CHAPTER 11
BIOTERRORISM AND BIODEFENSE
FOR AMERICA’S PUBLIC SPACES
AND CITIES
Brian Hanley and Birthe Borup
The Black Death swept through Europe from 1347 to 1350, killing 60 per1
cent of the entire population, around 50 million people, and changing history (see Figure 11.1). “During the 14th century the black death struck
2
Florence and wiped out three of every four people in the city.” This was
the backdrop for Giovanni Boccaccio’s writing The Decameron:
The plight of the lower and most of the middle classes was even more pitiful
to behold. … Since they received no care and attention, almost all of them
died. Many ended their lives in the streets both at night and during the day;
and many others who died in their houses were only known to be dead
because the neighbors smelled their decaying bodies. Dead bodies filled
every corner. Most of them were treated in the same manner by the survivors,
who were more concerned to get rid of their rotting bodies than moved by
charity towards the dead … Such was the multitude of corpses brought to
the churches every day and almost every hour that there was not enough
consecrated ground to give them burial … Although the cemeteries were full
they were forced to dig huge trenches, where they buried the bodies by hundreds. Here they stowed them away like bales in the hold of a ship and cov3
ered them with a little earth, until the whole trench was full.
Other accounts of this period are equally dramatic. For example, Johanes
Nohl wrote,
From all countries it is reported that gravediggers threw infected matter from
their carts so as to stimulate the epidemic which for them was a time of
luxury … The worst of all is that the rich, higher town officials and all persons vested with official authority flee among the first at the outset of the
�Bioterrorism and Biodefense for America’s Public Spaces and Cities
Figure 11.1
255
Estimated Population of Europe during the Black Death
plague, so that administration of justice is rendered impossible and no one
can obtain his rights. General anarchy and confusion set in and that is the
4
worst evil by which the commonwealth can be assailed.
And according to Fray Toribio Motolinia,
They died in heaps, like bedbugs. … as it was impossible to bury the great
number of dead, they pulled down the houses over them so that their homes
become their tombs. … Many others died of starvation because they were all
taken sick at once, they could not care for each other, nor was there anyone to
5
give them bread or anything else.
Smallpox and other European diseases sweep through the Indian nations
in Mexico in the 1500s, killing on the order of 50 percent to 90 percent of
all native inhabitants. Earliest records from colonists in New England
record fatality rates of 90 percent to 95 percent among American Indians
exposed to European diseases such as smallpox and influenza (see Fig6
ure 11.2).
Such is the power of natural diseases, able to cripple nations or remove
them completely from our world. Imagine a similar epidemic sweeping
through the United States today, spreading from person to person, and
killing indiscriminately, perhaps even aided by people who see it as giving them advantage and a better life than they had. And now imagine that
this disease did not come from nature, but that it was introduced willfully
by man, maybe even created by him. Such is the power of biological warfare: a power so great as to render nations and cultures powerless, or to
nearly erase them from our earth. This has been demonstrated on or near
United States soil, from American Indians of the sixteenth through the
7
eighteenth centuries, to Pacific Islanders of the twentieth century. Methods and techniques for biological warfare have become so readily available, so well understood and inexpensive worldwide, that it is simply a
matter of time before they will be applied effectively by states and
�Figure 11.2
Major Disease Pool Competition and Biological Warfare Time Line
�Bioterrorism and Biodefense for America’s Public Spaces and Cities
257
nonstate actors. As the price tag for biological weapons development and
deployment drops, even small terrorist groups can easily acquire the
means for a biological attack. A survey conducted in May 2005 by one of
the authors of this chapter indicated that less than $10,000 would be
needed to assemble a laboratory with highly sophisticated capabilities.
Since biological weapons are capable of such high death rates, they can
seriously damage or even bring down entire nations. Natural disease
pools, prior to the development of modern medicine, were a primary
8
determinant of the outcome of long-term conflicts. Those disease pools
9
have been deliberately used in warfare as well. It is worth noting that,
from an evolutionary point of view, a population that is resistant to, yet
supports the propagation of deadly diseases wins out against a newly
contacted population that is not resistant. Thus, there is a benefit to being
susceptible enough to support propagation of a disease, but resistant
enough in the population as a whole that the population can survive as
a group. Such disease pools have been basic to guiding the long-term out10
come of military conquests and conflicts prior to modern medicine.
