Acute MalnutritionMohammad Farouq OmarNo ratings yet
- Kwashior and MarasmusDocument17 pagesKwashior and Marasmuszuby_0302No ratings yet
- Group 5Document66 pagesGroup 5Cms CSUNo ratings yet
- Acute Gastroenteritis Presentation EDITEDV2Document49 pagesAcute Gastroenteritis Presentation EDITEDV2Sharmini RajagopalNo ratings yet
- Acute GastroenteritisDocument29 pagesAcute Gastroenteritisjinggalu100% (5)
- HT and PE Acute Diarrhea GIS 2022Document13 pagesHT and PE Acute Diarrhea GIS 2022Alfiyya nur marhdiyyahNo ratings yet
- World Health Organization (Who) Guidelines On Treatment of Diarrhea (2005)Document7 pagesWorld Health Organization (Who) Guidelines On Treatment of Diarrhea (2005)Tina AldabaNo ratings yet
- PretermDocument88 pagesPretermAhmed KitawNo ratings yet
- Imci PPT 6th ExamDocument50 pagesImci PPT 6th ExamGladys YaresNo ratings yet
- Stabilization CentreDocument64 pagesStabilization CentreShafaat HussainNo ratings yet
- Stabilization CentreDocument64 pagesStabilization CentreShafaat HussainNo ratings yet
- DiarrheaDocument17 pagesDiarrheaAchyut KanungoNo ratings yet
- Gastroenteritis: Faculty of Medicine University of North Sumatera Haji Adam Malik General Hospital Medan 2013Document24 pagesGastroenteritis: Faculty of Medicine University of North Sumatera Haji Adam Malik General Hospital Medan 2013Nithiyah ManiamNo ratings yet
- Stabilization CentreDocument64 pagesStabilization CentreShafaat HussainNo ratings yet
- Severe Acute Malnutrition and Fluid Management inDocument76 pagesSevere Acute Malnutrition and Fluid Management inBibsNo ratings yet
- Clinical Features: How Do Youbecome A Carrier of Malaria?Document6 pagesClinical Features: How Do Youbecome A Carrier of Malaria?Ma Sophia LimNo ratings yet
- Dehydration in ChildrenDocument24 pagesDehydration in ChildrenDani AsmareNo ratings yet
- Neonatal Protocol Hargeisa Group HospitalDocument27 pagesNeonatal Protocol Hargeisa Group HospitalAhmedNo ratings yet
- IMCI Revised For CHN 1 NEW 1st Sem 2022Document82 pagesIMCI Revised For CHN 1 NEW 1st Sem 2022Aech Euie100% (1)
- Protein Calorie MalnutritionDocument97 pagesProtein Calorie Malnutritionnshaikh56No ratings yet
- Management of MalnutritionDocument80 pagesManagement of MalnutritionAbdul HadiNo ratings yet
- DiarrheaDocument23 pagesDiarrheayadavmanas808No ratings yet
- CholeraDocument5 pagesCholerabishnu011978No ratings yet
- DIARHEADocument7 pagesDIARHEAahmedmuuseabokorNo ratings yet
- 08 Complicated MalariaDocument36 pages08 Complicated MalariaMwanja MosesNo ratings yet
- Hypoglycemia1 & FeedingDocument25 pagesHypoglycemia1 & FeedingMimo HemadNo ratings yet
- High Risk NeonateDocument102 pagesHigh Risk NeonateJaya Prabha100% (2)
- Approach To Acute Diarrhoea: Dr. Pankaj Kumar Singhal Govt. Medical College, KotaDocument43 pagesApproach To Acute Diarrhoea: Dr. Pankaj Kumar Singhal Govt. Medical College, KotaVandanaNo ratings yet
- Neonatal SepsisDocument20 pagesNeonatal SepsisJustine Nyangaresi100% (1)
- 14 Malnutrition 1Document21 pages14 Malnutrition 1Joy KirumbaNo ratings yet
- Hippo EM Foundations - Pediatric Emergencies Written SummaryDocument31 pagesHippo EM Foundations - Pediatric Emergencies Written Summarykaylawilliam01No ratings yet
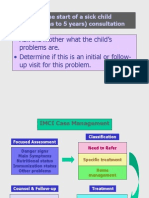
- Ask The Mother What The Child's Problems Are. - Determine If This Is An Initial or Follow-Up Visit For This ProblemDocument43 pagesAsk The Mother What The Child's Problems Are. - Determine If This Is An Initial or Follow-Up Visit For This ProblemJoereyConelNo ratings yet
- Fluid and Electrolyte TherapyDocument4 pagesFluid and Electrolyte TherapyKhirren RaoNo ratings yet
- Cholera Case Managment 1.3.23Document35 pagesCholera Case Managment 1.3.23Billy ManyadzaNo ratings yet
- Davidkamau ppt2Document40 pagesDavidkamau ppt2Jimmy MainaNo ratings yet
- NUTRITIONDocument12 pagesNUTRITIONgeofreymax9No ratings yet
