Presentation 2
Presentation 2
Download as pptx, pdf, or txt
You might also like
- Borer (2013) Advanced Exercise Endocrinology PDFDocument272 pagesBorer (2013) Advanced Exercise Endocrinology PDFNicolás Bastarrica100% (1)
- Grade 10 EndocrineDocument14 pagesGrade 10 EndocrineHashtag NileNo ratings yet
- Lect 5Document26 pagesLect 5eslambasuony98No ratings yet
- Management of Thyroid DisordersDocument119 pagesManagement of Thyroid DisordersmatthiaspaullowNo ratings yet
- Therapeutics: Thyroid DisordersDocument24 pagesTherapeutics: Thyroid DisordersSharas FarhadNo ratings yet
- Lecture (1) - THDocument34 pagesLecture (1) - THyoussef hossamNo ratings yet
- Thyroid DisorderDocument60 pagesThyroid DisorderThe AbyssinicansNo ratings yet
- Lecture (2) TherapDocument25 pagesLecture (2) Therapyoussef hossamNo ratings yet
- PATIENT WITH ENDOCRINE DYSFUNCTION THYROID .pptx1Document52 pagesPATIENT WITH ENDOCRINE DYSFUNCTION THYROID .pptx1sembakarani thevagumaranNo ratings yet
- Thyroid DiseaseDocument36 pagesThyroid Diseasejozemomo206No ratings yet
- Lec#15+16 Thyroid DisordersDocument82 pagesLec#15+16 Thyroid DisordersKhaldoun AlmomaniNo ratings yet
- 15 2020 Thyroid - Antithyroid Drugs - SlidesDocument26 pages15 2020 Thyroid - Antithyroid Drugs - Slidesالبيان البيانNo ratings yet
- Thyroid DiseaseDocument72 pagesThyroid Diseaseluna zeidNo ratings yet
- Thyroid DisordersDocument34 pagesThyroid DisordersAbdulhameed Mohamed100% (1)
- Thyroid and Antithyroid Agent-VDocument60 pagesThyroid and Antithyroid Agent-VVine100% (1)
- THYROIDECTOMYDocument53 pagesTHYROIDECTOMYlolelanji NakambaNo ratings yet
- Drug Management of Thyroid DiseaseDocument22 pagesDrug Management of Thyroid DiseaseHassan.shehri100% (6)
- Thyroid Disorder: Meaza Bulbula (M. Pharm)Document61 pagesThyroid Disorder: Meaza Bulbula (M. Pharm)Ko MhdNo ratings yet
- Thyroid Hormones & DrugsDocument51 pagesThyroid Hormones & DrugsSUTHANNo ratings yet
- Thyroid and Antithyroid DrugsDocument51 pagesThyroid and Antithyroid DrugsToufiq Imam Zuboraz 1821982649No ratings yet
- Thyroid Disorders: Aromokunola Boluwaji Peter (B.Pharm, Ife)Document18 pagesThyroid Disorders: Aromokunola Boluwaji Peter (B.Pharm, Ife)boluwaji aromokunolaNo ratings yet
- Hyperthyroidism: by TemesgenDocument33 pagesHyperthyroidism: by TemesgenTemesgen100% (2)
- Lesson 6 Thyroid and Antithyroid DrugsDocument28 pagesLesson 6 Thyroid and Antithyroid DrugstheintrovNo ratings yet
- Thyroid and Antithyroid Drugs... HaftomDocument40 pagesThyroid and Antithyroid Drugs... Haftomkaleab AlemayehuNo ratings yet
- 2 TSHDocument7 pages2 TSHNashat SaadiNo ratings yet
- 02 Lecture 10 Anti-Thyroid Drugs (DR Thatcher Pod Pharm 2022)Document36 pages02 Lecture 10 Anti-Thyroid Drugs (DR Thatcher Pod Pharm 2022)sahilaminNo ratings yet
- Thyroid DisordersDocument62 pagesThyroid Disorderslibentadesse57No ratings yet
- Thyroid and Parathyroid GlandsDocument133 pagesThyroid and Parathyroid GlandsmunafalmahdiNo ratings yet
- Interpretation of Laboratory Thyroid Function Tests: The "Hidden" Health ProblemDocument38 pagesInterpretation of Laboratory Thyroid Function Tests: The "Hidden" Health Problemalanoud.877No ratings yet
- Thyroid PresentationDocument38 pagesThyroid Presentation천사자No ratings yet
- Thyroid Gland L-Thyroxine (T4) Vs Triiodothyronine (T3) : Follicular CellsDocument7 pagesThyroid Gland L-Thyroxine (T4) Vs Triiodothyronine (T3) : Follicular CellsPrincess Noreen SavellanoNo ratings yet