Most public health scenarios consider casualty rates of 2 percent to
3 percent of the total population to be catastrophic. The scenarios considered in this chapter include but also far exceed that. In the modern era, the
effect of high casualty rates from disease can be seen on the less developed countries of Africa from the HIV plague. Infection rates in subSaharan Africa are over 7 percent, with 2.3 million deaths per year, and
11
over half of the total population with AIDS worldwide. This has led to
legions of orphans who have provided cannon fodder for wars in the
region and other ill effects. UNICEF has estimated that by 2010 there will
be as many as 18 million children in sub-Saharan Africa orphaned by
12
AIDS. Thus, it should be understood that the effects of disease can be
highly destructive for societies in various ways.
DEATHS FROM WAR VERSUS DISEASE
Compared to war, diseases have killed far more people. For example, in
13
the United States alone, 36,000 people per year die from influenza, and
14
18,000 people per year are now dying from HIV/AIDS. (This rate has risen, fallen, and risen again.) In general, infectious disease rates in the
United States dropped during the twentieth century; however, rates have
varied, from 797 deaths per every 100,000 people in 1900 to 36 deaths per
100,000 in 1980, with a dramatic peak in 1918 due to the influenza pan15
demic. From 1981 to 1995, the mortality rate increased to a peak of
63 deaths per 100,000 in 1995 and declined to 59 deaths per 100,000 in
16
1996. Today, that number of roughly 60 deaths per 100,000 people translates to approximately 180,000 Americans dying each year of infectious
disease under normal conditions.
�258
Public Spaces and Social Institutions
Overall, in the last 100 years, approximately 10–18 million people have
17
died from infectious diseases alone in the United States Compare that
with the number of Americans who have died due to wars over the last
century:
• World War I—118,000 dead
• World War II—300,000 dead
• Korean War—34,000 dead
• Vietnam War—59,000 dead
• Iraq War—2,000 dead
• Total—less than 520,000
In other words, all twentieth century wars combined have killed approximately 5 percent of the number of Americans who have died of disease
during the same time period. Using the Centers for Disease Control and
Prevention (CDC) estimates for influenza deaths, at least 1 million and
probably more than 1.5 million Americans died from influenza alone
during the second half of the twentieth century. For the United States,
influenza alone killed three times the number of people in just 50 years
of low-level mortality (nonpandemic) than died from all wars combined
during the whole century.
Worldwide, estimates vary for the number killed in war. Zbigniew
Brzezinski cataloged between 167 and 175 million “lives deliberately
18
extinguished by politically motivated carnage.” However, looking at just
three diseases in the twentieth century, that number is probably eclipsed.
It is not possible to cite precise statistics for malaria, influenza, and HIV
for the entire twentieth century, since even today deaths are estimated.
But according to the CDC, malaria deaths today currently account for
19
700,000–2.7 million deaths each year, though other estimates are a bit
20
higher. In any case, it is reasonable to estimate that approximately
120 million people worldwide died of malaria in the twentieth century.
There was only a short hiatus in the years immediately following World
War II when malaria mortality dropped to low levels because of the application of DDT (dichloro-diphenyl-trichloroethane). For HIV/AIDS, an
21
estimated 11.7 million deaths had occurred by 1997. From influenza, just
22
the 1918 pandemic killed 50 million people around the world. This brief
review gives us a number of around 180 million people dead from
malaria, HIV, and the 1918 influenza pandemic alone.
However, outside of the extraordinary pandemic in 1918, the worldwide yearly normal death toll from influenza is unlikely to be below
500,000 per year, and quite possibly is over 1 million per year; in the
United States alone, 36,000 people die each year. The United States contains roughly 5 percent of the total population of the world, so if that
�Bioterrorism and Biodefense for America’s Public Spaces and Cities
259
death rate holds true for the world as a whole, then one would expect
700,000 people worldwide to die of influenza. Since the United Stataes
has better health care than developing nations of the world, the true number is most likely higher. Thus, the flu has killed a lot of people over the
course of a century, most likely producing another 30–80 million fatalities.