- Group 5 Endocrine and Metabolic Complications of The Newborn SU 6.5Document13 pagesGroup 5 Endocrine and Metabolic Complications of The Newborn SU 6.5CHARLOTTE DU PREEZNo ratings yet
- Abnormal Midwifery: by Gladys M. BSN, KRCHNDocument352 pagesAbnormal Midwifery: by Gladys M. BSN, KRCHNMercy KeruboNo ratings yet
- CPG On Acute Infectious Diarrhea 2021Document42 pagesCPG On Acute Infectious Diarrhea 2021babbettemdNo ratings yet
- Abnormal Midwifery1 1Document352 pagesAbnormal Midwifery1 1Mary AndrewNo ratings yet
- Contact Details Name: Hospital Telephone:: Carnitine Transporter Deficiency (CTD) - Acute DecompensationDocument4 pagesContact Details Name: Hospital Telephone:: Carnitine Transporter Deficiency (CTD) - Acute DecompensationCaterina PrepelitaNo ratings yet
- The Treatment of Diarrhea: Skill LabDocument16 pagesThe Treatment of Diarrhea: Skill LabnovylatifahNo ratings yet
- Clinical Presentation and Case ManagementDocument34 pagesClinical Presentation and Case ManagementPatrick MukosoNo ratings yet
- DR - Salika Jayasundara (MO/SCBU) General Hospital - Kegalle Sri LankaDocument23 pagesDR - Salika Jayasundara (MO/SCBU) General Hospital - Kegalle Sri LankaAli FalihNo ratings yet
- Hypoglycemia, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandHypoglycemia, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Sample LNAP Template (Updated)Document24 pagesSample LNAP Template (Updated)roseannurakNo ratings yet
- Why Invest in NutritionDocument52 pagesWhy Invest in NutritionroseannurakNo ratings yet
- MBFW RequirementsDocument2 pagesMBFW RequirementsroseannurakNo ratings yet
- AidsDocument11 pagesAidsroseannurakNo ratings yet
- Letter of Intent - Calauag LGU For MBFW CertificationDocument2 pagesLetter of Intent - Calauag LGU For MBFW CertificationroseannurakNo ratings yet
- Final Ppan 2023 2028Document17 pagesFinal Ppan 2023 2028roseannurakNo ratings yet
- Template Equipment Inventory - General LunaDocument22 pagesTemplate Equipment Inventory - General LunaroseannurakNo ratings yet
- Sam CaseDocument17 pagesSam CaseroseannurakNo ratings yet
- Pob 2Document635 pagesPob 2roseannurakNo ratings yet
- Pob 4Document635 pagesPob 4roseannurakNo ratings yet
- INVENTORYDocument14 pagesINVENTORYroseannurakNo ratings yet
- Pob 3Document635 pagesPob 3roseannurakNo ratings yet
- Module 7 MKKDocument10 pagesModule 7 MKKroseannurakNo ratings yet
- FINAL - Strengthening of The LGU Nutrition Program Creation of LGU Nutrition OfficesDocument34 pagesFINAL - Strengthening of The LGU Nutrition Program Creation of LGU Nutrition Officesroseannurak100% (1)
- LNC FunctionalityDocument1 pageLNC FunctionalityroseannurakNo ratings yet
- Module 1Document42 pagesModule 1roseannurakNo ratings yet
- Module 4Document107 pagesModule 4roseannurakNo ratings yet
- Module 6ADocument176 pagesModule 6AroseannurakNo ratings yet
- Module 3Document36 pagesModule 3roseannurak100% (1)
- Module 5 BDocument15 pagesModule 5 BroseannurakNo ratings yet
- Module 2: Advancing Core Values and Skills of Nutrition Workers 1Document41 pagesModule 2: Advancing Core Values and Skills of Nutrition Workers 1roseannurak100% (1)
- Module 8Document6 pagesModule 8roseannurakNo ratings yet
- Module 2Document65 pagesModule 2roseannurakNo ratings yet
- Module 7.pptx FinalDocument38 pagesModule 7.pptx FinalroseannurakNo ratings yet
- DSP Survey Form 2022Document6 pagesDSP Survey Form 2022roseannurakNo ratings yet
- CDP SocialWorkshop MatrixDocument21 pagesCDP SocialWorkshop MatrixroseannurakNo ratings yet
- Local Health Board MeetingDocument1 pageLocal Health Board MeetingroseannurakNo ratings yet
- Health ReportDocument21 pagesHealth ReportroseannurakNo ratings yet
- General-Luna Elem Districtschool NS Baseline Consolidation Sy2023-2024Document99 pagesGeneral-Luna Elem Districtschool NS Baseline Consolidation Sy2023-2024roseannurakNo ratings yet
- Insulin Therapy: by Dr. Adithya PolavarapuDocument18 pagesInsulin Therapy: by Dr. Adithya Polavarapuadithya polavarapuNo ratings yet
