Behavioural Brain Research 205 (2009) 67–75
Contents lists available at ScienceDirect
Behavioural Brain Research
journal homepage: www.elsevier.com/locate/bbr
Research report
Predictable stress versus unpredictable stress: A comparison
in a rodent model of stroke
Fabíola C.R. Zucchi, Scott W. Kirkland, Nafisa M. Jadavji, Linda T. van Waes,
Alexander Klein, Rebecca D. Supina, Gerlinde A. Metz ∗
Canadian Centre for Behavioural Neuroscience, University of Lethbridge, 4401 University Drive, Lethbridge, AB, Canada T1K 3M4
a r t i c l e
i n f o
Article history:
Received 27 January 2009
Received in revised form 15 June 2009
Accepted 23 June 2009
Available online 30 June 2009
Keywords:
Restraint stress
Variable stress
Skilled reaching
Skilled walking
Corticosterone levels
Ischemia
a b s t r a c t
Previous studies have associated stress with poor outcome in individuals affected by stroke. It was suggested that the effects of stress depend on the stressor’s type and strength. Here we compare the effects
of chronic predictable restraint stress and chronic unpredictable variable stress on motor recovery after
focal lesion in the rat motor cortex. Adult male rats were pre-trained and tested in skilled reaching and
skilled walking tasks. Animals were assigned to daily treatments of either restraint stress or variable stress
starting 1 week prior to lesion up to 2 weeks post-lesion. One group served as lesion only control. The
results revealed a distinct pattern of recovery and compensation of skilled movement. Animals exposed
to predictable restraint stress had significantly lower reaching success at both pre- and post-lesion time
points, and higher error rates in skilled walking when compared to lesion controls. Overall, restraint
stress induced more pronounced motor impairments prior to and after injury than variable stress. Variable stress increased the number of attempts required to grasp food pellets and changed movement
pattern performance. By contrast, variable stress improved limb placement accuracy when compared
to lesion controls. The behavioural changes were not accompanied by differences in infarct size. These
findings are in agreement with other studies reporting that both chronic predicable restraint stress and
unpredictable variable stress influence the course of recovery following stroke, however, restraint stress
might affect stroke recovery through a different route than variable stress.
© 2009 Elsevier B.V. All rights reserved.
1. Introduction
Cerebrovascular disease, such as stroke, is a leading cause of
disability. A major consequence of stroke is permanent motor disturbance, such as postural imbalance, gait abnormalities, and loss
of skilled movement [9,46,57]. The degree of neuronal and functional loss and subsequent recovery after stroke were shown to
be influenced by physiological variables, such as stress [25,38].
Stress and high levels of stress hormones are associated with poor
outcome after stroke in humans [41,39,7]. Studies in laboratory
rodents showed that stress delays or diminishes recovery of cognitive functions after cerebral ischemia [10,49]. Furthermore, stress
and elevated glucocorticoid (GC) levels, such as corticosterone,
diminish recovery of skilled movement after ischemic lesion of the
motor cortex [22].
It has been suggested that the effects of stress strongly depend
on the stressor’s type and strength [30,24]. While many previous studies in rats have used predictable restraint stress models
[22,35,55], others have argued that an unpredictable variable stress
∗ Corresponding author.
E-mail address: gerlinde.metz@uleth.ca (G.A. Metz).
0166-4328/$ – see front matter © 2009 Elsevier B.V. All rights reserved.
doi:10.1016/j.bbr.2009.06.030
paradigm might cause a closer association between stress and permanently elevated GC levels [40,26,45]. While repeated restraint
stress might allow for habituation as reflected by a decline in plasma
GC levels, a variable stress paradigm combines different stressors
in an unpredictable sequence to maintain elevated GC levels. To circumvent habituation, an effective stress paradigm that involves a
sequence of various psychological and physical stressors given at
random intervals was developed [15,54,13,28,3,4,27,42–44]. Studies of recovery from stroke have found that both restraint and
chronic variable stress influence the course of functional recovery after lesion [55,25,45]. Furthermore, previous findings suggest
that both elevated GC levels as well as stress-induced emotional
changes, such as anxiety, may affect recovery of motor function after
ischemic lesion [22]. While previous studies have used restraint
stress to examine the effects of stress on motor system function,
the present study is the first to explore the influence of stressor
type on motor performance.
The purpose of the present study was twofold. First, this study
investigated the influence of continuous restraint stress prior to
and after lesion on recovery and compensation in a rat model of
stroke. Second, this study compared the effects of chronic predictable restraint stress and chronic unpredictable variable stress
on recovery of skilled movement. Based on previous findings of
�68
F.C.R. Zucchi et al. / Behavioural Brain Research 205 (2009) 67–75
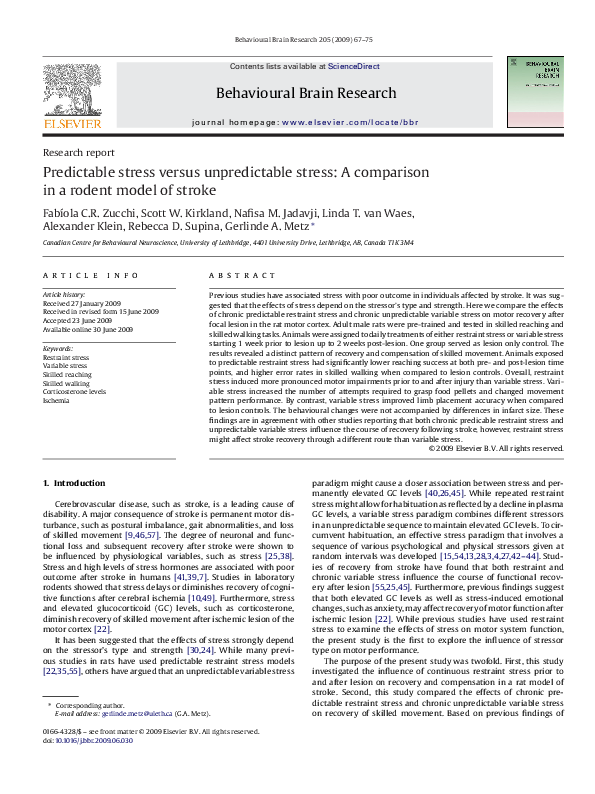
Fig. 1. Timeline of the experimental design. After 5 days of baseline testing, the Restraint & lesion and Variable & lesion groups underwent stress treatment for 8 days. On day
16 all experimental groups underwent devascularization lesion. Both stress regimens, restraint and variable, were continued for 15 days post-lesion. Skilled reaching tests
were performed daily for 30 days. Skilled reaching and skilled walking performance was video-recorded at baseline, pre-lesion (day 15) and post-lesion (day 30) time points.
Blood samples were taken on the last day of baseline testing (day 7), and the day before sacrifice (day 31).
replicable and discrete skilled movement deficits [60], a model of
focal motor cortex lesion was used to induce permanent loss of fine
motor control. The results reveal distinct patterns of recovery and
compensation of skilled movement as assessed in skilled reaching
and skilled walking tasks.