If this figure is added to the previous observations, between 220 million
and 250 million people have died from these three major diseases alone.
It is for this reason that many physicians say, “Nature is the greatest
terrorist.”
Approximately 2,750 died in the New York World Trade Center attack,
23
with exact numbers unlikely to ever be known precisely. In Spain, 202
24
died in Madrid’s train bombing, and approximately 50 in London for a
rough total of around 3,000—less than 10 percent of the 36,000 people
25
who die each year from influenza in the United States alone.
This is why there should be concern about bioterrorism. Diseases that
nature has provided, combined with the ingenuity of men, could easily
exceed deaths from all other causes in just one serious incident. All other
terrorist attacks from bombs and planes will pale in comparison. In
addition, in the modern world, man is capable of doing more than what
26
nature is likely to do with bioterrorism. Thus, it is a frightening reality
that extremist groups like al Qaeda are actively seeking bioterrorism
capabilities.
FUNDAMENTAL PRINCIPLES
There are seven fundamental principles of biological warfare: (1) Any
virus whose DNA sequence is known can no longer be considered eradicated. (2) New organisms not found in nature can be engineered. (3) The
focus of biological warfare is populations, not individuals. (4) To be maximally successful, the attack must go unnoticed until the population’s
health system is overwhelmed by cases of infection. (5) The attacker needs
to have a motive and the means to carry out the attack. (6) The attack must
be carefully prepared. (7) Murphy’s Law, that anything that can go wrong
will go wrong, applies to attackers during the preparation and the attack.
The most fundamental principle of biological warfare today is that any
virus whose DNA sequence is known can no longer be considered eradicated. Since the DNA sequences of dangerous viruses are published, and
nucleotide synthesis is capable of reproducing them at will with an ease
growing by leaps and bounds, it is, while not yet trivial, a reasonably
straightforward matter to assemble the required equipment and cell cultures to produce small seed culture amounts of almost any virus. For as
long as our world maintains the technological capability for synthesis of
nucleotide chains of sufficient length, this will remain true. Consequently,
attack by any known sequenced organism must be considered plausible.
�260
Public Spaces and Social Institutions
In the modern world, the attacker would not need to acquire the virus,
such as smallpox, from cold storage, but could synthesize it.
The second principle is that for every known disease, there is some
unknown number of organisms that could be engineered that could be
more deadly than the wild type. Given the demands of evolution on
microorganisms to spare their own host population or face extinction
themselves, it is a near certainty that any organism that is able to kill more
than 30 percent of a total population in today’s medical milieu (note that
this is not 30 percent of those infected) will be an engineered organism,
most likely with human logistical help to infect the population. (Note
the difference between sparing any specific host or person and sparing
enough of the host population to allow the disease parasite to survive.)
Our knowledge of the mammalian cell and of the human immune system
has become very sophisticated. Engineering a deadly disease organism,
while definitely not trivial, is a much more tractable problem than it once
was, and it is becoming more so at a rate that is disquieting.
For instance, advances in genetic engineering in the past ten years have
made it possible to create enzymes with novel activities. These enzymes
27
can either synthesize chemicals generally not found in nature, synthesize
28
29
known chemicals with greater efficiency, or degrade chemicals. Using
these techniques it is possible to create new organisms (virus or bacteria)
that can be used in biological warfare. These organisms could produce
toxins (potentially in high quantities) that our immune systems are unable
to cope with, killing us outright, or weakening us so that we become susceptible to other diseases. The genetically modified organism could also
be made resistant to antibiotics or other medication by having enzymes
that degrade the antibiotics. This could create supergerms that modern
medicine would be unable to kill effectively. However, this is not the limit
of what modern molecular biology makes possible.