- A Study of CIN-107 in Adults With Treatment-Resistant Hypertension - American College of CardiologyDocument2 pagesA Study of CIN-107 in Adults With Treatment-Resistant Hypertension - American College of CardiologynepalNo ratings yet
- ( (Drugs For Diabetes Mellitus) ) PDFDocument7 pages( (Drugs For Diabetes Mellitus) ) PDFMohamedYosefNo ratings yet
- Jurnal Glikosida FIXDocument5 pagesJurnal Glikosida FIXfiqriNo ratings yet
- DM - Satyanarayan TextbookDocument5 pagesDM - Satyanarayan TextbookSafa FatimaNo ratings yet
- Diagnostics 11 01714 v2Document14 pagesDiagnostics 11 01714 v2Biswaranjan SwainNo ratings yet
- Changing Patterns of Self-Management in Youth With Type I DiabetesDocument2 pagesChanging Patterns of Self-Management in Youth With Type I DiabetesMAHESH KOUJALAGINo ratings yet
- DB 151028Document11 pagesDB 151028aminm23kNo ratings yet
- DM Related For JCIDocument3 pagesDM Related For JCIJohn Nine ErispeNo ratings yet
- Gabriel - Shaibi@asu - Edu: Abriel Haibi HDocument22 pagesGabriel - Shaibi@asu - Edu: Abriel Haibi Hapi-306659854No ratings yet
- AL CIERRE DE Julio Del 2021: Barra COD AlfabetaDocument2 pagesAL CIERRE DE Julio Del 2021: Barra COD AlfabetaBrian Javier GomezNo ratings yet
- Endo Drug StudyDocument37 pagesEndo Drug StudylorreaNo ratings yet
- Hubungan Kualitas Tidur Dengan Kadar Glukosa Darah Pada Pasien Diabetes Mellitus Tipe IiDocument8 pagesHubungan Kualitas Tidur Dengan Kadar Glukosa Darah Pada Pasien Diabetes Mellitus Tipe IiIyas SalwaniNo ratings yet
- chap06.ppt-BODY COMPOSITIONDocument29 pageschap06.ppt-BODY COMPOSITIONJeremy Bio FangonNo ratings yet
- Case Study 2Document2 pagesCase Study 2api-547174770100% (1)
- Diabetes: EndocrinologyDocument8 pagesDiabetes: EndocrinologyZhanyar Omer Mustafa F210050No ratings yet
- Diabetes Mellitus Forecast Using Artificial Neural Network AnnDocument5 pagesDiabetes Mellitus Forecast Using Artificial Neural Network AnnDivya SinghNo ratings yet
- Dr. MD Rezaul Karim Thesis Prevalance of Micro and Macrovascular Complications in Newly DetecDocument22 pagesDr. MD Rezaul Karim Thesis Prevalance of Micro and Macrovascular Complications in Newly Detecrezalata38100% (1)
- Diabetes Knowledge, Attitude, and Practice Among Type 2 Diabetes Mellitus Patients in Kuala Muda District, Malaysia - A Cross-Sectional StudyDocument7 pagesDiabetes Knowledge, Attitude, and Practice Among Type 2 Diabetes Mellitus Patients in Kuala Muda District, Malaysia - A Cross-Sectional Studymaryam farrukhNo ratings yet
- BSN 3C NCM112 Diabetic Kidney Disease Case Study FinalDocument85 pagesBSN 3C NCM112 Diabetic Kidney Disease Case Study FinalMarjune DimayugaNo ratings yet
- Immersion Midpoint Reflective JournalDocument2 pagesImmersion Midpoint Reflective Journalapi-496376311No ratings yet
- RBS - Random Blood Sugar PDFDocument4 pagesRBS - Random Blood Sugar PDFKrishna Faith P. DelaraNo ratings yet
- Insulin and Its Preparation: DR C.Sadhana Final Year MD Pharmacology Department of Pharmacology SBMCHDocument62 pagesInsulin and Its Preparation: DR C.Sadhana Final Year MD Pharmacology Department of Pharmacology SBMCHP Vinod KumarNo ratings yet
- Study PlanDocument4 pagesStudy Planuriaswalliser.frnb1.04.4No ratings yet
- Risk factors of diabetic retinopathy and vision threatening diabetic retinopathy and vision threatening diabetic retinopaty based on diabetic retinopathy screening program in greater bandung, west java.astriDocument14 pagesRisk factors of diabetic retinopathy and vision threatening diabetic retinopathy and vision threatening diabetic retinopaty based on diabetic retinopathy screening program in greater bandung, west java.astriSi PuputNo ratings yet
- DM CasesDocument8 pagesDM CasesMelekNo ratings yet
- Prevalence of Refractive Errors in Type 2 Diabetic Patients in Northern IndiaDocument8 pagesPrevalence of Refractive Errors in Type 2 Diabetic Patients in Northern IndiaRagni MishraNo ratings yet