JSLHR
Research Article
Clinical Outcomes Following LanguageSpecific Attention Treatment Versus
Direct Attention Training for Aphasia:
A Comparative Effectiveness Study
Richard K. Peach,a Katherine M. Beck,a Michelle Gorman,a and Christine Fishera
Purpose: This study was conducted to examine the
comparative effectiveness of 2 different approaches,
1 domain-specific and the other domain-general, to language
and attention rehabilitation in participants with strokeinduced aphasia. The domain-specific treatment consisted
of language-specific attention treatment (L-SAT), and the
domain-general treatment consisted of direct attention
training (DAT) using the computerized exercises included in
Attention Process Training-3 (Sohlberg & Mateer, 2010).
Method: Four individuals with mild–moderate aphasia
participated in this study. A randomized controlled cross-over
single-subject design was used to assess the effectiveness
of the 2 treatments administered in this study. Treatment
outcomes were evaluated in terms of participants’ task
performance for each program, standardized language
and attention measures, tests of functional abilities, and
patient-reported outcomes.
Results: Visual comparisons demonstrated linear
improvements following L-SAT and variable patterns following
DAT. Omnibus effect sizes were statistically significant for
9 of the 13 L-SAT tasks. The weighted standardized effect
sizes for posttreatment changes following L-SAT ranged
from small to large, with the exception of 1 task. The
average group gain following DAT was 5%. The Western
Aphasia Battery–Revised Aphasia Quotients (Kertesz, 2007)
demonstrated reliable improvements for 3 of the 4 participants
following L-SAT, whereas only 1 of the participants improved
reliably following DAT. The margins of improvements in
functional language were substantially larger following
L-SAT than DAT. Performance on the Test of Everyday
Attention improved significantly for 2 participants following
L-SAT and for 1 participant following DAT on selected Test
of Everyday Attention (Robertson, Ward, Ridgeway, &
Nimmo-Smith, 1994) subtests. Patient-reported outcomes
for communication and attention following treatment favored
L-SAT compared to DAT.
Conclusions: The results support the view that attention
is allocated in ways that are particular to specific tasks rather
than as a general resource that is allocated equivalently to all
processing tasks. Domain-specific treatment for language
deficits due to attentional impairment appears to be a
suitable, if not preferable, approach for aphasia rehabilitation.
Supplemental Material: https://doi.org/10.23641/asha.
8986427
I
Pabón, 1964; Wepman, Jones, Bock, & Van Pelt, 1960).
However, Wepman’s interests in the effects of language
disturbances on a patient’s thought processes led him to
argue for an indirect, more contextualized approach to language treatment (Wepman, 1972), whereas Schuell, who
conceptualized aphasia as a multimodal, unidimensional
language disturbance based on a primary deficit of auditory
language, advocated for direct, intensive auditory stimulation as the preferred approach to aphasia rehabilitation
(Schuell & Jenkins, 1959; see also Coelho, Sinotte, & Duffy,
2008). These methods have constituted some of the most
frequently used approaches to aphasia therapy (e.g., Peach,
1993, 2001) while their application has been extended subsequently to more conversational contexts (e.g., Davis,
n aphasia rehabilitation, the theoretical underpinnings
of the disorder guide the methods that have been developed and tested for the treatment of the condition.
For example, two contemporaries in early clinical aphasiology, Joseph Wepman and Hildred Schuell, argued for
direct language stimulation to ameliorate the language deficits of people with aphasia (Schuell, Jenkins, & Jiménez-
a
Department of Communication Disorders and Sciences, Rush
University Medical Center, Chicago, IL
Correspondence to Richard K. Peach: richard_k_peach@rush.edu
Editor-in-Chief: Sean Redmond
Editor: Sarah Wallace
Received December 19, 2018
Revision received February 17, 2019
Accepted April 1, 2019
https://doi.org/10.1044/2019_JSLHR-L-18-0504
Disclosure: The authors have declared that no competing interests existed at the time
of publication.
Journal of Speech, Language, and Hearing Research • Vol. 62 • 2785–2811 • August 2019 • Copyright © 2019 American Speech-Language-Hearing Association
Downloaded from: https://pubs.asha.org Richard Peach on 08/16/2019, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions
2785
�2005; Difrancesco, Pulvermüller, & Mohr, 2012; Peach &
Wong, 2004).
Some treatment approaches have been based on representational accounts of language impairment following
aphasia, that is, how aphasia impairs the patient’s ability
to construct syntactic or semantic representations (see, e.g.,
Grodzinsky, 1986; Rogers, Patterson, Jefferies, & Ralph,
2015). The corresponding treatment approaches to improve
syntactic (e.g., Treating Underlying Forms [Thompson &
Shapiro, 2005]; message-level treatment [Peach & Wong,
2004]) or semantic abilities (e.g., semantic feature analysis
[Boyle, 2004; Boyle & Coelho, 1995; Peach & Reuter, 2010];
semantic complexity training [Kiran, 2007; Kiran &
Thompson, 2003]; Verb Network Strengthening Treatment
[Edmonds, Nadeau, & Kiran, 2009]) exhibit strong evidence for their efficacy and thus have widespread usage.
Alternatively, a number of processing-based approaches
have been used for aphasia treatment. Unlike representational approaches, these approaches view the disorder as a
problem in the patient’s ability to access his or her preserved
linguistic knowledge during language processing. Some examples of these methods include syntactic mapping treatment (Jacobs & Thompson, 2000; Rochon, Laird, Bose, &
Scofield, 2005), semantic and phonological cueing treatments (Conroy, Sage, & Lambon Ralph, 2009; Wambaugh,
Cameron, Kalinyak-Fliszar, Nessler, & Wright, 2004), semantic and phonological processing treatments (Kendall,
Oelke, Brookshire, & Nadeau, 2015; Kiran, Sandberg, &
Abbot, 2009; Peach, 1996; Raymer & Ellsworth, 2002), and
contextual repetition priming (Martin, Fink, Renvall, &
Laine, 2006; Renvall, Laine, & Martin, 2005).
Recently, a number of treatment approaches have been
based on resource theory. Unlike the approaches above,
however, these approaches assume that the language impairment in aphasia results from difficulty in using cognitive
resources (e.g., attention, memory) for the comprehension
or production of language (Code, 2018). Representative
models emphasize the effects of deficient attentional processing (Hula & McNeil, 2008; McNeil et al., 2004; Peach,
Newhoff, & Rubin, 1993; Peach, Rubin, & Newhoff, 1994),
auditory–verbal short-term memory (Kalinyak-Fliszar,
Kohen, & Martin, 2011; Minkina, Rosenberg, KalinyakFliszar, & Martin, 2017; Peach, 1987; Salis, 2012), and
working memory (Henderson, Kim, Kintz, Frisco, & Wright,
2017; Martin, Kohen, Kalinyak-Fliszar, Soveri, & Laine,
2012; Salis, Hwang, Howard, & Lallini, 2017; Wright &
Shisler, 2005) on language processing. Improving these
deficiencies, therefore, is the goal of methods that target
these resources in treatment.
Attention Treatment for Aphasia
Of the cognitive resources that have been targeted in
aphasia rehabilitation, attention, perhaps, has received the
most consideration (Connor, Albert, Helm-Estabrooks, &
Obler, 2000). Helm-Estabrooks, Connor, and Albert (2000)
treated two patients with mixed nonfluent aphasia (PWA)
using nonlinguistic sustained attention tasks followed by
2786
selective and alternating attention tasks, including symbol
cancellation, trail making, repeated graphomotor patterns,
auditory continuous performance, and card sorting, to improve auditory comprehension deficits. Improvements of 6
and 13 percentile points on the Boston Diagnostic Aphasia
Examination (Goodglass & Kaplan, 1983) were observed
immediately after the treatment program, with slight declines
at approximately six to seven months posttreatment. Kohnert
(2004) attempted to improve response speed and accuracy
in a patient with transcortical motor aphasia by administering
a series of nonverbal attention activities, including card sorting, written single-digit computations, and visual letter and
number searches. Tasks from a high-level, computer-based
training program were also administered (e.g., discrimination
between target and nontarget icons in alternating quadrants
of the computer screen). Gains were observed across all
treatment tasks followed by modest improvements in some
language tasks. Ramsberger (2005) also reported the outcome of a treatment study using a computer-based program
to improve attention/executive functioning, linguistic processing, and conversational success for a patient with borderline fluent aphasia. The patient showed improvement
on all of the training tasks, and the treatment appeared to
generalize to two attention tests as well. Importantly, the
patient’s ability to convey main ideas in conversation improved dramatically.
A number of studies have administered either Attention
Process Training–II (APT-II; Sohlberg, Johnson, Paule,
Raskin, & Mateer, 2001) or APT-3 (Sohlberg & Mateer,
2010) to individuals with aphasia to address their language
impairments. Both programs are commercially available and
designed to address attentional deficits in individuals with
acquired brain injury. Coelho (2005) administered APT-II
to a 50-year-old woman with chronic aphasia (10 months
postonset of stroke) to improve reading comprehension and
reading rate. Reading comprehensions scores, based on responses to comprehension questions regarding magazine
articles, improved from approximately 40%–60% to 83%
accuracy following treatment. Reading rate (words per minute) remained variable throughout treatment. Posttreatment
gains on two reading batteries provided support for improved
reading outcomes secondary to this program. Sinotte and
Coelho (2007) replicated Coelho’s study with a 60-year-old
woman with mild anomic aphasia 6 months postonset of a
left frontal hemorrhagic stroke. Following 16 sessions of
APT-II over a 5-week period, few changes in reading comprehension accuracy or reading rate were observed. Murray,
Keeton, and Karcher (2006) administered APT-II to a
57-year-old man with chronic, mild conduction aphasia
and deficits in repetition, high-level auditory comprehension, language, and working memory. Mildly impaired
attention for timed tasks was also observed. After more
than 50 hr of training, the patient demonstrated faster response latencies to a paragraph listening task, but no other
improvements in auditory comprehension. Murray et al. concluded that structured attention programs such as APT-II
may not provide a viable approach to treating attention
problems in patients with aphasia.
Journal of Speech, Language, and Hearing Research • Vol. 62 • 2785–2811 • August 2019
Downloaded from: https://pubs.asha.org Richard Peach on 08/16/2019, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions
�Lee and Sohlberg (2013) administered APT-3 to treat
reading comprehension in a single-subject design study with
four participants demonstrating mild–moderate chronic
aphasia. APT-3 combines direct attention training (DAT; as
in APT-II) with metacognitive training. Despite the modest
results obtained previously with this approach, the authors
hypothesized that the addition of metacognitive instruction
would improve resource allocation and, therefore, the reading comprehension of their participants with aphasia. Participants completed a maze reading task in which they select
a target word from three choices in parentheses to replace
missing words within each passage. The task is reported to
be sensitive to the working memory and attentional demands
required for reading comprehension. Two of the four participants demonstrated small improvements in maze reading
scores during the intervention phase, although a rising trend
during baseline for one of the participants made the source
of the improvement uncertain. Small gains on a standardized
reading test were also observed for these two participants.
Lee, Sohlberg, Harn, Horner, and Cherney (2018)
replicated the Lee and Sohlberg (2013) study, but with six
participants presenting with mild aphasia, impairments in
attention and/or working memory (as suggested by standardized testing), and complaints of reading difficulty. Also, the
metacognitive facilitation component of APT-3 was expanded to include individualized instruction to promote
generalization of self-monitoring to reading. The results
suggested an effect between APT-3 and maze reading for
three of the six participants, as indicated by visual analysis
of the data plots and Tau-U effect sizes. However, participants who adopted metacognitive strategies performed
better following treatment than those who did not. The authors concluded that APT-3 has the potential to improve
reading in participants with aphasia. Yet the design of this
study leaves open to question which component of the treatment, DAT or metacognitive strategy instruction, was the
more effective for achieving the observed outcomes.
Domain-Specific Versus Domain-General
Attention Training
All of the treatment studies reported above utilized
domain-general approaches for aphasia rehabilitation, that
is, treatment that targeted a variety of cognitive processes
to improve language. The alternative to such an approach
is a domain-specific approach, that is, one that focuses on
and exposes participants to highly practical tasks (e.g., language) to increase generalization (Pella, Kendra, Hill, &
Gouvier, 2008). The relative contributions of domain-general
or domain-specific processes for language processing are a
topic of continuing discussion. Recent reviews raise questions
about the interaction between domain-specific regions for language processing and large-scale domain-general systems
(Fedorenko & Thompson-Schill, 2014; Hartwigsen, 2018).
How these domain-general processes contribute to language
processing and “whether they are even necessary for…natural, everyday language” are uncertain (Campbell & Tyler,
2018, p. 132). According to Campbell and Tyler (2018),
“domain-general regions may be active during these tasks
because they are contributing to language processing or,
more likely, because they are contributing to general attention and memory demands of the task” (p. 132).
Despite the modest improvements reported in the
previous treatment studies, it has been suggested that
domain-general attentional approaches to language intervention result in poor outcomes (Rohling, Faust, Beverly,
& Demakis, 2009). Other studies discourage the use of
decontextualized computer-based attentional tasks, including APT, that address domain-general processes because
of a lack of demonstrated impact on everyday attentional
functions (Loetscher & Lincoln, 2013; Ponsford et al., 2014;
Zickefoose, Hux, Brown, & Wulf, 2013).
Alternatively, some researchers (see, e.g., Simonet, von
Roten, Spierer, & Barral, 2019) have argued that treatment
for attention deficits should require specific training for the
activities to which the training is expected to generalize.
Sturm, Willmes, Orgass, and Hartje (1997) demonstrated
that specific attention functions improve in patients with localized vascular lesions only when specific training is received
for that function. In this study, computer-based programs
were used to train the intensity (alertness, vigilance) and selectivity (selective and divided attention) aspects of attention.
Even when patients demonstrated deficits in both domains
of intensity or selection, improvements were only noted for
the single domain that received training. This was particularly evident for the intensity aspects of attention. In a
follow-up study, Sturm et al. (2003) administered the attention training programs to a participant group composed
of individuals with both traumatic brain injury and vascular
brain damage. A baseline phase was included to control for
spontaneous recovery, and participants received treatment for
only one of their impaired attention functions. The results
demonstrated comparable training effects in both groups for
specific training, not only for the intensity aspects of attention
but also for divided attention. Specific attention training for
alertness was also found to contribute to reorganization
of the right-hemisphere functional network known to subserve the alertness domain in healthy subjects. Similar
reorganization was not observed for patients with righthemisphere brain damage who received nonspecific (memory)
training for alertness (Sturm et al., 2004).