The third principle is that in biological warfare, individuals are not the
focus, populations are. While there are methods and techniques for delivering or making organisms for the purpose of specific assassination of
individuals, and these could be a small, maybe crucial, part of a larger
warfare scenario, they are not in themselves going to win a war anymore
than snipers will in conventional warfare. What matters is the degree of
penetration of a population by an agent, and the amount and type of
desired casualties produced in the population by the agent.
Fourth, to be successful, a biological attack must either overwhelm the
capacity of the target population to respond to the attack or evade the ability of the target population to diagnose that an attack has taken place until
it is too late. A corollary to this is that the difficulty of either overwhelming a health care system or evading detection of the agent probably rises
with the percentage of the population the attacker desires to eliminate.
However, this latter should not be cause for overconfidence.
�Bioterrorism and Biodefense for America’s Public Spaces and Cities
261
Fifth, as in any serious crime, an attacker must have both motive and
capacity to carry out the attack. Accidental development, production,
and deployment are exceedingly unlikely. While stating that motive and
capacity are necessary may seem to be a tautology, it leads us to carefully
examine who has the means and who has the motive. In today’s world it
no longer requires the resources of nation-states to conduct serious biological warfare as it did in the relatively recent past. Nation-states certainly can do so, but the means to develop and produce them has such a
low cost, that small non-state actors can afford it. Nation-states face the
problem that, if they use them, they will suffer heavy conventional retaliation. Individuals and transnational terrorists do not have this problem of
retaliation, since, if nation-states could retaliate effectively, they would
already have done so and terrorism would not be a problem in the first
place. Consequently, when examining motive, we must look beyond the
classical motives of national militaries and examine both the record of
attacks and attempted attacks that have occurred and the pattern of action
of small groups and private individuals for violent activism.
The sixth principle is that in order to conduct an attack, several things
are necessary. The organism must be acquired or developed. The organism must be cultured or reproduced by some means, and finally, the
organism must be deployed according to an effective plan of attack. Interdiction is possible at any point in the process, as are errors or mistakes by
potential attackers. Dangerous viruses have significant handling problems, which may be, for an attacker, one of the most difficult issues to deal
with, though this should also not be cause for overconfidence.
In addition, to accomplish a successful attack, the attackers will need
two more things. They will need to test their organism’s effectiveness,
and they will need to create a plan for effective deployment. Intuition
and luck can produce quite a number of casualties, but only a well-developed plan will ensure a successful high-level attack (high mortality rate of
target population), unless the attacker gets lucky. In general, the higher
the level of attack to be carried out, the greater the degree of testing and
planning required to be successful.
The last principle of biological warfare is that Murphy’s Law (that anything that can go wrong will go wrong) applies to attackers without a
30
doubt. Every actual deployment has had serious problems. The Japanese
in World War II dropped plague-bearing fleas on China from airplanes. It
is unclear that any illness resulted from this. In 1991, Shoko Asahara’s
group in Japan sprayed anthrax from a building in Tokyo with no result
because the variety used was a nontoxic lab strain. Asahara sent followers
to Africa to collect a sample of the Ebola virus during an epidemic, which
they failed to obtain. In 1984, Ananda Sheela of the Rajneesh group in Oregon directed the spraying of Salmonella typhimurium on a salad bar and
succeeded in making people ill. However, her alleged attempts to
�262
Public Spaces and Social Institutions
assassinate a district attorney failed. Any individual or group who
decides to launch an attack has a high probability of making a serious
mistake, which is all to the good.
POSSIBLE ATTACKERS
In the United States biological weapons are generally thought unreliable for militaries because of the problem of blowback—i.e., that the
attackers themselves could get sick. This is, however, a debatable classification since no such blowback has occurred in practice in the twentieth
century, even when biological weapons have been deployed, though biological warfare, per se, has never occurred on an unrestricted scale in the
twentieth century.
Other nations and their leaders are also unlikely users of biological
weapons. In the modern world with its nuclear weapons and highly
developed conventional military capabilities, the problem for a nation
considering the use of biological weapons is the problem of retaliation.