- Thyroid and ParathyroidDocument29 pagesThyroid and Parathyroidpranutan739No ratings yet
- Management and Medications in Thyroid Strom and Myxoedema ComaDocument41 pagesManagement and Medications in Thyroid Strom and Myxoedema ComaBhavesh kunvarNo ratings yet
- Thyroid Gland Diseases in ChildrenDocument29 pagesThyroid Gland Diseases in ChildrenadinayNo ratings yet
- Hyperthyroidism and HypothyroidismDocument59 pagesHyperthyroidism and HypothyroidismJun AmaroNo ratings yet
- Module I 2 - Thyroid Gland DisordersDocument43 pagesModule I 2 - Thyroid Gland Disordersaysha jasim100% (1)
- Theme 2: Thyroid Diseases: Study GoalsDocument9 pagesTheme 2: Thyroid Diseases: Study GoalsOlesyaNo ratings yet
- Sophie Keyte Bvms (Hons) Mvetmed (Dist) Fhea Dipacvim Mrcvs Sophie - Keyte@Bristol - Ac.UkDocument24 pagesSophie Keyte Bvms (Hons) Mvetmed (Dist) Fhea Dipacvim Mrcvs Sophie - Keyte@Bristol - Ac.UkStefana UrsuNo ratings yet
- Makalah Case 2 Grave DiseaseDocument8 pagesMakalah Case 2 Grave Diseasesalsabila firdausiaNo ratings yet
- Thyroid CrisisDocument34 pagesThyroid CrisisRidyah Ning TyasNo ratings yet
- Thyroid StormDocument3 pagesThyroid StormSuprit SnNo ratings yet
- Thyroid and Antithyroid DrugsDocument71 pagesThyroid and Antithyroid DrugsDr. Lokeshwar ChaurasiaNo ratings yet
- Endocrinologic DisordersDocument80 pagesEndocrinologic Disordersfanuiel mandefroNo ratings yet
- Trachea: Thyroid Agents Thyroid Gland Is Located in The Middle of The Neck and SurroundsDocument10 pagesTrachea: Thyroid Agents Thyroid Gland Is Located in The Middle of The Neck and SurroundsMIR SARTAJNo ratings yet
- Hyperthyroidism NotesDocument17 pagesHyperthyroidism NotesAthira BabuNo ratings yet
- Thyroid & Anti-Thyroid DrugsDocument59 pagesThyroid & Anti-Thyroid DrugsNiranjanNo ratings yet
- Diagnosis and Management of Hyperthyroidism, A Rational ApproachDocument35 pagesDiagnosis and Management of Hyperthyroidism, A Rational ApproachANCHAL SHARMANo ratings yet
- Thyroiddisease 190216062020Document42 pagesThyroiddisease 190216062020Manikandan Vp100% (1)
- THYROTOXICOSISDocument20 pagesTHYROTOXICOSISfig8fashion1No ratings yet
- Thyroid PharmacologyDocument26 pagesThyroid PharmacologyVikrant GholapNo ratings yet
- 3 ThyroidDocument60 pages3 ThyroidyeabsraNo ratings yet
- Thyroid Anti-Thyroid DrugsDocument56 pagesThyroid Anti-Thyroid DrugsRida WaseemNo ratings yet
- 2.tyroid Gland DrsDocument55 pages2.tyroid Gland DrsAddis KusseNo ratings yet
- ThyrotoxicosisDocument105 pagesThyrotoxicosisAli Murtaza Abbas100% (1)
- Thyroid Emergencies-Dr. AM IyagbaDocument13 pagesThyroid Emergencies-Dr. AM IyagbaDr. Amb. Monday ZaccheausNo ratings yet
- Hypothyroid in Pregnancy Andi CakraDocument32 pagesHypothyroid in Pregnancy Andi CakraCakraEkky100% (1)
- Thiroid DisordersDocument11 pagesThiroid Disordersرعد النميريNo ratings yet
- Thyroid Disorders: Dr. Lubna DwerijDocument52 pagesThyroid Disorders: Dr. Lubna DwerijNoor MajaliNo ratings yet
- U World Endocrine FinalDocument19 pagesU World Endocrine FinalrpereiracruzNo ratings yet
- Thyroid and Parathyroid AgentsDocument28 pagesThyroid and Parathyroid AgentsMary Faith Kiat-ongNo ratings yet
- Hyperthyroidism, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandHyperthyroidism, A Simple Guide To The Condition, Treatment And Related ConditionsRating: 2 out of 5 stars2/5 (2)