Park and colleagues (Park & Barbuto, 2005; Park &
Ingles, 2001; Park, Proulx, & Towers, 1999) found no evidence to support APT for remediating impaired attention
functions (e.g., sustained, selective, divided, and alternating
attention) but did conclude that it results in learning of
specific skills. This is consistent with recent results reported
by Peers et al. (2018), who found that a group of 23 participants with brain damage improved significantly on a
working memory outcome measure following working
memory training but not on a series of selective attention
tasks, whereas performance improved on attentional outcome measures following selective attention training but
not following working memory training. Furthermore, Park
and colleagues found that attention treatments that focus
on learning or relearning of specific skills that are important
Peach et al.: Language-Specific Attention Treatment for Aphasia
Downloaded from: https://pubs.asha.org Richard Peach on 08/16/2019, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions
2787
�to desired outcomes or behaviors having functional consequences resulted in significant improvement. Curran, Hussain,
and Park (2001, as cited in Park & Barbuto, 2005) found
that patients with mild cognitive impairment following
stroke learned novel naturalistic actions (goal-directed activities that require the production of several actions in a
particular order that cannot be learned prior to instruction,
e.g., preparing an unfamiliar recipe) more effectively when
the trainer verbally described the action while demonstrating it than when no verbal description accompanied the
demonstration. The authors hypothesized that the verbal
descriptions facilitated learning of the actions by enabling
the patients to develop a more accurate conceptual representation of the novel actions. It may also be, however, that
the verbal descriptions directed the patients’ attention to
the relevant environmental information and, in this way,
focused attention to facilitate the development of mental
representations for these actions.
Many of these investigators have called for further
exploration into the generalization of specific training effects to everyday functions relying on different aspects of
attention. With regard to language training, this requires a
consideration of the ways that specific linguistic processes
recruit select attentional operations in the service of language. That is, treatment for language disorders due to
attentional impairments might be better served by addressing the underlying attentional deficits that influence specific linguistic operations. That most previous treatment
studies of language and attentional impairments have
not done this might provide one explanation for the modest outcomes that have been observed. This requires an
analysis of some of the ways that language operates as an
attention director. For example, Crosson and colleagues
(Crosson & Cohen, 2012; Crosson et al., 2007; Dotson
et al., 2008) described two treatments manipulating attention and intention during confrontation naming that,
unlike the previously reported studies, produced robust
improvements in participants with moderate and severe
word-finding deficits.
Peach et al. (Peach, 2012; Peach, Schenk, Nathan, &
Beck, 2018) developed the framework for a domain-specific
program for the remediation of language disorders due to
attentional impairment (language-specific attention treatment [L-SAT]). The approach is based on five principles:
(a) train attentional focus and resource management for
language, (b) increase attentional demands, (c) automatize
attentional recruitment for language, (d) engage undamaged
attentional mechanisms in the nondominant hemisphere,
and (e) incorporate linguistic devices that require controlled
attention. A preliminary analysis of the results obtained
from four participants with aphasia for this treatment program provided evidence for improved language and attention but only for patients with aphasia having no greater
than a moderate degree of attentional impairment (Peach,
Nathan, & Beck, 2017). Based on these findings, the authors
concluded that greater scrutiny was warranted regarding
the effectiveness of L-SAT for stimulating attentional processing and language skills in people with aphasia.
2788
Purpose
Given the varied opinions, approaches, and results
that have been reported regarding attention rehabilitation,
especially as it relates to attention-related language deficits
following aphasia, this study was conducted to examine
the comparative effectiveness of two diverging attentional
approaches to language rehabilitation in participants
with stroke-induced aphasia. One approach consisted of
a domain-general approach, whereas the other utilized a
domain-specific approach. We assessed the clinical outcomes
associated with these treatments using multiple procedures at a variety of disability levels, including (a) statistical
and visual analyses to measure the participants’ responses
to each treatment, (b) standardized test scores to examine
the effects of each treatment on the participants’ language
and attention abilities, (c) functional tests of language and
attention to assess the impact of each treatment on everyday
abilities, and (d) patient-reported outcome scales to assess
the participants’ own views of the impact of each treatment on their language and attentional abilities.
Based on the modest results obtained previously using
domain-general approaches to the treatment of language
deficits following aphasia and the relatively stronger results
in cognitive training observed following domain-specific
methods, we hypothesized that the specific skills approach
to improving attention for language would result in more
desirable outcomes than a domain-general attentional approach for treating language deficits following aphasia.
Method
Participants
This study was approved by the institutional review
board of Rush University Medical Center (RUMC). A convenience sample consisting of four right-handed individuals
(three men, one woman) with an average age of 62 years
(SD = 17.0, range: 39–80 years) and an average education
of 15 years (SD = 2.58, range: 12–18 years) participated in
this study. They included two White and two Black participants who were recruited from RUMC and were paid for
their participation in the study. All participants were monolingual speakers of English. All participants reported adequate hearing and had adequate near vision as determined
by a brief vision screening (Schneider, 2002). No participant
demonstrated a history of alcohol or substance abuse or
psychiatric difficulties.
All participants had a documented, previous diagnosis of aphasia from a single left-hemisphere stroke. Three
of the participants had been enrolled previously in speechlanguage treatment; the treatment provided in this study
was the first exposure to speech-language treatment for the
remaining participant (P2). All participants had an Aphasia Quotient (AQ) below 93.8 on the Western Aphasia
Battery–Revised (WAB-R; Kertesz, 2007), indicating the
presence of aphasia. Aphasia severity was mild–moderate.
Based on the profiles obtained from the WAB-R, all participants demonstrated fluent aphasia, although one (P3)
Journal of Speech, Language, and Hearing Research • Vol. 62 • 2785–2811 • August 2019
Downloaded from: https://pubs.asha.org Richard Peach on 08/16/2019, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions
�Treatment
All participants were exposed to two attention treatment programs: a domain-specific treatment (languagespecific treatment) and a domain-general treatment (DAT).
Both programs followed written guidelines for their administration and were delivered largely by the same advanced
graduate student in speech-language pathology in the same
clinical setting at RUMC.
The study was designed so that each participant received the same dosage and intensity of both treatment
programs. All components of the study (initial assessment, Treatment Program A, post–Treatment Program A
assessment, washout phase, Treatment Program B, post–
Treatment Program B assessment, and final 1 month posttreatment assessment) were completed in approximately
25 weeks. Each treatment program consisted of 15 sessions
(three 1-hr sessions per week for 5 weeks), for a total of
30 treatment sessions. Both treatment programs were discontinued after 15 sessions whether or not they had been
fully completed.
Domain-specific treatment. The domain-specific treatment consisted of L-SAT (Peach, 2012; Peach et al., 2017).
In this program, the tasks and stimuli are language-based
and impose increasing attentional demands on lexical and
sentence processing. The goals of the treatment are to
improve attentional focus and resource management for
language and to automatize attentional recruitment for language. Administration of the program followed a written
protocol that includes directions for task administration,
the materials needed for each task, the task stimuli, the
scoring procedures, the advancement criteria, and the task
discontinuation procedures. The protocol is provided in
Supplemental Material S1 for this article.
The approach is based on a hierarchy of increasingly
more complex language tasks (Peach et al., 2018). For the
simplest task, picture-naming procedures are included to engage attentional mechanisms in the right cerebral hemisphere
by moving the locus of stimulus presentation into left
hemispace. Based on the evidence to date, this modification is appropriate for language-impaired individuals with
left hemisphere brain damage (Coslett, 1999; Crosson et al.,
2007; Dotson et al., 2008). A dual processing task (LaPointe
& Erickson, 1991; see also Hula & McNeil, 2008; McNeil
et al., 2004) is included to promote attention allocation for
lexical processing. The sentence tasks exploit linguistic devices that are known to focus attention during language
clearly was evolved from nonfluent aphasia and exhibited
simplified sentence production and occasional agrammatism.
The participants were, on average, 32 months postonset
of their aphasia (SD = 35.7 months, range: 3–82 months).
The participant characteristics, including their WAB-R
aphasia classifications, are summarized in Table 1.
Procedure
Assessment
A battery of tests and measurement scales were administered to the participants to characterize the nature of their
acquired language and communication deficits, to establish
and measure concomitant attention deficits, and to determine the outcomes of the two treatment programs investigated in this study. Assessment was performed at four time
points: (a) prior to initiation of the first treatment program
(Time 1), (b) after completion of the first treatment program and prior to initiation of a washout phase (Time 2),
(c) after completion of the second treatment program
(Time 3), and (d) 1 month after completion of the second
treatment program (Time 4).
The same battery of measures was given at each administration. Participants were not exposed to their previous assessment scores at any time. General language skills were
assessed using the WAB-R (Kertesz, 2007) and the Object
and Action Naming Battery (Druks & Masterson, 2000).
Higher level language skills were assessed using the Discourse Comprehension Test (Brookshire & Nicholas, 1997).
Functional language was assessed using the Communication Activities of Daily Living–Second Edition (CADL-2;
Holland, Fratalli, & Fromm, 1999). Communicative participation was assessed using the ASHA Quality of Communication Life Scale (QCL; Paul et al., 2004).
To assess attentional abilities, the Test of Everyday
Attention (TEA; Robertson, Ward, Ridgeway, & NimmoSmith, 1994) was administered. Attention allo cation was
assessed using the Stroop test (MacLeod, 1992). The Paced
Auditory Serial Addition Test–3-Second Version (PASAT;
Gronwall, 1977) was administered to assess processing
speed. Finally, the Rating Scale of Attentional Behavior
(RSAB; Ponsford & Kinsella, 1991) was used to assess ecological outcomes regarding attentional abilities following
treatment. The participants’ language and attention standardized test scores at baseline are provided in Table 2.
Table 1. Participant demographic and clinical data.
Participant
P1
P2
P3
P4
Age (years)
Race
Gender
Education (years)
Occupation
MPOa
WAB-R AQ
Aphasia typeb
39
80
62
66
W
B
B
W
M
F
M
M
18
14
16
12
Teacher
Postal worker
Environmental auditor
Carpenter
25
3
82
10
71.7
86.6
86.0
66.0
Anomic
Anomic
Anomic
Conduction
Note. WAB-R AQ = Western Aphasia Battery–Revised Aphasia Quotient; W = White; M = male; B = Black; F = female.
a
Months postonset of aphasia. bWAB-R classification.
Peach et al.: Language-Specific Attention Treatment for Aphasia
Downloaded from: https://pubs.asha.org Richard Peach on 08/16/2019, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions
2789
�Table 2. Pretreatment standardized test scores across participants.
Test
Western Aphasia Battery–Revised Aphasia Quotient (max. = 100)
Information
Fluency
Auditory Verbal Comprehension
Repetition
Naming
Object and Action Naming Battery (max. = 131)
Discourse Comprehension Test (max. = 40)
Communication Activities of Daily Living–Second Edition
Test of Everyday Attention (Attention Factor)
Map Search (Selective)
Elevator Counting With Distraction (Selective)
Visual Elevator (Switching/Mental Flexibility)
Elevator Counting With Reversal (Working Memory)
Telephone Search (Selective)
Telephone Search While Counting (Sustained/Divided)
Lottery (Sustained)
Stroop Color–Word Score
Paced Auditory Serial Addition Test–3-Second Version (max. = 60)
P1
P2
P3
P4
71.1a
9
7
7.15
7
5.4
56a
29a
49b
86.6
9
9
8.7
9.8
6.8
111
35
78
86
9
6
9.5
9
8.5
110
30
94
66.
7.
7.
9.05
3.75
6.2
64.
27.
45.
5
26.6
2.4
37.2
2.4
0.4
2.4
20
0
37.2
16.2
9.5
16.2
74.5
9.5
0.4
18.
0.
16.2c
62.9
37.2
50
83.8
25.6
0.4
28d
20a
5
5
2.4
16.2
5
1.05
0.4
21
0
a
Raw scores. bPercentile ranks. cMidpoint of range for percentile ranks. dT scores.
processing. These include noncanonical sentence structure
(Caplan & Waters, 1999; Myachykov & Posner, 2005;
Shankweiler, Crain, Gorrell, & Tuller, 1989), focus structure
(Cutler & Fodor, 1979), anaphoric reference (Myachykov
& Posner, 2005), grounding elements (Langacker, 2008),
and event windowing (Talmy, 2003). The tasks and phases
that comprise the program, as well as descriptions of the
treatment stimuli, cues, therapeutic operations, and advancement criteria, are provided in Appendix A. Additional
stimuli for the Spatial Attention and Attention Allocation
tasks are available from the first author.
Recent work has established the validity of these tasks
for directing attentional processing in healthy individuals
and in persons with aphasia (Peach et al., 2018). The battery of language tasks that comprises the L-SAT program
follows the expected pattern of engaging attentional processing (selective, sustained/divided, attentional switching),
auditory–verbal working memory, and executive functioning (attentional control). The attentional correlates for each
task for people with aphasia are provided in Table 3.
Each task includes baseline and posttreatment probes
to assess treatment generalization. The baseline stimuli for
the first task, Spatial Attention, include 10 items from each
of the three treatment phases and 10 untreated items. All of
the baseline stimuli for the remaining tasks consist of untreated exemplars of the same forms requiring the same target responses as those required in the treatment tasks with
the exception of the fourth task, Topicalization. Since the
focus structure of these sentences provides the attentiondirecting element, the baseline stimuli for this task assess
comprehension of embedded topics in nontopicalized sentences. The posttreatment probe tasks are identical to the
baseline tasks.
Discontinuation criteria were established for the
baseline probes. A baseline score of 80% accuracy (or
2790
approximately 80% accuracy for probes with odd numbers
of items) on the initial administration of the probe resulted
in discontinuation of the task. In these instances, the next
task was introduced immediately. When the participant did
not meet the discontinuation criterion, three baseline probes
were completed for each task.
Completion criteria were also developed for each task
to expedite the participants’ progression through the program and to achieve the goal of completing the program in
15 sessions. Criterion-level performance for each phase of
all tasks was set at 80% accuracy over two consecutive trials. Once this level of performance was achieved on the last
phase of a task, the posttreatment probe was administered,
and the next task was introduced. If, however, a participant
did not reach criterion on a phase of a task, the task was
discontinued after three sessions. In these instances, the
posttreatment probe for that task was administered, and
the next task was introduced.
Domain-general treatment. The computer exercises
included in APT-3 (Sohlberg & Mateer, 2010; DAT) were
used for the domain-general treatment. The treatment adhered to the instructions for administering these exercises
provided in the program manual. The exercises are organized
to address basic sustained attention and four domains of executive control: working memory, selective attention, suppression, and alternating attention. The program includes
over 400 tasks; many have multiple versions with different
stimuli. Generally, task selection is based on a patient’s accuracy and level of effort for any specific task. Tasks are
designed to be hierarchical and can be modified by manipulating the speed and number of presented stimuli. Guidelines
for task selection, as well as strategy selection and generalization activities, are provided with the program.