A nation-state discovered to be conducting serious biological warfare
against a nuclear power, or even knowingly harboring those who are, is
quite probably committing suicide. The degree of threat to the world as
a whole from such a nation would result in very serious consequences
based on consensus among leading nations. But this balance of power is
specific to nations and their leaders. For the purpose of this calculation,
national leaders are quite rational and, therefore, unlikely to use biologi31
cal warfare overtly. However, using intercontinental ballistic missiles
(ICBMs) carrying biological weapons after attacking another nation with
nuclear weapons was an integral part of warfare doctrine of the Soviet
32
Union.
Since any organism can be obtained, and new attack organisms can be
engineered with budgets potentially accessible to individuals, this means
that we can no longer exclusively focus on the motives of nation-states
and their leaders. In fact, the most likely initiators of a serious biological
warfare attack are small religious groups, activist groups, and “armies of
one” (for example, Theodore John Kaczynski, Ph.D., aka the Unabomber).
The basics here are leadership and doctrine.
Since the close of World War II, all biological attacks of known origin
have been carried out by religious organizations run by a charismatic
leader. Of the known attacks, one occurred in Oregon at the command of
Ananda Sheela, an aide to Bhagwan Rajneesh. It is possible that this attack
was carried out without Rajneesh’s knowledge, as he was the one who
blew the whistle on it. The other attack was carried out at the command
of Asahara in Japan. His group sprayed a raw extract of anthrax culture
from a rooftop in Tokyo, which accomplished nothing except the creation
of an exceedingly bad smell that attracted the attention of the citizenry
�Bioterrorism and Biodefense for America’s Public Spaces and Cities
263
and police. The 2001 U.S. letter attack using anthrax powder is the only
known biological attack that actually caused deaths. Since it is possible
(though not certain) that al Qaeda carried out this attack, the attack may
eventually be classified as an attack by a religious group. None of these
attempts was meant to kill a large fraction of a population. There has also
been a possible attempt to acquire Yersinia pestis and anthrax for weapons
use by an Aryan Nations member, microbiologist Larry Harris in 1995
33
and 1998.
A biological attack will not occur without a leader who gives the orders
or approves of the plan. It is possible for an attack to occur without doctrine supporting it; however, this is more difficult. There will generally
be a chain of reasoning justifying an act of such magnitude. In the case
of Rajneesh’s lieutenant, Ananda Sheela, her motive was political power
to advance her guru’s interests, in the context of evidence that she may
have embezzled millions from Rajneesh. In the case of Asahara, the
motive was the glory of Aum Shinrikyo that Asahara might rule on earth.
This latter is a common enough motive in history.
The “army of one” (e.g., the Unabomber) also conforms to these basics,
just rolled into one body. Ted Kaczynski was his own philosopher king,
and he conducted his campaign within the framework of a doctrine that
he had made for himself. That doctrine excuses his acts as the Unabomber,
sending exploding packages through the mail to people he considered
key technology boosters, killing three of them and maiming others, as a
necessary evil. The sort of individual who would conduct a biological
attack is probably going to fit the profile of a mass murderer, the type that
distances himself or herself from their victims.
THE MOTIVE AND ORGANIZATION OF THE ATTACKER
Its global reach and its ability to inflict damage should not be underestimated, This enemy seeks to acquire weapons of mass destruction and will
certainly use such weapons if they obtain them … They experimented with
anthrax in Afghanistan. They tried to develop crude chemical weapons in
Afghanistan. … This is not my guess, this is what they say. It’s well known
34
they want to do this, and they’ll stop at nothing.
—General John Abizaid
In the modern world the primary biological weapons threat is probably
small to midsize terrorist groups and individuals, perhaps in clandestine
league with rogue states. This section of the chapter examines several
basic rationales that can serve as the basis for a biological attack and discusses their organization.