- Thyroid FunctionDocument2 pagesThyroid FunctionSm Bikash Kumar MohonNo ratings yet
- Jähf  F, Áwgh Ikædu¡F Ey Ga¡F M Á Kyu Jiz Úy Fÿ: Brašglhj M.Ï.M.Â.K.F M Á¡F Koî F L FÿDocument4 pagesJähf  F, Áwgh Ikædu¡F Ey Ga¡F M Á Kyu Jiz Úy Fÿ: Brašglhj M.Ï.M.Â.K.F M Á¡F Koî F L Fÿjnizamudeen6958No ratings yet
- Disorders of The Ovaries 2Document92 pagesDisorders of The Ovaries 2rerenNo ratings yet
- Feedback Mechanism Animal PhysiologyDocument27 pagesFeedback Mechanism Animal PhysiologyBacon ZenNo ratings yet
- Final Endocrinology 2024Document143 pagesFinal Endocrinology 2024anushkagupta11akjNo ratings yet
- General Medicine Lec4 Adrenal GlandsDocument9 pagesGeneral Medicine Lec4 Adrenal GlandsAli MONo ratings yet
- Endocrine System TransDocument21 pagesEndocrine System TransMa. Mil Adrianne PamaNo ratings yet
- Steroid AbuseDocument7 pagesSteroid Abuseapi-400575655No ratings yet
- Pituitary DisordersDocument65 pagesPituitary Disordersgema disiyuna100% (2)
- Endocrine Patient SimulationsDocument15 pagesEndocrine Patient SimulationsrebbiegNo ratings yet
- Endocrine System NCM116 Midterm - XCDocument4 pagesEndocrine System NCM116 Midterm - XCXia CabilloNo ratings yet
- List of Endocrine DiseasesDocument6 pagesList of Endocrine DiseasesPreethiHonavarNo ratings yet
- Endocrine System and AdolescenceDocument22 pagesEndocrine System and Adolescencenia tombriNo ratings yet
- Endocrine MCQDocument10 pagesEndocrine MCQBadr DihamNo ratings yet
- Medicine Quiz 11 - AMC Question Bank - TextDocument37 pagesMedicine Quiz 11 - AMC Question Bank - TextbuffettmorandiniNo ratings yet
- Sheehan's Syndrome PathophysiologyDocument2 pagesSheehan's Syndrome PathophysiologyirismgallNo ratings yet
- J of Obstet and Gynaecol - 2021 - Oride - Reproductive Prognosis of Patients With Hypogonadotropic HypogonadismDocument8 pagesJ of Obstet and Gynaecol - 2021 - Oride - Reproductive Prognosis of Patients With Hypogonadotropic Hypogonadismaarthisjayraj91No ratings yet
- BALOTARIODocument8 pagesBALOTARIOYaretz BastidasNo ratings yet
- Urine Formation and ExcretionDocument12 pagesUrine Formation and ExcretionNilesh Sawant100% (1)
- Haematology Test Name Result Units Reference IntervalsDocument2 pagesHaematology Test Name Result Units Reference Intervalssk hitechlabNo ratings yet
- Lect 9 Parathyroid Gland-1Document30 pagesLect 9 Parathyroid Gland-1warda farooqNo ratings yet
- DLP Biology 10 CotDocument7 pagesDLP Biology 10 CotCarl AnthonyNo ratings yet
- Congenital Hypothyroidism From MedscapeDocument11 pagesCongenital Hypothyroidism From MedscapeAgustin IskandarNo ratings yet
- Assessment and Management of Patients With Endocrine DisordersDocument91 pagesAssessment and Management of Patients With Endocrine DisordersAirme Raz AlejandroNo ratings yet
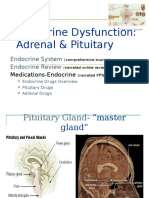
- Endocrine Dysfunction: Adrenal & Pituitary: Endocrine System Endocrine ReviewDocument102 pagesEndocrine Dysfunction: Adrenal & Pituitary: Endocrine System Endocrine ReviewCalimlim KimNo ratings yet
- Free T3Document1 pageFree T3Jason Roy Edward NathanNo ratings yet
- SCIENCE Role of Hormone in Female and Male Reproductive SystemDocument8 pagesSCIENCE Role of Hormone in Female and Male Reproductive SystemJasmineNo ratings yet
- Chemical Coordination MCQDocument6 pagesChemical Coordination MCQRavi Kumar100% (2)