Because there are no standardized rules for task
selection, sampling may be required to identify the most
Journal of Speech, Language, and Hearing Research • Vol. 62 • 2785–2811 • August 2019
Downloaded from: https://pubs.asha.org Richard Peach on 08/16/2019, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions
�Table 3. Language-specific attention tasks and attentional correlates for participants with aphasia.
Language task
Spatial Attention
Attention Allocation
Object Manipulation
Topicalization
Anaphora
Nominal Grounding
Clausal Grounding
Windowing
Attention
Memory
Sustained/divided
Sustained/divided
Selective
Attentional switching
Sustained/divided
Attentional switching
Selective
Attentional switching
Sustained/divided
Selective
Sustained/divided
Sustained/divided
Sustained/divided
Central executive
Auditory working
Executive functioning (attentional control)
Auditory working
Executive functioning (attentional control)
Auditory working
Executive functioning (attentional control)
Note. This table is based on results reported by Peach et al. (2018).
appropriate level for a patient (Sohlberg & Mateer, 2010,
p. 29). In order to increase the reliability of the sampling
process for this study, we developed baseline procedures
for identifying the most appropriate entry-level tasks for
each participant. The procedures incorporated the program
guideline suggesting that 80% accuracy with a medium
to high level of effort indicates an appropriate task level
(Sohlberg & Mateer, 2010, p. 29).
The program addresses five components of attention:
(a) auditory and visual sustained attention, (b) auditory and
visual selective attention, (c) auditory working memory,
(d) auditory and visual suppression, and (e) auditory and
visual alternating attention. A hierarchy of the program
tasks (from easiest to hardest) for each attention component
was developed for this study to identify increasing levels of
difficulty. The sampling began at the highest level of difficulty for the task that was at the approximate midpoint in
the task hierarchy for a specific component. An iterating
procedure was used until tasks were identified where the
participants were performing at 60%–90% accuracy, with
an effort rating of 5–10. Those tasks were used as the entry
point for treatment within the appropriate attentional components. Once an entry point was determined, treatment
began immediately within the same session on the selected
tasks. If an entry-level task was not identified in the first
session, baseline probing continued in a subsequent session
until an appropriate, entry-level task was identified. The
complete baseline procedures are described in Appendix B.
Once entry-level tasks were identified for the five
attentional components, treatment generally addressed all
components in each session. The criterion for advancement
to the next most difficult task for each component was
80% accuracy over two consecutive trials using different
versions of the task where appropriate. Effort ratings were
not considered for advancement. If a participant performed
with 90% or greater accuracy on an ensuing task, that task
was discontinued, and treatment advanced to the next
most difficult task. This procedure was applied continuously
to identify tasks at increasing levels of difficulty within
the target range of performance. Treatment for a specific
component was discontinued if all tasks for that component
were completed. The treatment program was discontinued
at the end of the 15th session.
Design
A randomized controlled cross-over single-subject
design (Hart & Bagiella, 2012; Maxwell & Satake, 1997;
Piantadosi, 2005), also known as an alternating treatments
design (Barlow & Hayes, 1979; Barlow, Nock, & Hersen,
2009), was used to assess the effectiveness of the two treatments administered in this study. Each patient underwent
both treatments. The participants were randomly assigned
to each treatment order based on the sequence of their entry into the study. Two participants received the treatments
in the order AB (language-specific treatment followed by
DAT), while the other two participants received the treatments in the reverse BA order. The participants who were
randomized to the AB order were designated Participants 1
and 2 for ease of tracking. The participants who were randomized to the BA order were designated Participants 3
and 4. At the end of the first treatment phase, all participants
underwent a 1-month period of no treatment (washout
period) to minimize any carryover effects.
Analyses
The following procedures were undertaken to analyze
the data. For the language-specific treatment, effect sizes
were calculated for the differences between the baseline phases
and the intervention phases for each phase of each task as
well as for the differences between the baseline and posttreatment phases of the study. Visual analyses were performed
to assist in the interpretation of the statistical analyses. For
the DAT, effect sizes could not be calculated as the administration procedures for the APT-3 computer exercises do
not include collection of pretreatment or posttreatment probe
data. Therefore, the participants’ performances were analyzed
descriptively and visually. Trend analyses were performed to
complement the visual assessment of the data.
Peach et al.: Language-Specific Attention Treatment for Aphasia
Downloaded from: https://pubs.asha.org Richard Peach on 08/16/2019, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions
2791
�Pretreatment and posttreatment standardized test scores
were analyzed and compared to assess the outcomes of
the two treatment programs. Finally, the results obtained
from patient-reported outcome scales were examined to
determine the extent of any changes in ecological communication and attention outcomes.
Reliability
The L-SAT tasks have been shown to demonstrate
good to excellent reliability in participants with aphasia
(Peach et al., 2018). Test–retest reliability ranges from r = .84
to .98 with one exception, Attention Allocation, when using
the scoring procedure for this task adopted in this study
(see Peach et al., 2018, for discussion of this finding). The
interclass correlation coefficients for inter- and intrarater
reliability are .97 and 1.0, respectively.
None of the administration procedures for the APT-3
exercises have been evaluated “empirically” (Sohlberg &
Mateer, 2010, p. 31). The program is computer based, and
guidelines for delivering the program are provided in the program manual. The score sheets that accompany each task
allow for tracking of important performance indicators, for
example, accuracy/time, error patterns, and level of effort.
A case example is provided in the manual to increase adherence to the program procedures.
Results
Interventions
L-SAT
While all participants received 15 sessions of treatment,
the baseline and completion criteria resulted in the participants progressing through the program at different rates.
This resulted in their completing varying numbers of task
trials and different numbers of phases and/or tasks. The participants completed between 49 and 76 (M = 62, SD = 11.9)
task trials (including baseline and posttreatment probes)
during the treatment period.
The participants’ performances across all tasks are provided in Figures 1–4. Participants 2 and 3 met the discontinuation criteria for Spatial Attention on initial exposure
at baseline. Therefore, only Participants 1 and 4 completed
this task. Participants 1 and 3 met the discontinuation criteria for Attention Allocation on initial exposure, whereas
Participants 2 and 4 met the completion criteria for this
task during baseline testing. None of the participants, therefore, were treated with the Attention Allocation task (see
Figures 1–4).
Participant 2 also met the completion criteria for
Object Manipulation during baseline testing. Participant 4
did not advance to Clausal Grounding, and no participant advanced sufficiently to be exposed to the last task,
Windowing, although Participant 3 did complete baseline
testing for this task. Otherwise, all participants were exposed to at least four sentence-processing tasks. Over all,
Participant 1 was exposed to six tasks (one word and five
sentence level), Participant 2 was exposed to four tasks (all
2792
sentence level), Participant 3 was exposed to five tasks (all
sentence level), and Participant 4 was exposed to five tasks
(one word and four sentence level). Some participants did
not complete all phases for all of the tasks to which they
were exposed.
Visual analyses of the plots for the participants’ performance across tasks demonstrated post–baseline improvements during the intervention phases for these tasks. By
and large, the data were characterized by linear trends suggesting steady increases in task performances until the later,
more complex sentence-processing tasks. Performances on
these tasks were more variable.
To determine the effect sizes associated with languagespecific treatment, Tau-U was calculated (Brossart, Laird,
& Armstrong, 2018; Lee & Cherney, 2018; Parker, Vannest,
Davis, & Sauber, 2011) for each phase of all tasks undergoing treatment using the online calculator available for this
procedure (Vannest, Parker, Gonen, & Adiguzel, 2011).
Tau-U measures both baseline and intervention-phase
trends. Baselines phases with trends can be corrected. The
procedure also provides significance testing and confidence
intervals to assist in interpreting the outcomes.
Data sets with tau ≥ .40 during both the baseline and
intervention phases trending in the same direction (Parker
et al., 2011) underwent baseline correction. Using these criteria, the baselines for Participants 2 and 4 on Topicalization and for all participants on Clausal Grounding were
corrected; none of the remaining tasks required baseline
correction.
Omnibus effect sizes (weighted tau) combined across
all participants were calculated for the intervention phases
of each task to assess the significance of the resulting changes
in performance (see Table 4). The effect sizes were statistically significant ( p < .05) for all phases of all tasks, with
the exception of four: Phase C of Anaphora ( p = .56),
Phases A ( p = .44) and B ( p = 1.0) of Nominal Grounding
(no participant advanced to Phase C of this task), and
Phase A ( p = .18) of Clausal Grounding. These findings indicate that the participants made significant improvements within the time frames of this study in 69% of the
13 program phases in which they participated until reaching the highest and most advanced levels of the treatment
program.
Standardized effect sizes (Beeson & Robey, 2006; Busk
& Serlin, 1992; see also Lee & Cherney, 2018) were calculated where possible for the tasks exposed to treatment to
determine the differences between the baseline and posttreatment phases of L-SAT intervention (see Table 5). Effect
sizes were not calculated for tasks with no/minimal variability
in the pretreatment baseline scores. To aid in the interpretation of these results and in the absence of previous benchmarks for this treatment program, the observed effect sizes
were assembled into four nonoverlapping groupings (based
on the distribution of the observed scores) and categorized
as follows: large effects (7.44 or greater), medium effects
(2.77–3.18), small effects (0.66–1.44), and no effect (< 0.66).
Of the 18 individual effect sizes that were calculated,
three (56%) indicated large, positive treatment effects;
Journal of Speech, Language, and Hearing Research • Vol. 62 • 2785–2811 • August 2019
Downloaded from: https://pubs.asha.org Richard Peach on 08/16/2019, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions
�Figure 1. Performance scores for Participant 1 for language-specific attention treatment across phases and tasks. Baseline probe data are
plotted using triangles, intervention phase data are plotted using circles, and posttreatment probes are plotted using squares. Attn. = Attention;
Obj. = Object; Nom. = Nominal.
five (28%) indicated medium, positive effects; three (17%)
indicated small, positive effects; and six (33%) indicated
no treatment effect. In summary, positive treatment effects
were observed for 67% of the L-SAT tasks. Participants 1
and 3 showed medium to large treatment gains on 4/6
and 2/3 tasks, respectively, and Participants 2 and 4 showed
small to medium gains on 3/5 and 2/4 tasks, respectively. Thus, all four of the individual participants demonstrated some degree of treatment gain in response to
L-SAT exposure.
Weighted standardized effect scores (Beeson & Robey,
2006) were also calculated to assess group performance
patterns for each task (see Table 5). Fitting the weighted
scores to the effect size groupings described above, positive
treatment effects were observed in response to five of the
six L-SAT tasks. Anaphora generated a large effect, Spatial
Attention and Object Manipulation produced medium effects, and Topicalization and Clausal Grounding yielded
small effects. Only one task, Nominal Grounding, produced
no effect.
DAT
As in L-SAT, the number of APT-3 computer tasks
that were performed and the number of sessions to complete each task varied across participants (see Table 6).
The mean number of tasks performed by each participant
per cognitive domain was 2.3 (SD = 1.58, range: 1.3–3.8),
and the mean number of sessions per task to completion
was 3.49 (SD = 1.07, range: 2.63–5.25). The mean level
of accuracy across tasks at entry into the program was
61% (SD = 0.19, range: 28%–79%), and the mean change
across tasks following treatment was 5% (SD = 0.21, range:
−4% to 11%). Participants 1 and 4 demonstrated mean increases in performance across all tasks. Participant 2 declined from baseline levels of performance on 89% of the
tasks posttreatment, and Participant 3 declined on 67% of
the tasks.
The participants’ performances for each APT-3 computer task within the five cognitive domains are demonstrated
in Figures 5–9. In lieu of effect sizes (because of the absence
of baseline phases), trend lines were fit using Microsoft Excel to assist in the visual analyses of the data. Single data
points were not included in these analyses. Trend lines were
fit to achieve an R2 as close to 1 as possible. All data were
found to conform to either a linear or polynomial trend. R2
for linear trends ranged between .9346 and 1. R2 for polynomial trends are shown in each graph.
The data for all tasks, with the exception of those
addressing Working Memory, were characterized by both
linear and polynomial trends. The data for Working Memory were characterized exclusively by polynomial trends. In
all domains, excluding visual selective attention, the data
conformed to polynomial trends a majority of the time (see
Table 6). In the case of visual selective attention, the data
demonstrated a polynomial trend just under half (42%)
of the time. These findings indicate that the participants’
Peach et al.: Language-Specific Attention Treatment for Aphasia
Downloaded from: https://pubs.asha.org Richard Peach on 08/16/2019, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions
2793
�Figure 2. Performance scores for Participant 2 for language-specific attention treatment across phases and tasks. Baseline probe data are
plotted using triangles, intervention phase data are plotted using circles, and posttreatment probes are plotted using squares. Attn. = Attention;
Obj. = Object; Nom. = Nominal.
performance on the APT-3 computer tasks largely fluctuated from trial to trial and suggest a wide degree of variability in performance across trials on these tasks.
Standardized Testing
The difference scores comparing pretreatment and
posttreatment scores for both intervention programs are
provided in Table 7. Difference scores were calculated by
subtracting the Time 1 test scores from the Time 2 test
scores following the first intervention and by subtracting
the Time 2 test scores from the Time 3 test scores following the second intervention.
Language
To assess the outcomes for each intervention program
on standardized language testing, summary scores were
calculated using the raw difference scores for the WAB-R,
the Object and Action Naming Battery, and the Discourse
Comprehension Test. The summary scores therefore indexed
a wide array of language abilities, including basic skills,
lexical retrieval for both nouns and verbs, and higher order
auditory comprehension skills. Comparing these scores
across participants revealed that Participant 1 made substantial improvements following both L-SAT and DAT, Participant 2 made greater gains following L-SAT than DAT,
Participant 4 made greater gains following DAT than L-SAT,
and Participant 3 made essentially no gains following either
2794
program. Changes in functional language, however, were
notable following L-SAT, where the participants improved
an average of 17.8 percentile points on the CADL-2, compared to an average decline of 1.25 percentile points on this
test following DAT.
Next, we investigated whether the WAB-R scores
captured posttreatment changes in language abilities. Previously, increases in the WAB-R AQ greater than the estimated standard error of measurement for the WAB-R (i.e.,
5 points) have been used to suggest clinically significant
improvement (Elman & Bernstein-Ellis, 1999; Katz &
Wertz, 1997). A problem with this approach concerns the
assumption of equal measurement error across individuals,
regardless of the severity of their aphasia (Hula, Donovan,
Kendall, & Gonzales-Rothi, 2010). Instead, we analyzed
the pretreatment–posttreatment changes on the WAB-R
for each participant using the method reported by Hula
et al. (2010). In this approach, WAB-R scores are fit to a
Rasch model to create a more normal distribution of item
scores and standard error scores that match the ability of
each participant. According to Hula et al., the approach
is a more valid method for indexing aphasia severity and
change. Thus, the Rasch-based WAB-R scores for each
participant were compared to determine whether the posttreatment results for each treatment approach were reliably
different from one another.