A political terrorist group such as al Qaeda may have a doctrine of war
against a nation or nations and carry out various terrorist acts of
�264
Public Spaces and Social Institutions
war. Al Qaeda declared war on the United States several times, but
was ignored until 9/11. This type of network is probably going to be
35
organized in a “small world” manner, as al Qaeda is. Such networks
are primarily social in their recruitment and motivation, not an outgrowth
36
of poverty, trauma, and ignorance. Poverty and ignorance have long
been understood to be correlated with revolution and conventional war;
however, they do not appear to be primary drivers for terrorists of
al Qaeda and its affiliated groups, which is a significant shift in thinking.
A religious group can have the doctrine that it must dominate all others
and rule the world. The doctrine usually demands this rule because it is
for the good of all, it is what its “god” wants, and therefore extraordinary
means are reasonable. Rajneesh is reported to have talked of the desirability of establishing a spiritual dictatorship, though this is not central to his
37
writings and is not part of the Hindu roots from which he came. Asahara
38
believed that he was the “divine emperor” of the world, though similarly, this was definitely not part of the Buddhist culture he claimed to
be representing. In the continuum of such groups, there are outliers on
the religious fringe that have engaged in dangerous terrorist attacks.
There is every reason to believe that such attacks may happen again from
the same type of source and possibly be extremely effective. Doctrines of
world domination are known among atheistic utopian movements, and
we have seen mass death resulting from this type of doctrine in the reign
of Pol Pot in Cambodia and Joseph Stalin in the USSR. If a group is short
of its goal of domination, a biological weapon that can reach the goal
may be used.
An ecological rationale for deploying a biological weapon is rationally
justifiable. Believing there are too many people in the world, such a
rationale proposes to kill a large fraction, or all people to save the planet.
A private individual could decide to do this, as could an ecoactivist fringe
group.
METHODS OF SELF-PROTECTION FOR ATTACKERS
There are three primary methods by which attackers could protect
themselves from being infected and even killed by their own biological
weapons. The first method is sterile technique and hygiene, coupled with
a knowledge of the precise nature of their virus. Some types of viruses can
be handled only this way.
The second method is to culture a nontoxic form of the same virus and
deliberately make sure that everyone involved with conducting the attack
has been infected with it. In this way, the developers could provide themselves with a “live vaccine” against the virus (albeit one not meeting FDA
standards), although it may even kill some of them. Such odd events
could potentially be investigated as possible indicators of a clandestine
�Bioterrorism and Biodefense for America’s Public Spaces and Cities
265
bioterror plot. Or, the developers could simply culture and kill the virus
and inject it into themselves. This killed vaccine technique was used by
the Soviet Union’s bioweapons program with success. Most of the time,
this would be effective enough for those already willing to take huge
risks.
Lastly, the developers could collect drugs for treatment and run a few
human prisoner trials or trials on volunteers from inside their organization to see if the drugs work before releasing the virus. It is probable that
antiviral drugs would be unreliable protection; however, if nothing else
is available, an attacker could resort to such a protection as it could at least
raise the survival rate of the attackers to a significant degree.
In most cases, it is highly probable that attackers would want to have
some protection from their creation. Thus, one goal of intelligence gatherers working on biological terrorism should be to determine what method
of self-protection any attackers are using. Of course, none of these selfprotection methods have any meaning to the suicide terrorist, like those
who have conducted many of the Islamic extremist attacks in the past decade. For them, dying in the attack is part of the plan. As Bruce Hoffman,
Robert Pape, and other scholars have noted, this explains why suicide terrorism is perhaps the most worrisome threat to homeland security offi39
cials today.
THREE SCENARIOS OF BIOLOGICAL WARFARE
Three basic categorical scenarios of biological warfare can be identified,
based on the amount of the target population that is killed. Each scenario
suggests a different set of motives for the attacker, as well as a different
choice of weapons. In the low-level scenario, anywhere from a small number to 10 percent or 15 percent of the target population is killed. This scenario would be desirable to a rational terrorist attacker intending to create
fear, economic repercussions, and extort compliance with demands.