2. Materials and method
focal lesion of the motor cortex contralateral to the paw preferred in skilled reaching
was induced by devascularization [60] (Fig. 2A and B). Briefly, the skin over the skull
was incised and the skull was exposed. Using a fine dental burr, a craniotomy was
made at the following coordinates: −1.0 to 4.0 mm anterior–posterior to Bregma and
1.5–4.5 mm lateral to Bregma. The dura was removed, and the blood vessels were
carefully wiped off using a sterile cotton tip. Then the skin was sutured and the
rat was given analgesic (Temgesic, Schering–Plough, Brussels, Belgium). Rats were
allowed to recover in individual cages on a heating pad until fully awake and were
then returned to their home cages.
2.1. Animals
2.4. Stress paradigms
Fifty-nine male Long-Evans rats (90 days and weighing 400–540 g at the beginning of the experiment) raised at the University of Lethbridge vivarium were used
in this study. The rats were housed in pairs under a 12 h light/day cycle with lights
on at 7:30 AM. Behavioural training and testing took place during the light phase of
the cycle.
To encourage participation in the skilled reaching task, animals were placed on
a restricted feeding schedule to maintain body weight at 90–95% of baseline weight.
Animals were weighed daily. All procedures were performed in accordance with the
guidelines of the Canadian Council for Animal Care and approved by the University
of Lethbridge Animal Welfare Committee.
2.4.1. Restraint stress
Rats were placed individually in transparent Plexiglas cylinders [55,35,44]. Each
cylinder (5 cm inner diameter) had perforated ends to allow for ventilation and maintained the animals in a standing position without compression of the body. Restraint
stress was given starting at 9:00 AM. Animals were restrained for 20 min and were
tested 10 min later in the skilled reaching task [17,22,35,47] and 2.5 h later in skilled
walking. Furthermore, on the last day of baseline (pre-stress) and on experimental day 31, blood samples were collected after a 10 min post-stress interval. Thus,
2.2. Experimental design
The time course of manipulations is shown in Fig. 1. Rats were trained in the
skilled reaching task for 5 weeks. The last 5 days of reaching training were considered for baseline measurements. Rats were also trained in the skilled walking task
on day 5 of baseline. On day 6 of baseline, rats were filmed in the skilled reaching and
skilled walking tasks. On days that required skilled walking tests, a recovery period of
2 h was given between skilled reaching and skilled walking tests. The next day, blood
samples were taken for corticosterone assessments. The animals were matched
based on baseline reaching success and subdivided into three groups: Restraint &
lesion (n = 12), Variable & lesion (n = 18), and handled Lesion controls (n = 30). One animal in the Restraint & lesion group died and was excluded from the analysis, leaving
n = 11 for this group. The Restraint & lesion and Variable & lesion groups were subjected to daily restraint or variable stress, respectively, for 8 days prior to the lesion.
On day 15 of the experiment, rats were filmed in the skilled reaching and skilled walking tasks (Fig. 1). On day 16, all three groups received a focal injury of the motor cortex. Both stress regimens continued for an additional 15 days post-lesion. Rats were
filmed in the skilled reaching and skilled walking tasks on day 30 of the experiment
(day 14 post-lesion), and blood samples were collected on day 31. All behavioural
testing, blood sampling and stress treatments were performed in the morning hours.
After completion of behavioural tests, rats were perfused and the brains and adrenal
glands were removed for analysis of infarct size and adrenal gland weight. All analyses were performed by experimenters blind to the experimental condition.
2.3. Focal cerebral insult
Rats were anesthetized using isoflurane in an oxygen/nitrous oxide mixture
(isoflurane 4% for initiation, 2% for maintenance at an oxygen flow rate of 2.0 l/min). A
Fig. 2. Infarct size. (A), diagram of serial sections delineating the average infarct
size. (B), photograph of the motor cortex lesion site. (C), infarct size [mm3 ] in motor
cortex. No significant differences in infarct size were found between groups. All data
are presented as group means ± SEM.
�F.C.R. Zucchi et al. / Behavioural Brain Research 205 (2009) 67–75
Table 1
Chronic unpredictable multiple stress paradigm.
Day
Morning/afternoon
1–5 baseline
6 filming day
7 blood samples
8
9
10
11
12
13
14
15 filming day
16 stroke surgery
17
18
19
20
21
22
23
24
25
26
27
28
29
30 filming day
31 blood samples
32 perfusions
No stress/no stress
No stress/no stress
No stress/no stress
Restraint/overcrowding
Forced swimming/foot shock
Saline injection/shaking
Fox odor/social isolation
Shaking/overcrowding
Foot shock/forced swimming
Restraint/social isolation
Fox odor/forced swimming
Foot shock/social isolation
Saline injection/foot shock
Restraint/overcrowding
Fox odor/shaking
Forced swimming/overcrowding
Shaking/social isolation
Foot shock/saline injection
Shaking/fox odor
Saline injection/overcrowding
Forced swimming/shaking
Foot shock/saline injection
Restraint/forced swimming
Saline injection/social isolation
Restraint/overcrowding
Fox odor/social isolation
Restraint/fox odor
No stress
The timeline and schedule of the variable stress paradigm used in the
current study. The rats were exposed to two stressors a day (stressor 1 in
the morning hours, stressor 2 in the afternoon). Each particular stressor
occurred six times throughout the stress period.
both behavioural testing and blood sampling took place at a time when elevated
corticosterone levels after restraint stress can be expected [35].
2.4.2. Variable stress
The variable stress paradigm used a combination of psychological and physical stressors as shown in Table 1. The stressors included restraint stress [55,35,44],
swim stress [32,55,35], shaking [26,55,3], foot shock [53,58], saline injection (0.09%)
[23,44], social isolation [55], overcrowding [11], and fox odor [37,8,52]. Each day,
two different stressors were given. The first stressor occurred between 9:00 AM and
11:30 AM and the second stressor occurred between 3:00 PM and 6:00 PM. The only
exception was single housing, in which the animals were separated from their cage
mate in the afternoon, and were socially isolated overnight before being returned
to their home cages on the following morning. Rats were tested in skilled reaching
10 min after completed application of the morning stressor.
2.5. Skilled reaching training and testing
The rats were trained in the single pellet reaching task to assess skilled forelimb function [59,31] (Fig. 4A). The reaching boxes were made of clear Plexiglas
(40 cm × 45 cm × 13 cm). The front wall of the box had a 1.3 cm wide vertical slit,
allowing the rats to reach for the food pellet located on a shelf attached to the outside of the box. The shelf was located 4 cm above the floor. On the top of the shelf
were two indentations (5 mm in diameter, and 1.5 mm deep), each aligned with one
side of the slit. These indentations stabilized the pellet and were located 1.5 cm away
from the front wall [31]. In each training session, rats were placed individually in
the reaching box and a food pellet (45 mg each, BioServ, Frenchtown, NJ) was placed
contralaterally to the rats’ preferred reaching paw. To readjust their body position,
rats were trained to walk to the rear end of the box before reaching for a new pellet.
Each rat was given 20 pellets per training and test session.
A successful reach was defined as obtaining the pellet on the first attempt, withdrawing the paw through the slit and releasing the pellet to the mouth. Success was
calculated using the following formula:
Success rate =
number of successful reaches
× 100
20
The percentage of total number of pellets eaten was measured by counting the
number of pellets eaten, regardless of whether the pellet was grasped and eaten on
the first attempt. If the rat dropped the pellet, it did not count as a pellet eaten. The
percentage of total pellets eaten was measured using the following formula:
Percentage of total pellets eaten =
number of pellets eaten
× 100
20
69
To assess reaching accuracy, the number of attempts to grasp a single pellet was
averaged.