The WAB-R scores for Times 1 and 2 were compared
using the Microsoft Excel WAB Rasch score sheet developed
Journal of Speech, Language, and Hearing Research • Vol. 62 • 2785–2811 • August 2019
Downloaded from: https://pubs.asha.org Richard Peach on 08/16/2019, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions
�Figure 3. Performance scores for Participant 3 for language-specific attention treatment across phases and tasks. Baseline probe data are
plotted using triangles, intervention phase data are plotted using circles, and posttreatment probes are plotted using squares. Attn. = Attention;
Obj. = Object; Nom. = Nominal.
for this analysis (W. Hula, personal communication, May
25, 2018) to assess changes after the first intervention and
for Times 2 and 3 to assess changes after the second intervention. The procedure uses one-tailed probabilities that
assume improvements in WAB-R scores following treatment.
Therefore, only those change scores that demonstrated
increases in performance were considered for this analysis.
To assess the significance of the individual changes
in WAB-R scores in this small sample, α was set at .15
(Crawford, Sommerville, & Robertson, 1997; Wechsler,
1981). Significantly improved WAB-R scores were found
for Participant 1 ( p = .09), Participant 2 ( p = .08), and
Participant 4 (p = .09) following L-SAT. Only Participant 1
showed significant improvement on the WAB-R following
DAT ( p = .01). Using the percentile ranks obtained from
the Hula et al. (2010) sample, Participant 1 improved
from the 26th to the 32nd percentile, Participant 2 improved
from the 57th to the 71st percentile, and Participant 4 improved from the 29th to the 34th percentile following L-SAT.
Following DAT, Participant 1 improved from the 32nd to
the 46th percentile.
Finally, maintenance of posttreatment scores 1 month
after the conclusion of treatment was assessed by comparing the WAB-R scores obtained at Times 3 and 4. No significant changes were observed for Participants 1 and 2
following the completion of DAT or Participant 4 following
L-SAT. However, significant improvement was observed for
Participant 3 following L-SAT (p = .07). Interestingly, it
should be noted that Participant 3 was the only individual
who did not show significant posttreatment improvements to
either treatment at the termination of each program.
Attention
Difference scores were calculated between the pretreatment and posttreatment administrations of the TEA, the
Stroop test, and the PASAT following L-SAT and DAT
(see Table 7). The mean percentile differences for the seven
subtests of the TEA were determined for each participant
using the midpoint of the percentile ranges for each scaled
score provided by Robertson et al. (1994). Overall, the only
improvement on the TEA was observed for Participant 1
following L-SAT. Otherwise, the average change for the
other three participants was 1 percentile point or less.
When inspecting the changes for individual subtests by
participant, the largest changes (greater than 5 percentile
points) occurred following L-SAT for Map Search (Participant 1), Elevator Counting With Distraction (Participants
1, 3, and 4), Visual Elevator (Participant 1), and Elevator
Counting With Reversal (Participant 1). Large changes on
Telephone Search (Participants 2 and 4) and Telephone
Search While Counting (Participants 1 and 3) were observed following both L-SAT and DAT.
To investigate these individual differences further,
we analyzed each participant’s TEA scaled scores using
Peach et al.: Language-Specific Attention Treatment for Aphasia
Downloaded from: https://pubs.asha.org Richard Peach on 08/16/2019, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions
2795
�Figure 4. Performance scores for Participant 4 for language-specific attention treatment across phases and tasks. Baseline probe data are
plotted using triangles, intervention phase data are plotted using circles, and posttreatment probes are plotted using squares. Attn. = Attention;
Obj. = Object; Nom. = Nominal.
the method recommended by Crawford et al. (1997). In
this approach, participants’ performances are assessed
with regard to the pattern of individual strengths and
weaknesses across the seven subtests of the battery to identify reliable differences among subtests. To achieve this, discrepancy scores estimating specific levels of significance are
calculated using particular subtest scores and the mean subtest score for the battery. A computer program is available
to perform these calculations (Crawford, 2018).
We applied this procedure to assess the significance of
changes across TEA administrations following both treatment programs. Our interest was in identifying those subtests
Table 4. Omnibus effect sizes calculated across participants for language-specific attention treatment tasks by intervention phases.
Task
Spatial Attention
Attention Allocation
Object Manipulation
Topicalization
Anaphora
Nominal Grounding
Clausal Grounding
Windowing
Phasea
Participantsb
Tauc
z
p
Confidence intervald
A
B
C
A
B
A
B
—
A
B
C
A
B
C
A
B
A–C
2
1
1
0
0
3
3
4
4
4
3
4
3
0
4
2
0
0.84
1.0
1.0
—
—
1.0
−0.88
0.59
1.0
0.56
0.21
0.18
0
—
0.39
0.76
—
2.83
2.24
1.96
—
—
3.49
−2.88
2.57
3.62
2.34
0.58
0.77
0
—
1.69
2.15
—
0.005
0.025
0.049
—
—
0.001
0.004
0.010
0.000
0.019
0.561
0.439
1.0
—
0.089
0.032
—
[0.2564, 1]
[0.264, 1]
[0.162, 1]
—
—
[0.4377, 1]
[−1, −0.2813]
[0.1406, 1]
[0.4583, 1]
[0.0913, 1]
[−0.4926, 0.9075]
[−0.2761, 0.6363]
[−0.6160, 0.6160]
—
[−0.0600, 0.8346]
[0.0658, 1]
—
Note. Em dashes indicate there are no data for these phases.
a
Phase of intervention for tasks with multiple phases (see Appendix A). bNumber of participants completing designated phase. cOmnibus
effect size for participants completing phase (in cases with one participant, tau equals effect size for contrast between participant’s baseline
and intervention phases). dConfidence intervals reported at 95% level except for Spatial Attention B and C, which is reported at 90% level.
2796
Journal of Speech, Language, and Hearing Research • Vol. 62 • 2785–2811 • August 2019
Downloaded from: https://pubs.asha.org Richard Peach on 08/16/2019, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions
�Table 5. Standardized effect sizes (d ) for pretreatment–posttreatment
differences in language-specific attention treatment performance by
tasks and participants as well as across participants.
Task
P1
P2
P3
P4
Spatial Attention
2.77
NA
NA
3.00
Attention Allocation
NA
NA
NA
NA
Object Manipulation
7.44 −1.20
*
0.80
Topicalization
2.89
3.18
*
−2.02
Anaphora
15.17 −0.50 12.86
*
Nominal Grounding
0.10
0.66 −2.92 −0.59
Clausal Grounding
−0.43
1.44
2.28
**
Counting With Reversal ( p < .05), and Participant 3 improved significantly on Elevator Counting With Distraction
(p < .01). Following DAT, the probability of reliable change
for Participant 1 increased for both Visual Elevator (p < .05)
and Elevator Counting With Reversal (p < .01). No other
significant changes in TEA subtest performance were
observed.
The pattern of performance for Participants 1 and 4
on the Stroop test was characterized by improvement after
administration of either treatment initially followed by
additional but smaller improvement after exposure to the
second treatment. For Participant 1, the change score following L-SAT resulted in his improving from the impaired
range to the borderline range (Psychometric Conversion
Table, n.d.). Additional increases following DAT improved his performance into the low average range of
performance. For Participant 4, exposure to DAT improved
his performance from the profound range to the impaired
range, and subsequent exposure to L-SAT improved his
performance to the borderline range. Participant 2 did
not improve on this test in response to L-SAT but showed
slight improvement to the severe range following DAT.
Participant 3 did not improve on this test in response to
either treatment.
Finally, Participant 1 demonstrated a large change
on the PASAT in response to L-SAT, whereas Participants 3 and 4 demonstrated large changes on this test in
response to DAT. The change observed in Participant 1
following L-SAT was sufficient to boost his score into the
low normal range for this test (Rao, Leo, Bernardin, &
Unverzagt, 1991). As was the case with the Stroop test,
Participants 1 and 4 showed smaller, additional improvements when exposed to DAT and L-SAT, respectively.
Participant 3 showed no further improvement following
L-SAT. Participant 2 demonstrated no changes in response
to either treatment.
Weighted d
2.89
—
4.12
1.35
9.18
−0.72
1.10
Note. Em dash indicates there is no effect size. NA = participant
met task criteria at baseline; * = unable to calculate effect size due
to no or minimal variability in baseline; ** = program completed,
no final posttreatment probe.
that improved significantly, relative to the participants’
individual abilities, following treatment. To do this, we
first identified subtests on which a participant performed
significantly better than average at baseline and within
the range of normal performance. Participants 1 and 4 performed significantly above average on Telephone Search
( p < .01), and Participant 3 performed significantly above
average on Elevator Counting With Reversal ( p < .10).
As these subtests represented individual strengths, they
were eliminated from further consideration when assessing changes following treatment. There were no significant discrepancies between any of the subtests performed
by Participant 2.
Next, we examined whether participants, given their
own levels of ability, improved significantly on any of the
remaining subtests for the two posttreatment administrations
that followed. Following L-SAT, Participant 1 improved
significantly on Visual Elevator ( p < .15) and Elevator
Table 6. Grouped performance data for direct attention training.
Cognitive domain
Input
modality
No. of tasks
performed
Sessions/
task
Initial percent
accuracy
Mean percent
change
Sustained Attention
Auditory
3.3 (0.96)
2.75 (1.50)
Visual
1.8 (1.50)
5.25 (0.50)
Auditory
3.8 (2.22)
3.99 (0.37)
Visual
3.3 (3.86)
2.88 (1.65)
Working Memory
Auditory
1.8 (1.50)
4.38 (1.49)
Suppression
Auditory
1.5 (1.00)
3.63 (1.49)
Visual
2.8 (2.22)
2.79 (0.98)
Auditory
1.3 (0.50)
3.13 (1.18)
Visual
1.3 (0.50)
2.63 (0.48)
67 (0.19)
(39–79)
65 (0.22)
(37–83)
68 (0.12)
(55–81)
79 (0.18)
(61–96)
28 (0.21)
(0–50)
47 (0.30)
(13–82)
72 (0.14)
(62–92)
50 (0.27)
(11–72)
76 (0.10)
(63–86)
11 (0.31)
(−17 to 52)
8 (0.18)
(−18 to 26)
1 (0.15)
(−20 to 16)
−4 (0.22)
(−36 to 16)
11 (0.21)
(−12 to 30)
6 (0.10)
(−7 to 14)
10 (0.22)
(−5 to 43)
6 (0.25)
(−16 to 33)
0 (0.20)
(−24 to 23)
Selective Attention
Alternating Attention
Trend (%)
Linear
Polynomial
10
90.
20
80.
25
75.
57.1
42.9
0
100.
20
80.
37.5
62.5
20
80.
40
60.
Peach et al.: Language-Specific Attention Treatment for Aphasia
Downloaded from: https://pubs.asha.org Richard Peach on 08/16/2019, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions
2797
�Figure 5. Performance scores across participants for Attention Process Training–3 alternating attention tasks. Auditory tasks are plotted
using circles, and visual tasks are plotted using triangles.
Patient-Reported Outcomes
In order to assess the ecological outcomes following
these treatments, participants completed the QCL (Paul
et al., 2004) and the RSAB (Ponsford & Kinsella, 1991;
see Table 8). The QCL consists of 17 statements scored 1–5
(5 = highest), assessing the impact of the participant’s aphasia on his or her communication and participation in life
situations. Higher scores indicate less communicative
disruption. The RSAB describes 12 everyday behaviors
that are associated with attentional impairments and
the frequency with which they affect the participant.
Items are scored on a 5-point scale (0 = not a problem,
5 = is a problem all the time). Lower scores indicate less
impairment.
The mean QCL difference scores were compared by
participant following administration of the two treatment
programs (see Table 8). Participant 3 responded at ceiling
for all items (despite his significant aphasia) on the posttreatment administrations for both programs. Because of
the lack of variability and questionable reliability of his
responses, he was removed from this analysis. The group
QCL difference score following L-SAT (M = 0.58, SD = 0.05)
exceeded that following DAT (M = 0.24, SD = 0.78), although this difference was not statistically significant (z =
−0.54, p = .59, Wilcoxon signed-ranks test). Individually,
two of the three participants rated their communication
higher following L-SAT than DAT.
2798
The total RSAB scores following each treatment were
also compared. Again, Participant 3 rated himself as having
virtually no attentional problems on the first two administrations of the RSAB but followed these ratings with one
indicating substantial attentional problems on the last administration. As with the QCL above, this pattern suggested
unreliable responses, and he was excluded from this analysis.
The mean decline in attentional problems following L-SAT
was 9.3 points (SD = 17.0). The mean decline following
DAT was 2.7 points (SD = 14.7). The probability of this difference representing a reliable change was 89% (z = −1.60,
p = .11, Wilcoxon signed-ranks test). All three participants
rated their attentional abilities more favorably following
L-SAT than DAT.
Discussion
In this study, we compared the effectiveness of L-SAT,
a domain-specific approach, to DAT, a domain-general
approach, for treating the language and attentional deficits
associated with aphasia. Based on recent reports and recommendations in the extant literature, we hypothesized
that the domain-specific approach to improving attention
for language would result in more desirable outcomes
than a domain-general approach to treating attention
for language in people with aphasia. Although both treatment programs produced variable improvements in both
Journal of Speech, Language, and Hearing Research • Vol. 62 • 2785–2811 • August 2019
Downloaded from: https://pubs.asha.org Richard Peach on 08/16/2019, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions
�Figure 6. Performance scores for Participants 1, 2, 3, and 4 for Attention Process Training–3 selective attention tasks. Auditory tasks are
plotted using circles, and visual tasks are plotted using triangles.
language and attention across participants, the preponderance of the findings in this study provides support for our
hypothesis.
We investigated the outcomes for each approach with
regard to these participants’ language impairment, their
functional language, and their personal reports regarding
their language and attentional abilities before and after
treatment. Visual comparisons of the participants’ performances on the treatment tasks in each program demonstrated steadier, linear improvements following L-SAT
versus more variable and unpredictable patterns of performance following DAT. This latter finding is consistent
with the increased between-sessions and within-session
variability that has been observed in people with aphasia in
response to domain-general attention training (Villard &
Kiran, 2018).