Historically, when used on the West, such forms of terrorism have
40
worked over time. Societies grow tired, and leaders tend to break ranks
and cut deals to favor their citizens due to the classic “prisoner’s dilemma” of game theory. Political parties attack each other using the fatigue
created by terrorism on opponents for advantage in elections. Even the
United States could play a role in the prisoner’s dilemma problem and
be unwilling to support drastic measures against a perpetrating group,
as long as that group did not intentionally direct its attack against the
United States, much as France, Ital,y and Germany have played this kind
of role in the Middle East relative to the Palestine Liberation Organiza41
tion, Hamas, and Hezbollah. Prior to 9/11, the United States turned a
blind eye to extremist fund-raising within our nation’s borders for
�266
Public Spaces and Social Institutions
Palestinian paramilitary groups. Existing terrorist groups are well aware
of the huge gap between rhetoric and action, and they are very experienced at this kind of international extortion. They have the advantage of
long-term one-man or junta-style rule, which do not require democratic
process, and consequently are able to operate past the time horizon of
election cycles in the West. Such groups could be willing to unleash such
a catastrophic but still low-level biological weapon. In addition, the
attackers would have a good chance to get away undetected, because in
general biological weapons have a gap of days to weeks between when
the attack occurs and when it is detected. This gives the perpetrators time
to cover their tracks, as demonstrated by the anthrax attacks. The fear
induced by these diseases would likely result in massive attempts at retaliation against those who deployed them, if they were known, at least the
first few times it occurred. However, since terrorists do not gain much
by attacks that they do not claim, it is less likely, though not impossible,
that they would resort to the phenomenally draconian attacks discussed
below.
At the medium-level scenario anywhere between 15 percent and 45 percent of the target population would die. At this level of attack things
become murkier. From a game theory point of view, this type of weapon
is a poor choice for a first strike if the attacker is not a nation-state intending to follow up in some manner. From the viewpoint of a terrorist striving to create fear for political gain, it is so draconian in its effect that the
people it was deployed on could be motivated far beyond the ordinary,
and world opinion could potentially tolerate otherwise intolerable measures such as the use of nuclear weapons to utterly eliminate an attacking
group. As with all biological weapons, barring an announcement, it could
be difficult to figure out exactly who was responsible.
It is a commonly held belief that terrorism is not well planned—a series
of desperate acts. This is false. It is another form of war, carefully planned
42
for very specific goals by its leaders. The rank and file may be, in some
cases, desperate, not terribly bright, and the like—simple-minded cannon
fodder. But the leadership plans their acts at least as carefully as a bank
robbery is planned. In the United States, the airliner attacks on 9/11 were
carried out by educated people with good life prospects, quite the opposite of the common thinking. Again, we must understand that for a
classical terrorist group, if no responsibility is taken or assumed, there is
usually little purpose to the attack. Most of terrorist warfare is conducted
for the benefit of the public relations war in the media. Consequently,
there are issues with this type of scenario, which would have difficulty
being claimed. The scenario would not necessarily be claimed, however,
if the attack was a failed attempt to destroy a nation or nations.
The logistics of intentional inoculation of the target populations to the
degree that would probably be required to achieve such high levels of
�Bioterrorism and Biodefense for America’s Public Spaces and Cities
267
casualties could be a serious weak point for the perpetrators. Logistics
tend to conform to Murphy’s Law. Large-scale and complicated deployment logistics are more probable to leave a forensic trail that could be followed and are much more prone to failures that allow interdiction prior to
or during an attack. The number of connections tends to rise logarithmically with the size of a network organization, not linearly. Thus, deployment logistics with double the number of people involved will tend to
be much more than twice as difficult to pull off successfully.
Some would argue that since an attack of this type could potentially
cause blowback and kill much of a nontarget population, it would not be
rational to use it. However, this does not take into account the apocalyptic
fervor of radical martyrdom-seeking groups who may feel themselves to
be living among fellows who are not properly following the one true path,
and hence not important. Nor does it take into account the type of value
system that considers the human race itself to be an environmental blight
upon the planet. An additional argument against believing it would be
irrational to deploy this type of attack is that perpetrators would have
the option of secreting themselves in caves or distant desert regions and
take quarantine precautions with any arriving visitor until the plague
had spent itself. Such a strategy is only marginally more dangerous to
the leadership of a group than was attacking the World Trade Center.