2.6. Qualitative analysis of skilled reaching
For qualitative analysis of single pellet reaching, a reaching movement was
broken down into ten components, modified from Metz and Whishaw [31]. The
following ten movement components were analyzed: (1) Limb lift: the mass of
the body weight is shifted to the hind limbs, and the hind limbs are aligned with
the body and parallel to each other. The forelimb is lifted so that the digits are
aligned with the body midline. (2) Digits close: the palm is partially supinated
and approaches the midline of the body; the digits are semi-flexed. (3) Aim: the
elbow comes in to the body with a shoulder movement while the digits retain
their position on the midline of the body. (4) Advance: the elbow is positioned
in a narrow angle to the body; the forelimb moves forward and is directed to
the target. The head and the upper body are raised and the weight is shifted to
the front. This movement is accompanied by a moderate lateral body movement
towards the reaching limb. (5) Digits open: the digits are opened by a discrete limb
movement; the palm is not fully pronated. (6) Pronation: the elbow adducts and
is pronated over the target in an arpeggio movement. (7) Grasp: the arm remains
still, while the digits close and then the paw holding the food pellet is lifted.
(8) Supination I: the elbow is adducted and the palm is supinated by approximately 90◦ . (9) Supination II: The palm is supinated to present the food pellet to
the mouth. The head drops to the level of the paws and the rat sits back on the
haunches. (10) Release: the food pellet is released into the mouth by opening the
digits.
Each of the ten components was scored on a 3-point scale. A score of 1 was given
if the movement was present. A score of 0.5 was given if the movement was present
but abnormal, and a score of 0 was given if the movement was absent. Average
scores for each component and for the total movement score (averaged values of all
10 components) were calculated based on three reaches.
2.7. Skilled walking training and testing
Fore- and hind limb coordination and limb placement were assessed using the
ladder rung walking task [33] (Fig. 6A). Rats were trained to cross a 1 m long horizontal ladder with metal rungs arranged at random distances, ranging from 1 to
5 cm. In each test session, the rung pattern was reversed to prevent the rats from
anticipating the location of the rungs. The ladder was elevated 30 cm above ground
with a neutral start box and the animals’ home cage at the end. A training session
consisted of five crossings. In each test session three trials were videotaped for further analysis. Each trial required the animal to cross the entire length of the ladder
to reach the home cage placed at the end of the apparatus.
2.8. Analysis of skilled walking
Skilled walking performance was video-recorded from a lateral perspective [33].
The camera was positioned at a slight ventral angle, so that both sides and the paw
positions could be recorded simultaneously. The video tapes were analyzed frameby-frame for quantitative and qualitative analysis. Quantitative analysis was based
on the number of errors in each crossing. Based on the limb placement scoring
system (see below), an error was defined as each limb placement that involved
missing the rung or slipping off the rung (score of 0, 1 or 2 points according to
the scale). The mean number of errors per step of each fore- and hind limb was
calculated and averaged for three trials.
The qualitative analysis of forelimb and hind limb placements was performed
using a foot fault scoring system developed earlier [33]. Limb placement was scored
by categorizing the placement of the limb on a rung and the limb protrusion between
rungs when a miss occurred by using a 7-category scale [33]. (1) Total miss: the limb
misses the rung, thus interrupting the gait pattern and causing the rat to stumble (0
points). (2) Deep slip: the limb is initially placed on the rung, but then slips off when
weight bearing and causes the limb to fall in-between rungs. (3) Slight slip: the limb
is placed on a rung, but slips off when weight bearing without causing a fall that
interrupts walking. (4) Replacement: the limb is placed on a rung, but withdrawn
before weight bearing and placed on another rung. (5) Correction: the limb aims
for one rung, but is then placed on another rung without touching the first one.
Alternatively, the limb is repositioned on the same rung. (6) Partial placement: the
limb is placed on a rung with either the wrist or digits of the forelimb or the heel and
toes of the hind limb. (7) Correct placement: the mid-portion of the palm is placed on
a rung and is weight bearing (6 points). Thus, a maximum score of six points could
be reached [33].
2.9. Video recording
All behaviour was recorded by using a Canon ZR50 MD camcorder set at a
shutter speed of 1/1000 s. During filming, additional light was supplied by a cold
light source (Lowel-light Mtg Inc., New York, USA). Frame-by-frame analysis was
performed using a Sony GV-D1000 NTSC miniDV player.
�70
F.C.R. Zucchi et al. / Behavioural Brain Research 205 (2009) 67–75
2.10. Blood samples
Blood samples were taken at baseline (day 7) and before sacrifice (day 31, 15 days
post-lesion). Rats were anesthetized using isoflurane in an oxygen/nitrous oxide
mixture (isoflurane 4% for initiation, 2% for maintenance at an oxygen flow rate
of 2.0 l/min). Blood samples were taken from the tail vein and an average of 1 ml
of blood was collected. The remainder was centrifuged at 2240 × g for 8 min. The
plasma was collected and stored at −20 ◦ C. Plasma corticosterone concentrations
were determined by radioimmunoassay using commercial kits (Coat-A-Count, Diagnostic Products Corp., Los Angeles, CA) [16]. Blood samples were collected between
the hours of 9:10–10:30 AM. No behavioural testing was performed on days on which
blood samples were taken.
2.11. Histology and measurement of infarct volume
Rats were sacrificed with an overdose of pentobarbital (Euthansol; CDMV Inc.,
Québec, Canada) and perfused through the heart with 0.9% saline and 4% formaldehyde. Brains were removed, weighed and cryoprotected in a 30% sucrose solution.
The brains were frozen and cut on a cryostat at 20 m thickness. Forty-five sections
from each brain were cut in each the anterior lesion site, the middle section and the
posterior lesion site. From each of these areas three sections were stained with cresyl violet. Photographs were captured digitally with a Zeiss microscope (Zeiss, Jena,
Germany). The cross-sectional volumes (Fig. 2A) of both hemispheres were calculated using ImageJ software (NIH, Bethesda, MD, USA). Infarct volume was measured
according to the Cavalieri method [29]. The following formulas were used:
Volume of a hemisphere = average (average area of a complete coronal hemisphere
− ventricles − area of damage)
Fig. 3. Physiological measurements. (A), adrenal gland weight [g]. (B), plasma corticosterone levels expressed as percentage of baseline values. Note that the Variable &
lesion group had significantly larger adrenal glands, while corticosterone levels were
higher in the Restraint & lesion group. All data are presented as group means ± SEM.
***p < 0.001, compared to the Lesion group.
× interval between sections × number of sections
Volume of tissue lost = tissue remaining in normal hemisphere
− tissue remaining in injured hemisphere
2.12. Adrenal gland weight
After sacrifice, adrenal glands were removed and weighed. The weights of the left
and right adrenal glands were averaged and the absolute weight of adrenal glands
was used for further analysis.