Tau-U effect sizes were statistically significant for nine
of the 13 L-SAT task phases that were administered suggesting reliable improvements. The three task phases for which
improvement was not demonstrated were among the most
complex tasks in the program. Also, the weighted effect
sizes for posttreatment changes following L-SAT ranged
conservatively from small to large with the exception of one
task (Nominal Grounding). Using the widespread metric
Peach et al.: Language-Specific Attention Treatment for Aphasia
Downloaded from: https://pubs.asha.org Richard Peach on 08/16/2019, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions
2799
�Figure 7. Performance scores across participants for Attention Process Training–3 attention suppression tasks. Auditory tasks are plotted
using circles, and visual tasks are plotted using triangles.
suggested by Cohen (1988), all of these effect sizes would be
considered large. Alternatively, the group average gain following DAT was 5%. Individually, while two of the participants showed mean increases overall, one declined from
baseline levels on two thirds of the tasks, and another declined from baseline on almost 90% of the tasks.
The results of standardized testing also favor the domain-specific approach. Simple sums of change scores for
the three standardized language tests suggested that one or
the other program (or both) may result in language improvements. However, the analysis of the WAB-R AQs, taking
person ability into consideration, demonstrated reliable
improvements for three of the four participants following
L-SAT, while only one participant improved reliably on
the WAB-R following DAT. Also, the margins of improvements in functional language were substantially larger
following L-SAT than DAT. These results provide further
evidence that either program may produce some language
improvements in people with aphasia but that a more robust outcome may be achieved from the domain-specific
approach both in terms of reducing language impairment
and improving functional language.
Some may assert that a language-based approach to
treatment (i.e., L-SAT) would be expected to produce better
outcomes in people with aphasia than a non–language-based
approach (i.e., DAT) and that the improvements described
2800
above are simply an outcome of this difference. However,
the test of this concern would be whether a domain-general
attentional approach results in improvements to attentional
processing that is not observed following a domain-specific
language-based approach. While both L-SAT and DAT are
known to engage attentional processing, the posttreatment
results suggested that L-SAT resulted in attentional improvements, even in purported nonlanguage tasks, that
exceeded those of the purely domain-general approach. These
results provide further support for the attentional requirements of the L-SAT tasks (Peach et al., 2018).
Following treatment, only one participant showed an
overall net improvement in performance on the TEA, and
this was in response to L-SAT. In addition, the individual
patterns demonstrated that large improvements for four of
the six TEA subtests occurred following L-SAT, while improvements on the remaining two tasks occurred following
both L-SAT and DAT. When assessing TEA performance
relative to the participants’ own strengths and weaknesses,
one participant improved significantly on two TEA subtests
following L-SAT and one on one TEA subtest. The only
significant individual improvement following DAT occurred
for one participant on two TEA subtests that were exposed
previously to L-SAT.
Equivocal results were demonstrated following
these treatments with regard to the Stroop test (attention
Journal of Speech, Language, and Hearing Research • Vol. 62 • 2785–2811 • August 2019
Downloaded from: https://pubs.asha.org Richard Peach on 08/16/2019, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions
�Figure 8. Performance scores across participants for Attention Process Training–3 sustained attention tasks. Auditory tasks are plotted using
circles, and visual tasks are plotted using triangles.
allocation) and the PASAT (speed of processing). For the
Stroop test, two participants showed initial improvement following the first treatment (L-SAT in the first instance, DAT
in the second) and continued improvement following the alternate treatment. Another showed slight improvement on
this test following DAT, and the fourth participant showed
no improvement to either treatment. For the PASAT, two
participants improved substantially following DAT and
one following L-SAT. Continued smaller improvements
were noted following exposure to the alternate treatment
in two cases. One of the participants who improved following DAT showed no further improvement to L-SAT, and
one participant showed no improvements to either treatment.
Greater improvements in speed of processing might be expected following DAT as some of the tasks in this program
include speeded presentations while none of the L-SAT
tasks address this component of attention.
Finally, the patterns for communication and attentional
improvements in functional language and patient perceptions following treatment favored L-SAT when compared
to DAT. Thus, L-SAT appears to provide a more ecologically valid approach to treating language and attention
given its emphasis on specific skills. Apparently, this emphasis is perceived as translating to everyday language and
attentional behaviors more effectively than domain-general
tasks. In this way, L-SAT provides (a) a working framework
for individual training that is tailored to the participant’s
particular needs and expectations and (b) a more ecological
perspective to theoretical models of cognition and their
application (Moreau & Conway, 2014).
Given the promising results obtained with L-SAT,
despite none of the participants finishing the program as
constructed, a question arises whether even more robust
outcomes could be achieved when PWA are exposed to the
complete program. The treatment schedule used with these
participants was constrained by the parameters of this
study. Nonetheless, the schedule emulated a somewhat typical, nonintensive course of contemporary aphasia treatment (Cherney, Patterson, & Raymer, 2011). As a result,
no participant was exposed to the most complex tasks in
the L-SAT program. It is intriguing then, given the beneficial effects associated with higher complexity and language
processing (Kiran & Thompson, 2003; Rubin, Newhoff,
Peach, & Shapiro, 1996; Thompson, Ballard, & Shapiro,
1998; Thompson & Shapiro, 2007; Thompson, Shapiro,
Kiran, & Sobecks, 2003), to speculate whether an extended
treatment schedule allowing for exposure to these tasks
might have resulted in further improvements. This will
be an important issue for future investigations regarding
L-SAT effectiveness.
Peach et al.: Language-Specific Attention Treatment for Aphasia
Downloaded from: https://pubs.asha.org Richard Peach on 08/16/2019, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions
2801
�Figure 9. Performance scores across participants for Attention Process Training–3 working memory tasks.
& Zimba, 2000; McNeil, Hula, & Sung, 2011; McNeil, Odell,
& Tseng, 1991; Tseng, McNeil, & Milenkovic, 1993). Descriptions that attempt to separate attention from language
processing (e.g., language and cognition; American SpeechLanguage-Hearing Association, 2016; Villard & Kiran, 2017)
or that refer to the attentional contributions to language
These results demonstrate how attention and language
bind together in the service of word and sentence processing
to form a cohesive mechanism for language processing.
Thus, resource perspectives regarding aphasia are well positioned to explain how attentional impairments in aphasia
account for language deficits (Granier, Robin, Shapiro, Peach,
Table 7. Standardized test difference scores posttreatment for language-specific attention treatment (L-SAT) and direct attention training
(DAT).
P1
Test
L-SAT
Western Aphasia Battery–Revised Aphasia Quotient
Object and Action Naming Battery
Discourse Comprehension Test
Summary score
Communication Activities of Daily Living–Second Edition
Test of Everyday Attention (Attention Factor)
Map Search (Selective)
Elevator Counting With Distraction (Selective)
Visual Elevator (Switching/Mental Flexibility)
Elevator Counting With Reversal (Working Memory)
Telephone Search (Selective)
Telephone Search While Counting (Sustained/Divided)
Lottery (Sustained)
Mean difference
Stroop Color–Word Score
Paced Auditory Serial Addition Test–3-Second Version
P2
P3
P4
DAT
L-SAT
DAT
DAT
L-SAT
DAT
L-SAT
5.6
25a
−5a
25.6
30b
5.7
7
14
26.7
11
4.2
−1
2
5.2
8
0.4
−4
−1
−4.6
−8
1.3
0
−1
0.3
−4
−5.4
6
−1
−0.4
−12
−3.6
22
4
22.4
−4
10.3
2.
2.
14.3
45.
9.4b
20.9
53.4
45.0
−9.3
49
0.0
24.0
6c
17a
0
−20.9
0
2.6
−37.4
−49.0
0.65
−14.85
5
8
0
0
0
0
5
0
0
0.7
1
0
4.5
0
0
0
−7.05
8.4
0.7
0.92
3
0
0
−9.4
2.6
−11.6
0
25.2
−2.0
0.7
−1
20
0
33.8
−4.0
−20.6
−1.4
−25.2
0
−2.5
−4
−11
−11.6
−6.8
0
0
16.1
0
0
−0.3
9
10
0.
6.8
0.
0.
0.
0.
0.
1.0
2.
3.
a
a
Raw score difference. bPercentile rank difference. cT-score difference.
2802
Journal of Speech, Language, and Hearing Research • Vol. 62 • 2785–2811 • August 2019
Downloaded from: https://pubs.asha.org Richard Peach on 08/16/2019, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions
�Table 8. Participant responses on patient-reported outcome measures by treatment program and assessment time (T).
P1
Measure
T1
ASHA Quality of Communication
3.6
Life Scale (maximum = 5.0)
Rating Scale of Attentional Behavior 22
(0 = highest, 48 = lowest)
P2
T2 L-SAT T3 DAT
4.1
14
3.9
24
T1
P4
T2 L-SAT T3 DAT T1 T2 DAT T3 L-SAT
3.7
40
P3
4.3
13
4.7
21
5.0
5.0
0
1
5.0
37
T1
3.4
17
T2 DAT T3 L-SAT
2.8
26
3.4
24
Note. L-SAT = language-specific attention treatment; DAT = direct attention training.
processing as somehow being “extralinguistic” (e.g., Murray
& Mayer, 2017) miss these integral relationships. The results
of this and previous work provide evidence for how attention
is recruited to process language and for how attentional
processing can be manipulated and strengthened through
the performance of language tasks that require increasingly
complex attentional abilities. The results also support the
view that attention is allocated in ways that are particular
to specific tasks rather than as a general resource that is allocated equivalently to all processing tasks (Park & Ingles,
2001; Sturm et al., 1997, 2003).
Limitations
While the randomized controlled cross-over design
offers a valid design for comparing the effectiveness of
two different treatments (see, e.g., Cherney, Kaye, & van
Vuuren, 2014; Crosson et al., 2007; Wilson, Emslie, Quirk,
& Evans, 2001), an important limitation concerns possible
confounds from carryover effects between treatments (also
known as multiple treatment interference). That is, treatment effects observed from a first treatment may continue
to influence the outcomes of a second treatment (Barlow
& Hayes, 1979; Hart & Bagiella, 2012; Piantadosi, 2005).
However, some recommended methods to address these
problems (Barlow & Hayes, 1979) were used in this study.
For example, the treatment periods in this study were
widely spaced because of the washout period so carryover
effects, if any, would be expected to be transient. Also, the
counterbalanced order of treatments are thought to minimize carryover effects across the treatment conditions.
Finally, only one treatment was administered per session in
each treatment phase. Carryover effects have been thought
to be most pronounced when the treatments are alternated
rapidly and within a short time. Nonetheless, despite the
fact that the study followed the typical structure of a randomized controlled cross-over design, testing prior to the beginning of the second treatment phase might have provided
information to assess the extent of carryover effects, if any.
The convenience sample for this study included four
PWA with varied profiles. Three of the participants presented
with fluent aphasia from the onset of their condition, while
one evolved to a profile of fluent aphasia from nonfluent
aphasia. Three presented with chronic aphasia, while one
(Participant 2) was in the subacute stage of her recovery. While
the time postonset for this latter participant might raise
concerns regarding spontaneous recovery, the pattern of
substantially greater improvement following her first treatment when compared with the second should diminish this
concern. Two presented with mild aphasia, while two presented with moderate aphasia. The attentional profiles
across participants also varied. While the data for the outcome measures as a whole appear to indicate that the group
of participants responded more favorably to L-SAT than to
DAT, the individual profiles were mixed. For example, the
participants completed different numbers of L-SAT tasks,
and the levels of improvement across tasks varied from
small to large. Also, the results of standardized language
and attention testing for each participant were equivocal,
with different participants demonstrating different outcomes
regarding the effectiveness of treatment and the program
that produced the superior results. Of note, Participant 3
demonstrated the poorest language outcomes to either treatment as suggested by the summary score for his language
testing and his CADL-2 score. As this individual was the
participant who evolved from a nonfluent to a fluent aphasia,
these results may suggest that a participant with nonfluent
aphasia (or those who evolve from nonfluent aphasia) may
not be as good a candidate for L-SAT as a participant with
fluent aphasia. Caution is advised, however, in drawing such
a conclusion from a single individual. While the overall
outcomes regarding L-SAT are encouraging, further study
ideally employing a stronger design with a larger pool of
participants would provide additional data to test the comparative effectiveness of the two approaches to intervention
and to determine the profile(s) of participants with aphasia
who enjoy the greatest benefit from this type of treatment.
Also, none of the participants in the study completed
the full L-SAT program. This was a result of the constraints
on the schedule for L-SAT that arose from the design of
the study (i.e., pre- and posttreatment testing, two interventions, a washout period between interventions, and posttreatment follow-up). In a typical clinical environment,
such constraints on L-SAT delivery might be loosened so
that all of the tasks could be administered. Inasmuch as this
includes the most complex tasks of the program, participants might derive even greater benefit from the program
than that which was observed here. However, since no data
relating to the participants’ performance on these tasks
was available, it is unknown what contributions these tasks
might make, if any, to the outcomes associated with this
program. For these reasons, it will be important that the
Peach et al.: Language-Specific Attention Treatment for Aphasia
Downloaded from: https://pubs.asha.org Richard Peach on 08/16/2019, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions
2803
�full L-SAT program be administered in any future studies
of L-SAT to fully gauge the effectiveness of this program
as written or whether modifications may be in order.
Finally, all of the participants met criterion for the
Attention Allocation task after initial exposure or during
baseline testing. Thus, the treatment portion of this task
was not administered to any of the participants. Recall that
the task requires participants to identify a target word from
a list of monosyllabic words presented auditorily while
completing a card sorting task simultaneously. The score
for the task is the number of target words identified correctly
(LaPointe & Erickson, 1991). But given that the directions
for this task as administered emphasize the identification of
the target words while sorting, it is very likely that the
participants allocated their attention primarily to the word
lists while focusing attention secondarily to the card sorting
task. This then could result in a high rate of accuracy for
target word identification with perhaps a high degree of
inaccuracy for the sorting task. This may have contributed to
the scores observed for these participants on this task. In
order for this task to index attention allocation more reliably,
scoring should include both the number of target words identified correctly and the number of card sorts performed correctly. Going forward, we would recommend that the
scoring for this task include performance on both of these
components. Based on the data reported by LaPointe and
Erickson (1991) for their PWA, we would recommend using
concurrent scores of 80% accuracy on the word identification task and 50% accuracy on the card sorting task twice
consecutively as the criteria for advancement. This change
has now been incorporated into the program protocol.
Conclusion
L-SAT provides a domain-specific approach to
attention-related language rehabilitation following aphasia
that results in relatively stronger clinical outcomes than
those observed with a domain-general approach. The program is based on known principles of learning, is consistent with current practice guidelines, and appears to be
ecologically valid in that the treatment tasks are largely
equivalent to the skills to which they are expected to generalize. While further investigation of this program is warranted, the results suggest that L-SAT is an effective tool
for managing language disability due to aphasia.
Acknowledgment
This work was supported by faculty research grants from the
College of Health Sciences, Rush University, Chicago, Illinois.
References
American Speech-Language-Hearing Association. (2016). Scope of
practice in speech-language pathology [Scope of practice].
Retrieved from http://www.asha.org/policy/
Barlow, D. H., & Hayes, S. C. (1979). Alternating treatments design: One strategy for comparing the effects of two treatments
2804
in a single subject. Journal of Applied Behavior Analysis, 12(2),
199–210.
Barlow, D. H., Nock, M., & Hersen, M. (2009). Single case experimental designs: Strategies for studying behavior for change
(3rd ed.). Boston, MA: Pearson.
Beeson, P. M., & Robey, R. R. (2006). Evaluating single-subject
treatment research: Lessons learned from the aphasia literature.
Neuropsychology Review, 16(4), 161–169.
Boyle, M. (2004). Semantic feature analysis treatment for anomia
in two fluent aphasia syndromes. American Journal of SpeechLanguage Pathology, 13, 236–249.
Boyle, M., & Coelho, C. A. (1995). Application of semantic feature
analysis as a treatment for aphasic dysnomia. American Journal
of Speech-Language Pathology, 4(4), 94–98.
Brookshire, R. H., & Nicholas, L. E. (1997). Discourse Comprehension Test: Test manual. Minneapolis, MN: BRK Publishers.
Brossart, D. F., Laird, V. C., & Armstrong, T. W. (2018). Interpreting Kendall’s tau and Tau-U for single-case experimental
designs. Cogent Psychology, 5(1), Article ID 1518687.
Busk, P. L., & Serlin, R. C. (1992). Meta-analysis for single case
research. In T. R. Kratochwill & J. R. Levin (Eds.), Singlecase research design and analysis: New directions for psychology
and education (pp. 187–212). Hillsdale, NJ: Erlbaum.
Campbell, K. L., & Tyler, L. K. (2018). Language-related domainspecific and domain-general systems in the human brain. Current Opinion in Behavioral Sciences, 21, 132–137.
Caplan, D., & Waters, G. S. (1999). Verbal working memory and sentence comprehension. Behavioral and Brain Sciences, 22(1), 77–94.
Cherney, L. R., Kaye, R. C., & van Vuuren, S. (2014). Acquisition
and maintenance of scripts in aphasia: A comparison of two
cuing conditions. American Journal of Speech-Language Pathology, 23(2), S343–S360.
Cherney, L. R., Patterson, J. P., & Raymer, A. M. (2011). Intensity of aphasia: Evidence and efficacy. Current Neurology and
Neuroscience Reports, 11, 560–569.
Code, C. (2018). Aphasia is not a disorder of language: Discuss
[Abstract]. Aphasiology, 32(Supp. 1), 52–53.
Coelho, C. (2005). Direct attention training as a treatment for reading impairment in mild aphasia. Aphasiology, 19(3), 275–283.
Coelho, C., Sinotte, M., & Duffy, J. (2008). Schuell’s stimulation
approach to rehabilitation. In R. Chapey (Ed.), Language intervention strategies in aphasia and related neurogenic communication disorders (5th ed., pp. 403–449). Philadelphia, PA:
Lippincott Williams & Wilkins.
Cohen, J. (1988). Statistical power analysis for the behavioral sciences
(2nd ed.). Hillsdale, NJ: Erlbaum.
Connor, L. T., Albert, M. L., Helm-Estabrooks, N., & Obler, L. K.
(2000). Attentional modulation of language performance.
Brain and Language, 71(1), 52–55.
Conroy, P., Sage, K., & Lambon Ralph, M. A. (2009). The effects
of decreasing and increasing cue therapy on improving naming
speed and accuracy for verbs and nouns in aphasia. Aphasiology, 23(6), 707–730.
Coslett, H. B. (1999). Spatial influences on motor and language
function. Neuropsychologia, 37(6), 695–706.
Crawford, J. R. (2018). Computer programs for research and practice
in neuropsychology/clinical psychology. Retrieved from https://
homepages.abdn.ac.uk/j.crawford/pages/dept/psychom.htm
Crawford, J. R., Sommerville, J., & Robertson, I. H. (1997). Assessing the reliability and abnormality of subtest differences on
the Test of Everyday Attention. British Journal of Clinical
Psychology, 36(4), 609–617.
Crosson, B., & Cohen, M. L. (2012). Language and communication disorders associated with attentional deficits. In R. K.
Journal of Speech, Language, and Hearing Research • Vol. 62 • 2785–2811 • August 2019
Downloaded from: https://pubs.asha.org Richard Peach on 08/16/2019, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions
�Peach & L. P. Shapiro (Eds.), Cognition and acquired language
disorders: An information processing approach (pp. 167–182).
St. Louis, MO: Elsevier Mosby.
Crosson, B., Fabrizio, K. S., Singletary, F., Cato, M. A., Wierenga,
C. E., Parkinson, R. B., . . . Rothi, L. J. (2007). Treatment of
naming in nonfluent aphasia through manipulation of intention
and attention: A phase 1 comparison of two novel treatments.
Journal of the International Neuropsychological Society, 13,
582–594.
Cutler, A., & Fodor, J. A. (1979). Semantic focus and sentence
comprehension. Cognition, 7(1), 49–59.
Davis, G. (2005). PACE revisited. Aphasiology, 19(1), 21–38.
Difrancesco, S., Pulvermüller, F., & Mohr, B. (2012). Intensive
Language–Action Therapy (ILAT): The methods. Aphasiology,
26(11), 1317–1351.
Dotson, V. M., Singletary, F., Fuller, R., Koehler, S., Moore, A. B.,
Gonzalez Rothi, L. J., & Crosson, B. (2008). Treatment of wordfinding deficits in fluent aphasia through the manipulation
of spatial attention: Preliminary finding. Aphasiology, 22(1),
103–113.
Druks, J., & Masterson, J. (2000). An Object and Action Naming
Battery. London, United Kingdom: Psychology Press.
Edmonds, L. A., Nadeau, S. E., & Kiran, S. (2009). Effect of Verb
Network Strengthening Treatment (VNeST) on lexical retrieval
of content words in sentences in persons with aphasia. Aphasiology, 23(3), 402–424.
Elman, R. J., & Bernstein-Ellis, E. (1999). The efficacy of group
communication treatment in adults with chronic aphasia.
Journal of Speech, Language, and Hearing Research, 42(2),
411–419.
Fedorenko, E., & Thompson-Schill, S. L. (2014). Reworking the
language network. Trends in Cognitive Sciences, 18(3), 120–126.
Goodglass, H., & Kaplan, E. (1983). The assessment of aphasia
and related disorders (2nd ed.). Philadelphia, PA: Lea & Febiger.
Granier, J. P., Robin, D. A., Shapiro, L. P., Peach, R. K., &
Zimba, L. D. (2000). Measuring processing load during
sentence comprehension: Visuomotor tracking. Aphasiology,
14(5), 501–513.
Grodzinsky, Y. (1986). Language deficits and the theory of syntax.
Brain and Language, 27(1), 135–159.
Gronwall, D. M. (1977). Paced auditory serial-addition task: A
measure of recovery from concussion. Perceptual and Motor
Skills, 44(2), 367–373.
Hart, T., & Bagiella, E. (2012). Design and implementation of
clinical trials in rehabilitation research. Archives of Physical
Medicine and Rehabilitation, 93(8), S117–S126.
Hartwigsen, G. (2018). Flexible redistribution in cognitive networks.
Trends in Cognitive Sciences, 22(8), 687–698.
Helm-Estabrooks, N., Connor, L. T., & Albert, M. L. (2000). Treating attention to improve auditory comprehension in aphasia.
Brain and Language, 74, 469–472.
Henderson, A., Kim, H., Kintz, S., Frisco, N., & Wright, H. H.
(2017). Working memory in aphasia: Considering discourse
processing and treatment implications. Seminars in Speech and
Language, 38(1), 40–51.
Holland, A. L., Frattali, C., & Fromm, D. (1999). Communication
Activities of Daily Living–Second Edition: CADL-2. Austin, TX:
Pro-Ed.
Hula, W. D., Donovan, N. J., Kendall, D. L., & Gonzalez-Rothi,
L. J. (2010). Item response theory analysis of the Western
Aphasia Battery. Aphasiology, 24(11), 1326–1341.
Hula, W. D., & McNeil, M. R. (2008). Models of attention and
dual-task performance as explanatory constructs in aphasia.
Seminars in Speech and Language, 29(3), 169–187.
Jacobs, B. J., & Thompson, C. K. (2000). Cross-modal generalization effects of training noncanonical sentence comprehension
and production in agrammatic aphasia. Journal of Speech,
Language, and Hearing Research, 43(1), 5–20.
Kalinyak-Fliszar, M., Kohen, F., & Martin, N. (2011). Remediation of language processing in aphasia: Improving activation
and maintenance of linguistic representations in (verbal) shortterm memory. Aphasiology, 25(10), 1095–1131.
Katz, R. C., & Wertz, R. T. (1997). The efficacy of computerprovided reading treatment for chronic aphasic adults.
Journal of Speech, Language, and Hearing Research, 40(3),
493–507.
Kendall, D. L., Oelke, M., Brookshire, C. E., & Nadeau, S. E. (2015).
The influence of phonomotor treatment on word retrieval
abilities in 26 individuals with chronic aphasia: An open trial.
Journal of Speech, Language, and Hearing Research, 58(3),
798–812.
Kertesz, A. (2007). Western Aphasia Battery–Revised. San Antonio,
TX: The Psychological Corporation.
Kiran, S. (2007). Complexity in the treatment of naming deficits. American Journal of Speech-Language Pathology, 16(1),
18–29.
Kiran, S., Sandberg, C., & Abbott, K. (2009). Treatment for lexical retrieval using abstract and concrete words in persons
with aphasia: Effect of complexity. Aphasiology, 23(7–8),
835–853.
Kiran, S., & Thompson, C. (2003). The role of semantic complexity in treatment of naming deficits: Training semantic categories
in fluent aphasia by controlling exemplar typicality. Journal of
Speech, Language, and Hearing Research, 46, 773–787.
Kohnert, K. (2004). Cognitive and cognate-based treatments for
bilingual aphasia: A case study. Brain and Language, 91(3),
294–302. https://doi.org/10.1016/j.bandl.2004.04.001
Langacker, R. L. (2008). Complex sentences. Cognitive grammar:
A basic introduction (pp. 406–453). New York, NY: Oxford
University Press.
LaPointe, L. L., & Erickson, R. J. (1991). Auditory vigilance during divided task attention in aphasic individuals. Aphasiology,
5(6), 511–520.
Lee, J. B., & Cherney, L. R. (2018). Tau-U: A quantitative approach
for analysis of single-case experimental data in aphasia. American
Journal of Speech-Language Pathology, 27(1S), 495–503.
Lee, J. B., & Sohlberg, M. M. (2013). Evaluation of attention training and metacognitive facilitation to improve reading comprehension in aphasia. American Journal of Speech-Language
Pathology, 22(2), S318–S333.
Lee, J. B., Sohlberg, M. M., Harn, B., Horner, R., & Cherney, L. R.
(2018). Attention Process Training–3 to improve reading comprehension in mild aphasia: A single-case experimental design
study. Neuropsychological Rehabilitation. https://doi.org/10.
1080/09602011.2018.1477683
Loetscher, T., & Lincoln, N. B. (2013). Cognitive rehabilitation
for attention deficits following stroke. Cochrane Database of
Systematic Reviews, 31(5). https://doi.org//10.1002/14651858.
CD002842.pub2
MacLeod, C. M. (1992). The Stroop task: The “gold standard”
of attentional measures. Journal of Experimental Psychology:
General, 121(1), 12.
Martin, N., Fink, R. B., Renvall, K., & Laine, M. (2006). Effectiveness of contextual repetition priming treatments for anomia
depends on intact access to semantics. Journal of the International Neuropsychological Society, 12(6), 853–866.
Martin, N., Kohen, F., Kalinyak-Fliszar, M., Soveri, A., & Laine, M.
(2012). Effects of working memory load on processing of
Peach et al.: Language-Specific Attention Treatment for Aphasia
Downloaded from: https://pubs.asha.org Richard Peach on 08/16/2019, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions
2805
�sounds and meanings of words in aphasia. Aphasiology, 26(3–4),
462–493.
Maxwell, D. L., & Satake, E. (1997). Research and statistical
methods in communication disorders. Baltimore, MD: Williams
& Wilkins.
McNeil, M. R., Doyle, P., Hula, W., Rubinsky, H., Fossett, T., &
Matthews, C. (2004). Using resource allocation theory and
dual-task methods to increase the sensitivity of assessment in
aphasia. Aphasiology, 18(5), 521–542.
McNeil, M. R., Hula, W., & Sung, J. E. (2011). The role of memory
and attention in aphasic language performance. In J. Guendouzi,
F. Loncke, & M. J. Williams (Eds.), The handbook of psycholinguistic and cognitive processes (pp. 551–577). New York, NY:
Psychology Press.
McNeil, M. R., Odell, K., & Tseng, C. H. (1991). Toward the integration of resource allocation into a general theory of aphasia.
Clinical Aphasiology, 20, 21–39.
Minkina, I., Rosenberg, S., Kalinyak-Fliszar, M., & Martin, N.
(2017). Short-term memory and aphasia: From theory to treatment. Seminars in Speech and Language, 38(1), 17–28.
Moreau, D., & Conway, A. R. A. (2014). The case for an ecological approach to cognitive training. Trends in Cognitive Sciences,
18(7), 334–336. https://doi.org/10.1016/j.tics.2014.03.009
Murray, L., Keeton, R. J., & Karcher, L. (2006). Treating attention
in mild aphasia: Evaluation of Attention Process Training–II.
Journal of Communication Disorders, 39, 37–61.
Murray, L., & Mayer, J. (2017). Aphasia and related neurogenic
communication disorders. In I. Papathanasiou & P. Coppens
(Eds.), Extralinguistic cognitive consideration in aphasia management (2nd ed., pp. 129–149). Burlington, MA: Jones & Bartlett
Learning.
Myachykov, A., & Posner, M. I. (2005). Attention in language. In
L. Itti, G. Rees, & J. Tsotsos (Eds.), Neurobiology of attention
(pp. 324–329). Waltham, MA: Elsevier.
Park, N. W., & Barbuto, E. (2005). Treating attention impairments: Review with a particular focus on naturalistic action
rehabilitation. In P. W. Halligan & D. T. Wade (Eds.), The
effectiveness of rehabilitation for cognitive deficits. (pp. 81–90).
New York, NY: Oxford University Press.