2.13. Statistical analysis
Statistical analysis was performed using Statview software version 5.0 (SAS Institute, 1998). The data were analyzed using analysis of variance (ANOVA). To avoid
possible inter-animal differences due to repeat experiments, the parametric data
were analyzed as percentage of baseline values. The Scheffe’s test was used for
between-group post hoc analysis. Within-group comparisons of quantitative data
were made via paired t-tests. The qualitative data of skilled reaching and skilled
walking were analyzed using nonparametric statistics. The Kruskal–Wallis test followed by the Mann–Whitney test was used for unpaired comparisons. The Wilcoxon
Signed Rank test was used for within-group comparisons of qualitative data. Correlation analysis of the relationship between infarct volume and skilled reaching was
performed using Fisher’s test. In all analyses a p-value of less than 0.05 was chosen as
the significance level. All data are presented as mean ± standard error of the mean.
3. Results
3.1. Infarct size
The lesion included the primary and secondary motor cortex
as well as the forelimb and hind limb areas of somatosensory
cortex (Fig. 2A and B). No significant differences between groups
in infarct size were found. The tissue lost in the damaged hemisphere was an average of 18.34 mm3 in the Lesion group, 18.02 mm3
in the Restraint & lesion group, and 22.99 mm3 in the Variable &
lesion group (Fig. 2C). There was no correlation between infarct size
and skilled reaching success on the last day of post-lesion testing
(r = 0.019).
3.2. Adrenal gland weight and plasma corticosterone levels
Data from three animals in the Lesion group and from three animals in the Variable & lesion control group were excluded from
analysis due to partial damage to one of the adrenal glands.
There were significant differences in adrenal gland weight
between groups (F(2,50) = 10.79, p < 0.001). Post hoc Scheffe analysis revealed significantly higher adrenal gland weight in Variable &
lesion animals when compared both to the Lesion group (p < 0.01)
and to the Restraint & lesion group (p < 0.01; Fig. 3A). The Restraint &
lesion group showed no difference in adrenal gland weights when
compared to the Lesion group (Fig. 3A).
Furthermore, the Restraint & lesion group had significantly
higher levels of corticosterone (CORT) compared to the Lesion group
post-lesion (CORT range: 264–847 ng/ml, in line with Thanos et
al. [51]; t(39) = 4.82, p < 0.001). There was no significant difference between the Variable & lesion and Lesion groups (CORT range:
137–661 ng/ml; Fig. 3B).
3.3. Skilled reaching
3.3.1. Reaching success
All analyses were performed as a percentage of baseline measurements. Overall, there were significant differences in success
rates between groups (F(2,56) = 2.65, p < 0.001). Post hoc Scheffe
analysis revealed significantly lower reaching success in Restraint
& lesion animals when compared to the Lesion group (p < 0.01; see
Fig. 4B).
On all pre-stroke test days and on day 29 post-stroke, Restraint
& lesion animals had lower reaching success than Lesion animals
(day 8: t(39) = −2.57, p < 0.01; day 9: t(39) = −3.38, p < 0.001; day
10: t(39) = −3.62, p < 0.001; day 11: t(39) = −3.46, p < 0.001; day
12: t(39) = −3.41, p < 0.001; day 13: t(39) = −3.63, p < 0.001; day 14:
t(39) = −3.38, p < 0.001; day 29: t(39) = −2.3, p < 0.05). There were
no significant differences between the success rates in the Restraint
& lesion and Lesion groups from day 17 to day 28. Variable & lesion
animals showed significantly lower reaching success than Lesion
animals on days 8, 9, 11 and 12 (day 8: t(46) = −2.08, p < 0.05; day
9: t(46) = −2.37, p < 0.05; day 11: t(46) = −2.58, p < 0.05; day 12:
t(46) = −2.17, p < 0.05). Success rates dropped in all three groups as
a result of the lesion.
Within-group comparisons revealed a significant decline in
the overall success rate from pre-lesion to post-lesion testing
in all groups (Lesion: t(29) = 12.16, p < 0.001; Restraint & lesion:
t(10) = 5.49, p < 0.001; Variable & lesion: t(17) = 9.78, p < 0.001).
�F.C.R. Zucchi et al. / Behavioural Brain Research 205 (2009) 67–75
71
group (day 9: t(39) = −2.66, p < 0.01; day 10: t(39) = −3.81, p < 0.001;
day 11: t(39) = −2.39, p < 0.05; day 12: t(39) = −2.62, p < 0.01; day
13: t(39) = −2.23, p < 0.05). The Variable & lesion group showed a
significantly lower value in pellets eaten on day 10 pre-lesion when
compared to the Lesion group (day 10: t(46) = −2.02, p < 0.05).
Within-group comparisons revealed a significant decrease in the
number of pellets eaten from pre-lesion to post-lesion testing in
the three groups (Lesion: t(29) = 11.26, p < 0.001; Restraint & lesion:
t(10) = 3.45, p < 0.01; Variable & lesion: t(17) = 9.43, p < 0.001).
3.3.3. Number of attempts
There were significant overall group differences in the number of
attempts needed to grasp a food pellet (F(2,56) = 2.38, p < 0.001; see
Fig. 4D). Animals from the Variable & lesion group made significantly
more attempts to grasp a pellet on days 8, 9, 11, 12 and 14 prelesion, and on days 26, 27 and 28 post-lesion, when compared to
the Lesion group (day 8: t(46) = 4.82, p < 0.001; day 9: t(46) = 3.23,
p < 0.01; day 11: t(46) = 2.79, p < 0.01; day 12: t(46) = 2.57, p < 0.01;
day 14: t(46) = 3.2, p < 0.01; day 26: t(46) = 4.21, p < 0.001; day 27:
t(46) = 2.2, p < 0.05; day 28: t(46) = 2.35, p < 0.05). Furthermore, rats
from the Restraint & lesion group made more attempts on day 8 (prelesion) and on day 18 (post-lesion) when compared to the Lesion
group (day 8 (pre-lesion): t(39) = 2.03, p < 0.05; day 18 (post-lesion):
t(39) = −2.17, p < 0.05).
Within-group comparisons revealed that the Lesion group made
significantly more attempts after the lesion when compared to prelesion performance (t(29) = −4.37, p ≤ 0.001). The Variable & lesion
group made significantly more attempts during pre-lesion testing
in comparison to post-lesion testing (t(17) = −3.2, p < 0.01).
3.4. Qualitative reaching movement analysis
Analysis of the qualitative reaching movement components
revealed significant differences between groups. There were differences in the overall movement score between groups at baseline
(H = 20.12, p ≤ 0.001) and pre-lesion stress (H = 8.72, p ≤ 0.05;
Kruskal–Wallis test). Due to group differences in baseline, the
analysis of reaching movement components was focused on withingroup comparisons (see Fig. 5).
Within-group comparisons revealed a significant drop in the
total score from pre-lesion to post-lesion in the Lesion group
(Z = −4.07, p < 0.001, Wilcoxon Signed Rank test). Comparisons
between the pre-lesion and post-lesion periods in the Lesion group
showed a significant drop in limb lift, aim, advance, digits open,
Fig. 4. Skilled reaching. (A), photograph of a rat reaching for a small food pellet in
the single pellet reaching task. (B), success rate expressed as percentage of baseline values. (C), average number of pellets eaten expressed as percentage of baseline
values. (D), average number of attempts to grasp a pellet expressed as percentage
of baseline values. Note that both restraint and variable stress reduced pre-lesion
reaching performance. Only variable stress, however, permitted post-lesion improvement in reaching success similar to control animals. All data are presented as group
means ± SEM. *p < 0.05, **p < 0.01, ***p < 0.001, compared to the Lesion group.
3.3.2. Number of pellets eaten
There were significant overall group differences in the number
of pellets eaten (F(2,56) = 2.03, p < 0.001; see Fig. 4C. The Restraint
& lesion group showed a significant decrease in pellets eaten on
days 9, 10, 11, 12 and 13 pre-lesion when compared to the Lesion
Fig. 5. Skilled reaching qualitative analysis. Rating scale of sub-components digits close, grasp, supination I, supination II, release and total reaching movement
score. Note that mainly variable stress changed the reaching movement strategy used
to grasp a food pellet both before and after lesion. $ p < 0.05, compared to baseline
values; # p < 0.05, ## p < 0.01, ### p < 0.001, compared to pre-lesion values.
�72
F.C.R. Zucchi et al. / Behavioural Brain Research 205 (2009) 67–75
pronation, grasp, supination I, supination II, and release scores (limb
lift: Z = −3.27, p < 0.01; aim: Z = −2.14, p < 0.05; advance: Z = −3.74,
p < 0.001; digits open: Z = −2.29, p < 0.05; pronation: Z = −2.32,
p < 0.05; grasp: Z = −4.23, p < 0.001; supination I: Z = −4.17, p < 0.001;
supination II: Z = −4.55, p < 0.001; release: Z = −3.77, p < 0.001).
While Lesion group scores did not change from baseline to prelesion, these scores were affected by stress treatments. Scores in
the Restraint & lesion group dropped significantly from baseline
to pre-lesion in limb lift and advance (limb lift: Z = −2.37, p < 0.05;
advance: Z = −2.47, p < 0.05). From pre-lesion to post-lesion there
was a significant drop in advance, supination I, supination II in the
Restraint & lesion group (advance: Z = −1.96, p < 0.05; supination I:
Z = −2.67, p < 0.01; supination II: Z = −2.22, p < 0.05). Variable & lesion
animals showed a drop in the total score from baseline to pre-lesion
(Z = −2.22, p < 0.05), and from pre-lesion to post-lesion (Z = −3.64,
p < 0.001). There was a significant drop in aim from the baseline to
the pre-lesion period (aim: Z = −2.34, p < 0.05). From pre-lesion to
post-lesion, Variable & lesion animals showed a drop in limb lift,
digits close, aim, advance, digits open, pronation, grasp, supination I and supination II, release, and total score (limb lift: Z = −3.46,
p < 0.001; digits close: Z = −2.59, p < 0.01; aim: Z = −2.17, p < 0.05;
advance: Z = −3.31, p < 0.001; digits open: Z = −2.76, p < 0.01; pronation: Z = −3.03, p < 0.01; grasp: Z = −3.41, p < 0.001; supination I:
Z = −3.72, p < 0.001; supination II: Z = −3.62, p < 0.001; release:
Z = −2.58, p < 0.01; total score Z = −3.63, p < 0.001).
3.5. Skilled walking
3.5.1. Number of placement errors
The ladder rung walking task revealed significant differences between groups in placement errors made with each limb
post-lesion (ipsilateral forelimb: H = 7.29, p < 0.05; contralateral
forelimb: H = 17.08, p < 0.001, ipsilateral hind limb: H = 7.7, p < 0.05;
contralateral hind limb: H = 11.94, p < 0.01; Kruskal–Wallis test;
Fig. 6B). In particular, errors increased significantly after lesion in
both, ipsilateral and contralateral forelimbs, in Restraint & lesion
animals when compared to Lesion animals (Z = −2.33, p < 0.05;
Z = −2.24, p < 0.05; respectively). By contrast, errors in the Variable &
lesion group significantly decreased post-lesion in the contralateral
forelimb and the ipsilateral and contralateral hind limbs when compared to the Lesion group (ipsilateral hind limb: Z = −2.37, p < 0.05;
contralateral hind limb: Z = −2.85, p < 0.01; contralateral forelimb:
Z = −3.17, p < 0.01).
Within-group comparisons revealed a decrease in ipsilateral
hind limb errors in the Variable & lesion group from baseline to prelesion period (Z = −2.7, p < 0.01; Wilcoxon Signed Rank test) as well
as an increase in contralateral forelimb errors from pre-lesion to
post-lesion in the Lesion (Z = −4.47, p < 0.001) and Restraint & lesion
groups (Z = −2.85, p < 0.01).
3.5.2. Foot fault scores
There were significant differences between groups in the types
of errors as expressed by the foot fault score. There were significant
differences between groups in ipsilateral and contralateral forelimb
scores post-lesion (ipsilateral forelimb: H = 6.78, p < 0.05; contralateral forelimb: H = 7.24, p < 0.05; Kruskal–Wallis test; Fig. 6C). In
the Restraint & lesion group there was a significant decrease in
ipsilateral and contralateral forelimb scores post-lesion when compared to Lesion animals [ipsilateral forelimb (post-lesion period):
Z = −3.08, p < 0.01; contralateral forelimb (post-lesion period):
Z = −2.85, p < 0.05; Mann–Whitney test].
Within-group comparisons between the pre-lesion and postlesion periods revealed a significant drop in scores in contralateral
forelimbs and hind limbs in Lesion (Z = −4.23, p < 0.001; Z = −2.77,
p < 0.01; respectively) and Restraint & lesion animals (Z = −2.93,
p < 0.01; and Z = −2.49, p < 0.05; respectively). Scores also dropped
Fig. 6. Skilled walking. (A), photograph of an animal crossing the ladder rung walking task. (B), limb placement errors and limb score (C), in the ladder rung walking
task. Note that restraint stress but not variable stress significantly exaggerated limb
placement errors as compared to lesion animals. *p < 0.05; **p < 0.01, compared to
the Lesion group.
in contralateral fore- and hind limbs in the Variable & lesion group
(Z = −2.2, p < 0.05; and Z = −1.98, p < 0.05; respectively).
4. Discussion
The current study compared the effects of chronic predictable
restraint stress with chronic unpredictable variable stress on recovery of skilled motor function in a rat model of stroke. Using a
standard lesion model in combination with a sensitive and reliable
test battery for motor performance and recovery, the observations
show that predictable restraint stress induces more pronounced
motor impairments than unpredictable variable stress in skilled
reaching and skilled walking prior to and after ischemic injury.
These findings are in controversy with the notion that unpredictable
stress might represent a more salient chronic stressor than predictable stress.
4.1. Responses to predictable restraint and unpredictable variable
stress show different physiological profiles
The present results are in accordance with previous reports
showing that exposure to chronic stress modulates motor function
in naïve rats [32,47] and exaggerates impairments after devascularization lesion [22]. In particular, Kirkland et al. [22] observed that
stress limits the development of post-lesion compensatory strategies, thus unraveling lesion-induced deficits. While these studies
used restraint to induce chronic mild stress, impaired motor function was not linked to elevated corticosterone levels. This led to
the conclusion that other components of the hypothalamic–adrenal
(HPA) axis or stress-associated emotional changes, such as anxiety,
may be the cause of stress-induced motor disturbance [35,22].