Park, N. W., & Ingles, J. L. (2001). Effectiveness of attention rehabilitation after an acquired brain injury: A meta-analysis.
Neuropsychology, 15(2), 199.
Park, N. W., Proulx, G., & Towers, W. M. (1999). Evaluation of
the attention process training programme. Neuropsychological
Rehabilitation, 9(2), 135–154.
Parker, R. I., Vannest, K. J., Davis, J. L., & Sauber, S. B. (2011).
Combining nonoverlap and trend for single-case research:
Tau-U. Behavior Therapy, 42(2), 284–299.
Paul, D., Frattali, C., Holland, A., Thompson, C., Caperton, C., &
Slater, S. (2004). ASHA Quality of Communication Life Scale
(QCL): Manual. Rockville, MD: American Speech-LanguageHearing Association.
Peach, R. K. (1987). A short-term memory treatment approach to
the repetition deficit in conduction aphasia. Clinical Aphasiology,
17, 35–45.
Peach, R. K. (1993). Clinical intervention for aphasia in the
United States of America. In A. L. Holland & M. M. Forbes
(Eds.), Aphasia treatment: World perspectives (pp. 335–369).
San Diego, CA: Singular.
Peach, R. K. (1996). Treatment for aphasic phonological output
planning deficits. Clinical Aphasiology, 24, 109–120.
Peach, R. K. (2001). Further thoughts regarding management of
acute aphasia following stroke. American Journal of SpeechLanguage Pathology, 10, 29–36.
2806
Peach, R. K. (2012). Management of acquired language disorders
associated with attentional impairment. In R. K. Peach & L. P.
Shapiro (Eds.), Cognition and acquired language disorders: An
information processing approach (pp. 241–274). St. Louis, MO:
Elsevier Mosby.
Peach, R. K., Nathan, M. R., & Beck, K. M. (2017). Languagespecific attention treatment for aphasia: Description and preliminary findings. Seminars in Speech and Language, 38(1), 5–16.
https://doi.org/10.1055/s-0036-1597260
Peach, R. K., Newhoff, M., & Rubin, S. S. (1993). Attention in
aphasia as revealed by event-related potentials: A preliminary
investigation. Clinical Aphasiology, 21, 323–333.
Peach, R. K., & Reuter, K. A. (2010). A discourse-based approach
to semantic feature analysis for the treatment of aphasic word
retrieval failures. Aphasiology, 24(9), 971–990.
Peach, R. K., Rubin, S. S., & Newhoff, M. (1994). A topographic
event-related potential analysis of the attention deficit for
auditory processing in aphasia. Clinical Aphasiology, 22,
81–96.
Peach, R. K., Schenk, K. A., Nathan, M. R., & Beck, K. M. (2018).
Construct validity, external validity, and reliability for a battery
of language-specific attention tasks. Aphasiology, 32(6), 618–645.
Peach, R. K., & Wong, P. C. M. (2004). Integrating the message
level into treatment for agrammatism using story retelling.
Aphasiology, 18(5/6/7), 429–441.
Peers, P. V., Astle, D. E., Duncan, J., Murphy, F. C., Hampshire, A.,
Das, T., & Manly, T. (2018). Dissociable effects of attention vs
working memory training on cognitive performance and everyday functioning following fronto-parietal strokes. Neuropsychological Rehabilitation. Advance online publication. https://doi.
org/10.1080/09602011.2018.1554534
Pella, R. D., Kendra, K., Hill, B. D., & Gouvier, W. D. (2008).
Cognitive rehabilitation with brain-damaged patients. In A. M.
Horton & D. Wedding (Eds.), The neuropsychology handbook
(3rd ed., pp. 419–467). New York, NY: Springer Publishing
Company.
Piantadosi, S. (2005). Clinical trials: A methodologic perspective.
Crossover designs (2nd ed., pp. 515–527). Hoboken, NJ: WileyInterscience.
Ponsford, J., Bayley, M., Wiseman-Hakes, C., Togher, L., Velikonja,
D., McIntyre, A., . . . INCOG Expert Panel. (2014). INCOG
recommendations for management of cognition following traumatic brain injury, Part II: Attention and information processing speed. Journal of Head Trauma Rehabilitation, 29(4),
321–337.
Ponsford, J., & Kinsella, G. (1991). The use of a rating scale of
attentional behaviour. Neuropsychological Rehabilitation, 1(4),
241–257.
Psychometric Conversion Table. (n.d.). Retrieved from https://
www.ritenour.k12.mo.us/cms/lib011/MO01910124/Centricity/
Domain/69/Psychometric_Conversion_Table.pdf
Ramsberger, G. (2005). Achieving conversational success in
aphasia by focusing on non-linguistic cognitive skills: A potentially promising new approach. Aphasiology, 19(10–11),
1066–1073.
Rao, S. M., Leo, G. J., Bernardin, L., & Unverzagt, F. (1991).
Cognitive dysfunction in multiple sclerosis. I. Frequency, patterns, and prediction. Neurology, 41(5), 685–691.
Raymer, A., & Ellsworth, T. (2002). Response to contrasting verb
retrieval treatments: A case study. Aphasiology, 16(10/11),
1031–1045.
Renvall, K., Laine, M., & Martin, N. (2005). Contextual priming
in semantic anomia: A case study. Brain and Language, 95(2),
327–341.
Journal of Speech, Language, and Hearing Research • Vol. 62 • 2785–2811 • August 2019
Downloaded from: https://pubs.asha.org Richard Peach on 08/16/2019, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions
�Robertson, I. H., Ward, T., Ridgeway, V., & Nimmo-Smith, I. (1994).
The Test of Everyday Attention. Suffolk, United Kingdom:
Thames Valley Test Company.
Rochon, E., Laird, L., Bose, A., & Scofield, J. (2005). Mapping
therapy for sentence production impairments in nonfluent
aphasia. Neuropsychological Rehabilitation, 15(1), 1–36.
Rogers, T. T., Patterson, K., Jefferies, E., & Ralph, M. A. L. (2015).
Disorders of representation and control in semantic cognition:
Effects of familiarity, typicality, and specificity. Neuropsychologia, 76, 220–239.
Rohling, M. L., Faust, M. E., Beverly, B., & Demakis, G. (2009).
Effectiveness of cognitive rehabilitation following acquired brain
injury: A meta-analytic re-examination of Cicerone et al.’s
(2000, 2005) systematic reviews. Neuropsychology, 23(1), 20–39.
Rubin, S. S., Newhoff, M., Peach, R. K., & Shapiro, L. P. (1996).
Electrophysiological indices of lexical processing: The effects
of verb complexity and age. Journal of Speech and Hearing
Research, 39(5), 1071–1080.
Salis, C. (2012). Short-term memory treatment: Patterns of learning
and generalisation to sentence comprehension in a person
with aphasia. Neuropsychological Rehabilitation, 22(3),
428–448.
Salis, C., Hwang, F., Howard, D., & Lallini, N. (2017). Short-term
and working memory treatments for improving sentence
comprehension in aphasia: A review and a replication study.
Seminars in Speech and Language, 38(1), 29–39.
Schneider, J. (2002, May). Block letter eye chart. Retrieved from
http://eyetestnow.com/images/snellen_block_letter_eye_chart_
eye_exam_test.pdf
Schuell, H., & Jenkins, J. J. (1959). The nature of language deficit
in aphasia. Psychological Review, 66(1), 45–67.
Schuell, H., Jenkins, J. J., & Jimenez-Pabon, E. (1964). Aphasia
in adults. New York, NY: Harper & Row.
Shankweiler, D., Crain, S., Gorrell, P., & Tuller, B. (1989). Reception of language in Broca’s aphasia. Language and Cognitive
Processes, 4(1), 1–33.
Simonet, M., von Roten, F. C., Spierer, L., & Barral, J. (2019).
Executive control training does not generalize, even when associated with plastic changes in domain-general prefrontal areas.
NeuroImage, 197, 457–469.
Sinotte, M. P., & Coelho, C. A. (2007). Attention training for
reading impairment in mild aphasia: A follow-up study. Neurorehabilitation, 22, 303–310.
Sohlberg, M. M., Johnson, L., Paule, L., Raskin, S. A., & Mateer,
C. A. (2001). Attention Process Training–II: A program to address attentional deficits for persons with mild cognitive dysfunction (2nd ed.). Wake Forest, NC: Lash & Associates.
Sohlberg, M. M., & Mateer, C. A. (2010). Attention Process
Training APT-3: A direct attention training program for persons
with acquired brain injury. Wake Forest, NC: Lash & Associates.
Sturm, W., Fimm, B., Cantagallo, A., Cremel, N., North, P.,
Passadori, A., . . . Leclercq, M. (2003). Specific computerized
attention training in stroke and traumatic brain-injured patients. Zeitschrift Für Neuropsychologie, 14(4), 283–292.
Sturm, W., Longoni, F., Weis, S., Specht, K., Herzog, H., Vohn, R.,
. . . Willmes, K. (2004). Functional reorganisation in patients with
right hemisphere stroke after training of alertness: A longitudinal PET and fMRI study in eight cases. Neuropsychologia,
42, 434–450. https://doi.org/10.1016/j.neuropsychologia.2003.09.
001
Sturm, W., Willmes, K., Orgass, B., & Hartje, W. (1997). Do specific attention deficits need specific training? Neuropsychological Rehabilitation, 7(2), 81–103.
Talmy, L. (2003). Toward a cognitive semantics, Volume I: Concept
structuring systems. The windowing of attention in language
(pp. 258–309). Cambridge, MA: MIT Press.
Thompson, C. K., Ballard, K. J., & Shapiro, L. P. (1998). The role
of syntactic complexity in training wh-movement structures in
agrammatic aphasia: Optimal order for promoting generalization. Journal of the International Neuropsychological Society,
4(6), 661–674.
Thompson, C. K., & Shapiro, L. P. (2005). Treating agrammatic
aphasia within a linguistic framework: Treatment of underlying forms. Aphasiology, 19(10–11), 1021–1036.
Thompson, C. K., & Shapiro, L. P. (2007). Complexity in treatment
of syntactic deficits. American Journal of Speech-Language
Pathology, 16(1), 30–42.
Thompson, C. K., Shapiro, L. P., Kiran, S., & Sobecks, J. (2003).
The role of syntactic complexity in treatment of sentence deficits
in agrammatic aphasia: The Complexity Account of Treatment
Efficacy (CATE). Journal of Speech, Language, and Hearing
Research, 46, 591–607.
Tseng, C., McNeil, M. R., & Milenkovic, P. (1993). An investigation of attention allocation deficits in aphasia. Brain and Language, 45(2), 276–296.
Vannest, K., Parker, R., Gonen, O. & Adiguzel, T. (2011). Single
case research: Web based calculators for SCR analysis. Retrieved
from http://www.singlecaseresearch.org
Villard, S., & Kiran, S. (2017). To what extent does attention underlie language in aphasia? Aphasiology, 31(10), 1226–1245.
Villard, S., & Kiran, S. (2018). Between-session and within-session
intra-individual variability in attention in aphasia. Neuropsychologia, 109, 95–106.
Wambaugh, J., Cameron, R., Kalinyak-Fliszar, M., Nessler, C., &
Wright, S. (2004). Retrieval of action names in aphasia: Effects of two cueing treatments. Aphasiology, 18(11), 979–1004.
Wechsler, D. (1981). Manual for the Wechsler Adult Intelligence
Scale–Revised. New York, NY: The Psychological Corporation.
Wepman, J. M. (1972). Aphasia therapy: A new look. Journal of
Speech and Hearing Disorders, 37(2), 203–214.
Wepman, J. M., Jones, L. V., Bock, R. D., & Van Pelt, D.
(1960). Studies in aphasia: Background and theoretical formulations. Journal of Speech and Hearing Disorders, 25(4), 323–332.
Wilson, B. A., Emslie, H. C., Quirk, K., & Evans, J. J. (2001).
Reducing everyday memory and planning problems by means
of a paging system: A randomised control crossover study.
Journal of Neurology, Neurosurgery & Psychiatry, 70(4),
477–482.
Wright, H. H., & Shisler, R. J. (2005). Working memory in aphasia:
Theory, measures, and clinical implications. American Journal
of Speech-Language Pathology, 14, 107–118.
Zickefoose, S., Hux, K., Brown, J., & Wulf, K. (2013). Let the games
begin: A preliminary study using Attention Process Training–3
and Lumosity™ brain games to remediate attention deficits
following traumatic brain injury. Brain Injury, 27(6), 707–716.
https://doi.org/10.3109/02699052.2013.775484
Peach et al.: Language-Specific Attention Treatment for Aphasia
Downloaded from: https://pubs.asha.org Richard Peach on 08/16/2019, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions
2807
�2808
Appendix A ( p. 1 of 3)
L-SAT Treatment Program
Journal of Speech, Language, and Hearing Research • Vol. 62 • 2785–2811 • August 2019
Attention manipulation
Lexical processing
Spatial Attention
Attention Allocation
Sentence processing
Object Manipulation
Topicalization
Phase
No. of items
A
40
B
40
C
40
A
3 Trials, 25 targets,
75 foils/trial
B
3 Trials, 25 targets,
75 foils/trial
A
20
B
14
20 Sentences,
40 questions
Treatment stimuli, tasks, cues, therapeutic operations, and advancement criteria
Present simultaneous visual (fireworks) and auditory (4-s tone) warning signals and line drawings alternately on a
computer monitor placed 45° to the left of the patient’s midline. Lexical items randomized for varying levels of
frequency of occurrence (high, medium, low). Patient names each item on confrontation (20 s maximum). If
patient provides incorrect name, correct response is modeled and patient repeats it. No more than three models
per item. Criterion for advancement to next phase: 32 or more correct responses over two consecutive trials.
Present auditory (4-s tone) warning signal and line drawings alternately on a computer monitor placed 45° to the left
of the patient’s midline. Lexical items randomized for varying levels of frequency of occurrence (high, medium, low).
Patient names each item on confrontation (20 s maximum). If patient provides incorrect name, correct response is
modeled and patient repeats it. No more than three models per item. Criterion for advancement to next phase: 32
or more correct responses over two consecutive trials.
Present auditory (0.5-s tone) warning signal and line drawings alternately on a computer monitor placed 45° to the left
of the patient’s midline. Lexical items randomized for varying levels of frequency of occurrence (high, medium, low).
Patient names each item on confrontation (20 s maximum). If patient provides incorrect name, correct response is
modeled and patient repeats it. No more than three models per item. Criterion for completion of task: 32 or more
correct responses over two consecutive trials.