It has been widely suggested that repeated exposure to one
particular stressor, such as restraint, might gradually produce
�F.C.R. Zucchi et al. / Behavioural Brain Research 205 (2009) 67–75
habituation, and consequently diminish the physiological stress
response. The exposure to the same stressor days or even weeks
after initial exposure can alter responsiveness [14]. To minimize
habituation and to induce lasting activation of the HPA axis, previous studies have introduced paradigms using a number of mild
stressors arranged in a quasi-random sequence. The present variable stress paradigm combined several processive stressors that
led to increased adrenal gland weight within 2 weeks, as shown
earlier [26]. While adrenal hypertrophy suggests overall increased
glucocorticoid production, the absence of elevated plasma corticosterone on the particular day of blood sampling in the present study
might be confounded, such as experience of a non-salient stressor
prior to the sampling session. Repeated blood samples might have
been able to reveal overall corticosterone elevation. In turn, it is
also possible that increased adrenal gland weight was caused by
production of adrenal stress hormones other than corticosterone,
such as adrenaline and noradrenaline. In contrast to variable stress,
animals exposed to restraint stress displayed elevated plasma corticosterone levels in the absence of adrenal hypertrophy. While
restraint stress frequently fails to produce adrenal hypertrophy
[26], the presence of elevated corticosterone levels is in contrast
to previous findings from our laboratory [35,22] where corticosterone levels returned to baseline levels after 2 weeks of daily
restraint stress. This discrepancy might possibly stem from environmental influences, such as novelty. Accordingly, exposure to
chronic restraint stress can increase the locomotor response to
forced novelty, while no changes were found after variable stress
[4,27]. Furthermore, the scores of reaching movement performance
revealed group differences in baseline measures. Due to the sensitivity of these behavioural measures, it is possible that differences
in basal HPA axis activity among groups of animals, such as litters,
might account for an overall group difference. Furthermore, repeat
experiments might be influenced by slight environmental changes,
such as seasonal climate, as demonstrated before for laboratory
animals [6].
There is one cautionary note in the interpretation of the present
findings. Because the variable stress paradigm encompasses both
random appearance and multifarious nature of individual stressors,
the present study does not allow conclusions on the impact of either
temporal or inherent differences between restraint and variable
stress paradigms. Accordingly, despite the general non-specificity
of the stress response, it has been suggested that not all stressors
activate the HPA axis to the same degree. Adrenocorticotropic hormone and corticosterone release after exposure to heat stress can
be higher than overcrowding, cold stress, and food deprivation as
measured by corticosterone levels [11]. This suggests that HPA axis
activity strongly depends on the type of stressor and emphasizes
the relevance of the present results.
4.2. Distinct effects of restraint and variable stress on movement
performance
Altered skilled reaching and skilled walking performance confirmed the effectiveness of the present stress paradigms. Chronic
stress induced lasting impairments prior to the lesion, and exaggerated post-lesion motor deficits. These findings are in line with
previous observations reporting significant impairments in quantitative and qualitative measures of motor performance induced by
stress [32,22,47,17].
There were, however, a number of differences between restraint
and variable stress. Restraint stress induced a larger loss of skilled
reaching accuracy than variable stress in naïve animals. This trend
continued after lesion. By contrast, although animals exposed to
variable stress displayed a larger reduction in reaching movement scores, this stress regimen permitted compensation of these
deficits. In addition, variable stress-treated animals showed an
73
elevated number of reaching attempts both before and after
lesion, suggesting that this stressor may have caused hyperactive
behaviour. This finding indicates that motivational loss did not
account for reduced reaching success. A notable outcome was found
in the ladder rung walking task, revealing increased error rates and
altered limb placement after restraint but reduced error rates after
variable stress. These findings reproduce previous data of restraint
stress-induced disturbance of inter-limb coordination [32,35,36].
As opposed to exaggerating effects of restraint stress, variable stress
might promote successful limb placement strategies, thus diminishing post-lesion error rates. These observations are even more
remarkable with respect to testing after an extended post-stress
interval (2.5 h after restraint and variable stress induction). In summary, our findings confirm previous notions that stress not only
alters quantitative performance but also movement trajectories
[35,47].
The behavioural findings indicate stress-induced exaggeration
of deficits after ischemic lesion, which were unrelated to lesion
size. These findings are in contrast to a number of studies showing increased infarct size after 7 days of restraint [25] or social
stress [49], chronic social [10,49] or chronic variable stress [45].
These studies, however, used either middle cerebral artery occlusion (MCAO) as a model of focal ischemia or 2-vessel occlusion as
a model of global ischemia. The present study used a much smaller
focal lesion with neuronal loss limited to motor cortex and associated pathways. It is possible that the modulation of pathological
processes after ischemic lesion by elevated levels of glucocorticoids
depend on lesion size. Accordingly, previous studies using devascularization lesion showed a lack of stress-induced exaggeration of
lesion size when animals were exposed to stress prior to the lesion
[22] or to continuous stress prior to and after lesion (Kirkland and
Metz, unpublished results). These and the present findings are in
line with a report that chronic restraint for 21 days prior to MCAO
attenuates lesion volume [25]. The present data extend these observations by showing similar effects for chronic variable stress in spite
of stress-induced reduction in outcome.
4.3. Possible mechanisms of stress-induced motor alterations
The present data suggest that both chronic restraint and variable stress affect function of the intact motor system and motor
recovery after ischemic lesion, although to different degrees. While
restraint stress mainly affects movement accuracy in both reaching
and walking tasks, variable stress rather modulates performance of
movement patterns and trajectories. According to previous studies,
stressor types might have different temporal profiles depending
on their duration. As noted by Magarinos and McEwen [26], the
time courses of adaptation of restraint and variable stress differ as
reflected by their physiological profile. This led the authors to argue
that adrenal steroid secretion facilitates release of other factors,
such as excitatory amino acids, that cause stress-induced morphological changes [26]. Similarly, a study by Vyas et al. [55] found
that chronic restraint stress induces dentritic atrophy in the CA3
layer of the hippocampus, as well as hypertrophy in the basolateral
amygdala. These alterations were ameliorated in animals exposed
to chronic variable stress [55]. Similar discrete changes in neuronal
morphology might as well impact functional outcome after motor
system damage in the absence of stress-induced changes in lesion
size. Furthermore, as shown for the limbic system [26,55,56], stress
might also alter lesion-induced neuronal plasticity in denervated
as well as intact motor circuits, including the intact hemisphere
[18,19,5,12]. This is in line with previous reports of diminished
compensatory capacity after ischemic lesion in animals exposed
to restraint stress [22].
Aside from physiological considerations, the disparity of
behavioural effects induced by restraint and variable stress might
�74
F.C.R. Zucchi et al. / Behavioural Brain Research 205 (2009) 67–75
be attributed to differential effects on movement subsystems. It
was suggested that movement subsystems independently support
skilled movements, posture and locomotion [50,34]. Different types
of stress might be able to separately affect movement subsystems
of skilled function to impair certain components while releasing or
improving others. For example, variable stress might alter postural control to allow for better balance and improve limb placement
when traversing the challenging surface of the ladder rung walking
task.