Patient listens to monosyllabic word lists and raises hand when target word is heard (auditory attention). If patient
demonstrates 20 or more correct responses on any trial with no cueing, advance to Phase B. If patient demonstrates
fewer than 20 correct responses, repeat trial with cueing and then proceed to next trial. Cues consist of auditory
attention strategies (i.e., self-monitor, rehearse, listen and anticipate, repeat) alone or in combination with written
cues (printed target word). As accuracy increases in combined cueing condition, visual cue is withdrawn systematically
(100%, 75%, 50%, or 25% of trials).
Patient listens to monosyllabic word lists and raises hand when target word is heard while simultaneously completing
card sorting task (dual task attention). If patient demonstrates 20 or more correct responses on two consecutive
trials, discontinue task. If patient demonstrates fewer than 20 correct responses, repeat trial with cueing and then
proceed to next trial. Cues consist of auditory attention strategies (i.e., self-monitor, rehearse, listen and anticipate,
repeat) alone or in combination with written cues (printed target word). As accuracy increases in combined cueing
condition, visual cue is withdrawn systematically (100%, 75%, 50%, or 25% of trials).
Patient provided cues for syntactic subjects of sentences and then manipulates objects to demonstrate correct
actions in semantically reversible sentences. Ten active sentences and 10 passive sentences with two-place verb
argument structure presented in random order. For incorrect responses, sentence is repeated, clinician models the
correct relationship, and then patient performs the correct action. Criterion for advancement to next phase: 16 or
more accurate responses over two consecutive trials.
Patient provided cues for syntactic subjects of sentences and then manipulates objects to demonstrate correct actions
in semantically reversible sentences. Seven active sentences and seven passive sentences with three-place verb
argument structure presented in random order. For incorrect responses, sentence is repeated, clinician models
the correct relationship, and then patient performs the correct action. Criterion for completion of task: 12 or more
accurate responses over two consecutive trials.
Twenty topicalized sentences (e.g., “Blue, the hat was, that the man on the corner was wearing”) presented orally to
patient followed by two comprehension questions for each sentence. Question A targets sentence topic (e.g.,
“Which hat was the man wearing? The blue hat.”). Question B targets remaining information (e.g., “Which man was
wearing the hat? The man on the corner.”). If patient does not answer Question A correctly, auditory cues provided
to promote attention strategies (self-monitoring, rehearsal, listening and anticipating, repetition). May be combined with
visual cues (printed sentences). Cues reduced systematically as response accuracy increases. If patient does not
answer Question B correctly, feedback provided and correct answer modeled. No further cueing. Criterion for task
completion: 32 or more correct responses over two consecutive trials.
(table continues)
Downloaded from: https://pubs.asha.org Richard Peach on 08/16/2019, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions
�Appendix A ( p. 2 of 3)
.L-SAT Treatment Program
Attention manipulation
Anaphora
Peach et al.: Language-Specific Attention Treatment for Aphasia
Nominal Grounding
Phase
No. of items
A
20 Sentences,
20 questions
B
20 Sentences,
20 questions
C
20 Sentences,
20 questions
A
20 Sentences,
20 questions
B
20 Sentences,
20 questions
C
20 Sentences,
20 questions
Treatment stimuli, tasks, cues, therapeutic operations, and advancement criteria
Twenty sentences presented orally with close syntactic distance between referents and anaphoric pronouns and low
load on working memory. Patient responds to a comprehension question for each sentence regarding referent of
anaphoric pronoun (e.g., “Jasmine stayed after she finished the meal. Who finished the meal?”). If patient does
not answer question correctly, auditory cues provided to promote attention strategies (self-monitoring, rehearsal,
listening and anticipating, repetition). May be combined with visual cues (printed target). Cues reduced systematically
as response accuracy increases. Criterion for advancement to Phase B: 16 or more correct responses over two
consecutive trials.
Twenty sentences presented orally with increased syntactic distance between referents and anaphoric pronouns and
medium load on working memory. Patient responds to a comprehension question for each sentence regarding
referent of anaphoric pronoun (e.g., “Tim argued with Kelly during the movie because she forgot to buy popcorn.
Who forgot to buy popcorn?”). If patient does not answer question correctly, auditory cues provided to promote
attention strategies (self-monitoring, rehearsal, listening and anticipating, repetition). May be combined with visual
cues (printed target). Cues reduced systematically as response accuracy increases. Criterion for advancement to
Phase C: 16 or more correct responses over two consecutive trials.
Twenty sentences presented orally with long syntactic distance between referents and anaphoric pronouns and
high load on working memory. Patient responds to a comprehension question for each sentence regarding referent
of anaphoric pronoun (e.g., “The manager who questioned the teller from the local bank branch told the policeman
how he suspected her of fraud. Who did the manager suspect of fraud?”). If patient does not answer question
correctly, auditory cues provided to promote attention strategies (self-monitoring, rehearsal, listening and anticipating,
repetition). May be combined with visual cues (printed target). Cues reduced systematically as response accuracy
increases. Criterion for completion of task: 16 or more correct responses over two consecutive trials.
Twenty sentences presented orally varying by definite (the) or indefinite (a) articles. Patient responds to yes/no
comprehension questions for each sentence probing whether particular nouns are specific or nonspecific (e.g.,
“The girl in the class likes the boy. Do we know which boy the girl likes?” Correct answer = yes; “Tom found a
home for the boy. Do we know which home Tom found?” Correct answer = no). Ten sentences require positive
response, 10 sentences require negative response. If patient does not answer question correctly, auditory cues
provided to promote attention strategies (self-monitoring, rehearsal, listening and anticipating, repetition). May
be combined with visual cues (printed target). Cues reduced systematically as response accuracy increases.
Criterion for advancement to Phase B: 16 or more correct responses over two consecutive trials.
Twenty sentences presented orally varying by demonstrative pronouns (this, that, these, those). Patient responds to
yes/no comprehension questions for each sentence probing whether particular nouns are in proximity (e.g., “This
evidence should satisfy those detectives. Are the detectives close at hand?” Correct answer = no; “This book is
more interesting than that movie. Is the book close at hand?” Correct answer = yes). Ten sentences require positive
response, 10 sentences require negative response. If patient does not answer question correctly, auditory cues
provided to promote attention strategies (self-monitoring, rehearsal, listening and anticipating, repetition). May be
combined with visual cues (printed target). Cues reduced systematically as response accuracy increases. Criterion
for advancement to Phase C: 16 or more correct responses over two consecutive trials.
Twenty sentences presented orally varying by noun qualifiers (every, all, some, most, each, any). Patient responds to
yes/no comprehension questions for each sentence probing whether particular nouns are enhanced or limited
(e.g., “All of the guests enjoyed the party, but some guests left early. Did any of the guests enjoy the party?”
Correct answer = yes; “Every player is part of the team but some receive more playing time. Do all players receive
equal amounts of playing time?” Correct answer = no). Ten sentences require positive response, 10 sentences
require negative response. If patient does not answer question correctly, auditory cues provided to promote attention
strategies (self-monitoring, rehearsal, listening and anticipating, repetition). May be combined with visual cues
(printed target). Cues reduced systematically as response accuracy increases. Criterion for task completion: 16 or
more correct responses over two consecutive trials.
2809
(table continues)
Downloaded from: https://pubs.asha.org Richard Peach on 08/16/2019, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions
�2810
Journal of Speech, Language, and Hearing Research • Vol. 62 • 2785–2811 • August 2019
Appendix A ( p. 3 of 3)
.L-SAT Treatment Program
Attention manipulation
Phase
No. of items
Clausal Grounding
A
16 Sentences,
16 questions
B
16 Sentences,
16 questions
A
20 Sentence,
60 questions
B
20 Sentences,
40 questions
C
20 Sentences,
20 questions
Windowing
Treatment stimuli, tasks, cues, therapeutic operations, and advancement criteria
Sixteen sentences presented orally with varying verb tenses (present, past). Patient responds to yes/no comprehension
questions for each sentence probing specific meanings with respect to time (e.g., “The teacher announces that she
was tired. Is the teacher tired now?” Correct answer = no; “Sara exclaims that she is excited. Is Sara exclaiming that
she is excited now?” Correct answer = yes). Eight sentences require positive response, eight sentences require
negative response. If patient does not answer question correctly, auditory cues provided to promote attention
strategies (self-monitoring, rehearsal, listening and anticipating, repetition). May be combined with visual cues (printed
target). Cues reduced systematically as response accuracy increases. Criterion for advancement to Phase B: 12 or
more correct responses over two consecutive trials.
Sixteen sentences presented orally with varying modal verbs (will, can, may, must). Patient responds to yes/no
comprehension questions for each sentence probing specific meanings with respect to the possibility, probability,
or certainty of an event (e.g., “The editor can veto the book proposal. Is there a chance the editor won’t veto the
book proposal?” Correct answer = yes; “The student must pass his final exams. Is there a chance the student won’t
have to pass his final exams?” Correct answer = no). Eight sentences require positive response, eight sentences
require negative response. If patient does not answer question correctly, auditory cues provided to promote
attention strategies (self-monitoring, rehearsal, listening and anticipating, repetition). May be combined with
visual cues (printed target). Cues reduced systematically as response accuracy increases. Criterion for task
completion: 12 or more correct responses over two consecutive trials.
Twenty sentences presented orally describing a path event frame (the entirety of a path of motion). Patient responds
to wh-questions (what, where, how) that window (focus attention on) the paths taken by objects that are physically
in motion during a period of time and have beginning and ending points that are in different locations in space (open
paths). Questions elicit open path windowing for initial, medial, and final events in varying orders (e.g., “The ball
kicked by the defender flew like a missile on a straight shot to the goal. How was the ball kicked? What kind of kick
was it? Where did the ball go?”). If patient does not answer question correctly, auditory cues provided to promote
attention strategies (self-monitoring, rehearsal, listening and anticipating, repetition). May be combined with visual
cues (printed target). Cues reduced systematically as response accuracy increases. Criterion for advancement to
Phase B: 48 or more correct responses over two consecutive trials.
Twenty sentences presented orally describing a cycle event frame (an iterating cycle that is sequential but with no clear
beginning, middle, or end). Patient responds to questions that direct attention to the departure and return phases
of the event (phase windowing; e.g., “When the meal would get cold, I would keep reheating it. What did the meal
do? What did I do?”). If patient does not answer question correctly, auditory cues provided to promote attention
strategies (self-monitoring, rehearsal, listening and anticipating, repetition). May be combined with visual cues
(printed target). Cues reduced systematically as response accuracy increases. Criterion for advancement to
Phase C: 32 or more correct responses over two consecutive trials.
Twenty sentences presented orally describing a factuality event frame (establish comparison of alternative conceptualizations
for the occurrence/nonoccurrence of some referent). Patient responds to questions that heighten attention (factuality
windowing) for an unrealized positive or negative event, an event at the opposite end of a continuum of certainty, or
an overtly counterfactual event (e.g., “The salesman would have celebrated if he had exceeded his yearly quota. What
happened because the salesman did not exceed his yearly quota?”). If patient does not answer question correctly,
auditory cues provided to promote attention strategies (self-monitoring, rehearsal, listening and anticipating, repetition).
May be combined with visual cues (printed target). Cues reduced systematically as response accuracy increases.
Criterion for completion of task: 16 or more correct responses over two consecutive trials.
Downloaded from: https://pubs.asha.org Richard Peach on 08/16/2019, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions
�Appendix B
Direct Attention Training
Baseline Procedure
1.
Begin with the task listed for each component of attention. Complete only one trial of each task until baseline is determined.
Task hierarchy increases from easiest to hardest within each component. See program for complete list of tasks.
Sustained Attention–Auditory
Sustained Attention–Visual
Selective Attention–Auditory
Selective Attention–Visual
Working Memory
Suppression–Auditory
Suppression–Visual
Alternating Attention–Auditory
Alternating Attention–Visual
Listening for Two Letters Fast (Level 4)
Watching for Number Comparisons Hard–Fast (Level 10)
Listening for 2 Letters Fast–Environmental Noise (Level 16)
Watching for Number Comparisons (Hard)–Fast–White Noise (Level 34)
4-Number Sequences (0–100) Subtract 2 (Level 17)
Happy–Sad Fast–Button Response (Level 2)
Word Shapes Fast–Verbal Response (Level 8)
Happy-Sad Fast–Button Response (Level 2)
Word Shapes Fast–Button Response (Level 4)
2.
Move to next hardest level within the same task if performance is greater or equal to 90% accurate with a false-positive
(FP) rate of less than or equal to 10%; if performance is 100% accurate with an FP rate of less than 5%, move down to
next hardest task in hierarchy.
3.
Move up to next easiest task if performance is less than or equal to 60% accurate and/or if the FP rate is greater than 10%.
a.
If performance on a single task is less than or equal to 30% or the FP rate is greater than 50%, move up to next
easiest task.
b.
If performance for two consecutive tasks is less than 50% and/or the FP rate is greater than 25%, move up to next
easiest task.
4.
If performance on a task is greater than 60% and less than 90% accurate and the FP rate is less than 10%, use as the
starting point for treatment.
5.
If patient does not meet starting criteria for easiest task (Level 1) in hierarchy, begin here with goal of increasing accuracy
and reducing FP rate.
Peach et al.: Language-Specific Attention Treatment for Aphasia
Downloaded from: https://pubs.asha.org Richard Peach on 08/16/2019, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions
2811
�
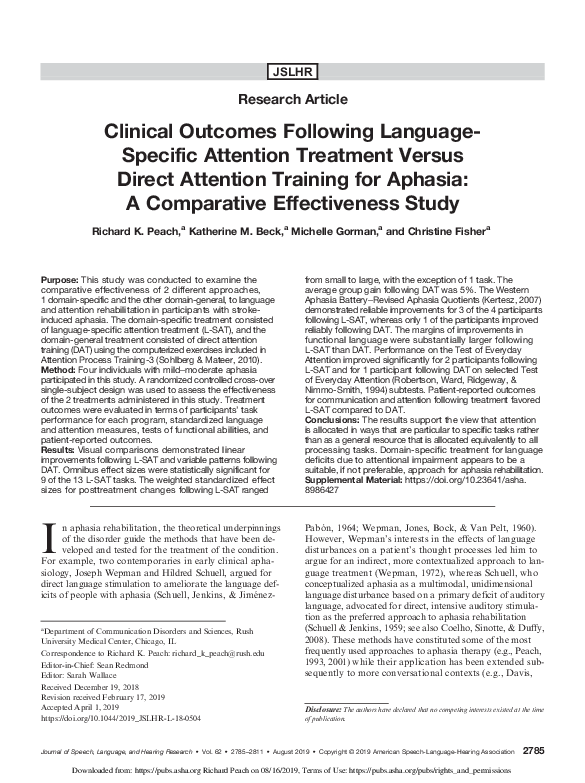
 Richard K Peach
Richard K Peach