Aside from the direct effects of stress on behaviour, stressinduced loss of skilled reaching capacity might be linked to
emotional changes. Chronic restraint stress represents an animal
model of anxiety [56,48,21], depression [40,48,21] and learned
helplessness [20]. These events might hinder the rat’s ability to
cope with lesion-induced motor impairments as discussed earlier [22,47]. Previous studies have indicated that anxiety-related
behaviour depends on stressor type. For example, rats exposed to
chronic restraint stress showed heightened anxiety-like behaviour
in the elevated plus maze, as opposed to rats treated with variable
stress [55,56]. Moreover, Richardson et al. [44] treated pregnant rats
with either chronic restraint stress or variable stress and compared
the behavioural alterations in the offspring. Only chronic restraint
stress resulted in offspring that exhibited increased anxiety-related
behaviours. This suggests that emotional changes generated by
restraint stress might be responsible for reduced skilled movement
accuracy in reaching and walking, as opposed to partially preserved
movement ability in variable stress-treated animals.
4.4. Conclusion
The current study demonstrated that both chronic restraint and
variable stress induce lasting impairments in skilled limb use. These
effects can be expected to persist even after cessation of stress,
particularly in males [17]. Furthermore, both stressors exaggerate
stroke outcome, although to different degrees. Impairments after
restraint stress are more pronounced than after variable stress.
Thus, the present data support the hypothesis that chronic stress
represents a major modulator of motor recovery after brain injury.
Not only stressor duration, but also the type of stress might play a
critical role in determining stroke outcome.
Acknowledgements
The authors are grateful to Keri L. Colwell, Noora Badr and Norah
F. Matthies for support with the experiments. This research was
supported by the Canadian Institutes of Health Research (GM), the
Canadian Stroke Network (GM), and the Alberta Heritage Foundation for Medical Research (LvW, AK, GM).
References
[3] Alfarez DN, Joels M, Krugers HJ. Chronic unpredictable stress impairs longterm potentiation in rat hippocampal CA1 area and dentate gyrus in vitro. Eur
J Neurosci 2003;17:1928–34.
[4] Araujo APN, DeLucia R, Scavone C, Planeta CS. Repeated predictable or
unpredictable stress: effects on cocaine-induced locomotion and cyclic AMPdependent protein kinase activity. Behav Brain Res 2003;139:75–81.
[5] Biernaskie J, Corbett D. Enriched rehabilitative training promotes improved
forelimb motor function and enhanced dendritic growth after focal ischemic
injury. J Neurosci 2001;21:5272–80.
[6] Catanach BM, Patrick G, Papworth D, Goodhead DT, Hacker T, Cobb L, et al.
Investigation of lung tumour induction in BALB/cJ mice following paternal Xirradiation. Int J Radiat Biol 1995;67:607–15.
[7] Christensen H, Boysen G, Johannesen HH. Serum-cortisol reflects severity and
mortality in acute stroke. J Neurol Sci 2004;217:175–80.
[8] Day HEW, Masini CV, Campeau S. The pattern of brain c-fos mRNA induced
by a component of fox odor, 2,5-dihydro-2,4,5-trimethylthiazoline (TMT), in
rats, suggests both systemic and processive stress characteristics. Brain Res
2004;1025:139–51.
[9] Desrosiers J, Malouin F, Richards C, Bourbonnais D, Rochette A, Bravo G. Comparison of changes in upper and lower extremity impairments and disabilities
after stroke. Int J Rehabil Res 2003;26:109–16.
[10] DeVries AC, Joh HD, Bernard O, Hattori K, Hurn PD, Traystman RJ, et al. Social
stress exacerbates stroke outcome by suppressing Bcl-2 expression. PNAS USA
2001;98:11824–8.
[11] Djordjevic J, Cvijic G, Davidovic V. Different activation of ACTH and corticosterone release in response to various stressors in rats. Physiol Res
2003;52:67–72.
[12] Dijkhuizen RM, Singhal AB, Mandeville JB, Wu O, Halpern EF, Finklestein SP,
et al. Correlation between brain reorganization, ischemic damage, and neurologic status after transient focal cerebral ischemia in rats: a functional magnetic
resonance imaging study. J Neurosci 2003;23:510–7.
[13] Grissom N, Kerr W, Bhatnagar S. Struggling behavior during restraint is regulated by stress experience. Behav Brain Res 2008;191:219–26.
[14] Harbuz M. Neuroendocrine function and chronic inflammatory stress. Exp
Physiol 2002;87:519–25.
[15] Hazard D, Leclaire S, Couty M, Guémené D. Genetic differences in coping strategies in response to prolonged and repeated restraint in Japanese
quail divergently selected for long or short tonic immobility. Horm Behav
2008;54:645–53.
[16] Ishida H, Mitsui K, Nukaya H, Matsumoto K, Tsuji K. Study of active substances
involved in skin dysfunction induced by crowding stress. I. Effect of crowding
and isolation on some physiological variables, skin function and skin blood
perfusion in hairless mice. Biol Pharm Bull 2003;26:170–81.
[17] Jadavji NM, Metz GA. Sex differences in skilled movement in response to
restraint stress and recovery from stress. Behav Brain Res 2008;195:251–9.
[18] Jones TA, Schallert T. Overgrowth and pruning of dendrites in adult rats recovering from neocortical damage. Brain Res 1992;581:156–60.
[19] Jones TA, Chu CJ, Grande LA, Gregory AD. Motor skills training enhances lesioninduced structural plasticity in the motor cortex of adult rats. J Neurosci
1999;19:10153–63.
[20] Kademian SME, Bignante AE, Lardone P, McEwen BS, Volosin M. Biphasic effects
of adrenal steroids on learned helplessness behavior induced by inescapable
shock. Neuropsychopharmacology 2005;30:58–66.
[21] Kim KS, Han PL. Optimization of chronic stress paradigms using anxiety- and
depression-like behavioural parameters. J Neurosci Res 2006;83:497–507.
[22] Kirkland SW, Coma AK, Colwell KL, Metz GA. Delayed recovery and exaggerated
infarct size by the post-lesion stress in a rat model of focal cerebral stroke. Brain
Res 2008;1201:151–60.
[23] Kiyatkin EA, Wise RA. Striatal hyperthermia associated with arousal: intracranial thermorecordings in behaving rats. Brain Res 2001;918:141–52.
[24] Lupien SJ, McEwen BS. The acute effects of corticosteroids on cognition: integration of animal and human model studies. Brain Res Rev 1997;24:1–27.
[25] Madrigal JLM, Caso JR, de Cristobal J, Cardenas A, Leza JC, Lizasoain I, et al. Effect
of subacute and chronic immobilization stress on the outcome of permanent
focal cerebral ischemia in rats. Brain Res 2003;979:137–45.
[26] Magarinos AM, McEwen BS. Stress-induced atrophy of apical dendrites of hippocampal CA3c neurons: comparison of stressors. Neuroscience 1995;69:83–8.
[27] Marin MT, Cruz FC, Planeta CS. Chronic restraint or variable stresses differently
affect the behavior, corticosterone secretion and body weight in rats. Physiol
Behav 2007;90:29–35.
[28] Masini CV, Day HEW, Campeau S. Long-term habituation to repeated loud noise
is impaired by relatively short interstressor intervals in rats. Behav Neurosci
2008;122:210–23.
[29] Mayhew TM, Olsen DR. Magnetic resonance imaging (MRI) and model-free
estimates of brain volume determined using the Cavalieri principle. J Anat
1991;178:133–44.
[30] McEwen BS, Sapolsky RM. Stress and cognitive function. Curr Opin Neurobiol
1995;5:205–16.
[31] Metz GA, Whishaw IQ. Skilled reaching an action pattern: stability in rat (Rattus novergicus) grasping movements as a function of changing food pellet size.
Behav Brain Res 2000;116:111–22.
[32] Metz GA, Schwab ME, Welzl H. The effects of acute and chronic stress on
motor and sensory performance in male Lewis rats. Physiol Behav 2001;72:
29–35.
[33] Metz GA, Whishaw IQ. Cortical and subcortical lesions impair skilled walking in the ladder rung walking test: a new task to evaluate fore-and hind
limb stepping, placing, and co-ordination. J Neurosci Methods 2002;115:
169–79.
[34] Metz GA, Gonzalez CL, Piecharka DM, Whishaw IQ. Acute alcohol administration
improves skilled reaching success in intact but not 6-OHDA dopamine depleted
rats: a subsystems analysis of the motoric and anxiolytic effects of alcohol.
Behav Brain Res 2003;142:167–74.
[35] Metz GA, Jadavji NM, Smith LK. Modulation of motor function by stress: a novel
concept of the effects of stress and corticosterone on behavior. Eur J Neurosci
2005;22:1190–200.
[36] Metz GA. Stress as a modulator of motor system function and pathology. Rev
Neurosci 2007;18:209–22.
[37] Morrow BA, Redmond AJ, Roth RH, Elsworth JD. The predator odor, TMT, displays
a unique, stress-like pattern of dopaminergic and endocrinological activation
in the rat. Brain Res 2000;864:146–51.
[38] Mosenthal AC, Livingston DH, Lavery RF, Knudson MM, Lee S, Morabito
D, et al. The effect of age on functional outcome in mild traumatic brain
injury: 6-month report of a prospective multicenter trial. J Trauma 2004;56:
1042–8.
�F.C.R. Zucchi et al. / Behavioural Brain Research 205 (2009) 67–75
[39] Murros K, Fogelholm R, Kettunen S, Vuorela AL. Serum cortisol and outcome of
ischemic brain infarction. J Neurol Sci 1993;116:12–7.
[40] Muscat R, Rapp M, Wilner P. Reversal of stress-induced anhedonia by the atypical antidepressants, fluoxetine and maprotiline. Psychopharmacology (Berl)
1992;109:433–8.
[41] Olsson T. Urinary free cortisol excretion shortly after ischaemic stroke. J Intern
Med 1990;228:177–81.
[42] Parker CC, Ponicsan H, Spencer RL, Holmes A, Johnson TE. Restraint stress
and exogenous corticosterone differentially alter sensitivity to the sedativehypnotic effects of ethanol in inbred long-sleep and inbred short-sleep mice.
Alcohol 2008;42:477–85.
[43] Pijlman FTA, Wolterink D, van Ree JM. Physical and emotional stress have differential effects on preference for saccharine and open field behaviour in rats.
Behav Brain Res 2003;139:131–8.
[44] Richardson HN, Zorrilla EP, Mandyam CD, Rivier CL. Exposure to repetitive versus varied stress during prenatal development generates two
distinct anxiogenic and neuroendocrine profiles in adulthood. Endocrinology
2006;147:2506–17.
[45] Ritchie LJ, De Butte M, Pappas BA. Chronic mild stress exacerbates the effects
of permanent bilateral common carotid artery occlusion on CA1 neurons. Brain
Res 2004;1014:228–35.
[46] Shepherd RB. Exercise and training to optimize functional motor performance
in stroke: driving neural reorganization? Neural Plast 2001;8:121–9.
[47] Smith LK, Jadavji NM, Colwell KL, Perehudoff KS, Metz GA. Stress accelerates
neural degeneration and exaggerates motor symptoms in a rat model of Parkinson’s disease. Eur J Neurosci 2008;27:2133–46.
[48] Strekalova T, Spanagel R, Dolgov O, Bartsch D. Stress-induced hyperlocomotion as a confounding factor in anxiety and depression models in mice. Behav
Pharmacol 2005;16:171–80.
[49] Sugo N, Hurn PD, Morahan B, Hattori K, Traystman RJ, DeVries AC. Social stress
exacerbates focal cerebral ischemia in mice. Stroke 2002;33:1660–4.
[50] Teitelbaum P, Schallert T, Whishaw IQ. Sources of spontaneity in motivated behavior. In: Satinoff E, Teitelbaum P, editors. Handbook of behavioral
[51]
[52]
[53]
[54]
[55]
[56]
[57]
[58]
[59]
[60]
75
neurobiology. New York: Plenum Publishing Corporation; 1983. Vol. 6,
pp. 23–65.
Thanos PK, Cavigelli SA, Michaelides M, Olvet DM, Patel U, Diep MN, et al. A
non-invasive method for detecting the metabolic stress response in rodents:
characterization and disruption of the circadian corticosterone rhythm. Physiol
Res 2009;58:219–28.
Thomas RM, Urban JH, Peterson DA. Acute exposure to predator odor elicits a robust increase in corticosterone and a decrease in activity without
altering proliferation in the adult rat hippocampus. Exp Neurol 2006;201:
308–15.
Trentani A, Kuipers SD, te Meerman GJ, Beekman J, ter Horst GJ, den Boer JA.
Immunohistochemical changes induced by repeated footshock stress: revelations of gender-based differences. Neurobiol Dis 2003;14:602–18.
Uchida S, Nishida A, Hara K, Kamemoto T, Suetsugi M, Fujimoto M, et al.
Characterization of the vulnerability to repeated stress in Fisher 344 rats: possible involvement of microRNA-mediated down-regulation of the glucocorticoid
receptor. Eur J Neurosci 2008;27:2250–61.
Vyas A, Mitra R, Shankaranarayana Rao BS, Chattarji S. Chronic stress induces
contrasting patterns of dendritic remodeling in hippocampal and amygdaloid
neurons. J Neurosci 2002;22:6610–8.
Vyas A, Chattarji S. Modulation of different states of anxiet-like behaviour by
chronic stress. Behav Neurosci 2004;118:1450–4.
Wade DT. Measuring arm impairment and disability after stroke. Int Disabil
Stud 1989;11:89–92.
Westenbroek C, Snijders TAB, den Boer JA, Gerrits M, Fokkema DS, Ter Horst GJ.
Pair-housing of male and female rats during chronic stress exposure results in
gender-specific behavioural responses. Horm Behav 2005;47:620–8.
Whishaw IQ, Pellis SM, Gorny B, Kolb B, Tetzlaff W. Proximal and distal impairments in rat forelimb use in follow unilateral pyramidal tract lesions. Behav
Brain Res 1993;56:59–76.
Whishaw IQ. Loss of the innate cortical engram for action patterns used in
skilled reaching and the development of behavioral compensation following
motor cortex lesions in the rat. Neuropharmacology 2000;39:788–805.
�
 Gerlinde Metz
Gerlinde Metz Fabiola Zucchi
Fabiola Zucchi