Thus, the views of the type of rational actors connected to viable nationstates must be discarded when considering small splinter groups and
individuals.
At the highest-level scenario, 50 percent to 95 percent of the population
would die, as occurred for native civilizations of North America in the
sixteenth century, and for other civilizations in Europe and Asia during
the spread of the Black Death. From a game theory viewpoint, this moves
into the range of a first strike weapon intended to defeat a nation and is
similar to nuclear weapons in this way. (The USSR had follow-up
43
with biological warfare warheads integral to their nuclear doctrine. )
Deployment of such a weapon becomes more complex and is, again, more
likely to leave a trail to follow; the organism and attack plan becomes
much harder to develop, and it may not be possible for some groups to
complete.
In favor of such an attack is that, absent sophisticated detection
equipment, by the time a sophisticated virus was detected and understood to be a problem, it could be too late. Lacking specific plans, it might
be impossible for the nation to retaliate should it decide to do so. Additionally, there is still the problem of whom to retaliate against, as the
proper party may not be known and, in some cases, may have died intentionally in the attack. Intentional mass suicide by fanatics is not unknown.
For this type of attack, the probability is low that it would be claimed
outright.
�268
Public Spaces and Social Institutions
BIOLOGICAL WEAPON TYPES
There are three basic types of biological weapons: biologically produced toxins such as botulinum toxin, bacterial diseases such as the
bubonic plague or anthrax, and viral diseases such as smallpox or influenza. Biologically produced toxins are essentially a type of chemical weapon, and they are not contagious. This type of weapon could be used for a
low-level scenario such as the theoretical attack described in Proceedings
of the National Academy of Sciences, where the milk supply is inoculated
44
with botulinum toxin and kills tens of thousands of people. Bacterial
and viral diseases can be contagious and thus potentially spread among
the target population, killing even people who were nowhere near the
original attack site.
There are many ways in which biological weapons can be deployed.
They can be applied to human populations directly, such as by spraying
or—as everyone is now aware—some can simply be sent through the
mail. They can be applied to food animals or farm plants, which could
either make the humans consuming the food sick or destroy the food supply for the humans. The results of such an attack were demonstrated by
an incident in Ethiopia in 1888, where the Italian army introduced rinderpest into Africa during its Ethiopia campaign. Some say this was
intentional, some say it was accidental. What is known is that 90 percent
of the cattle died that year in that part of Africa. The result was that
between 60 percent and 90 percent of the people of the region starved to
death and much cultivated land reverted to bush. The biological weapon
could be applied directly to the food itself, such as before distribution to
grocery stores or cafeterias or at the retail location. A weapon could be
encapsulated in various ways developed for pharmaceutical delivery,
applied to anything from clothing to paper money, to fragments in a suicide bomb, or perhaps released into the ventilation system of a subway
or building. It could be injected into homeless people or mixed with illegal drugs to infect users. The specific way to apply the biological weapon
45
depends upon the organism and what the attacker desires to achieve.
BASIC STRATEGIC ELEMENTS OF BIOLOGICAL WARFARE
The method by which a target population is infected by a biological
weapon is called the initiating vector. There are a number of types of
possible initiating vectors: aerosol, material on a surface, through the
food or water supply, through injection, or intentional person-to-person
contagion.
Taken alone all of these methods are of limited scope and highly
unlikely to have fatality rates that are very high, unless the agent is contagious. The scope may be the size of a city or, even conceivably, some
�Bioterrorism and Biodefense for America’s Public Spaces and Cities
269
degree of coverage of an entire state. For instance, if an attacker sprayed
an entire city such as San Francisco with weaponized anthrax (anthrax
ground to 5 micron powder), using the methods developed successfully
46
by the U.S. Navy, the city and communities in its wind pattern swath
for the time of the attack would be the only area affected, since anthrax
has virtually no level of contagion. Make no mistake; properly done, such
an attack could kill a million or more people. However, it would not go
significantly beyond the first level of infection experienced by those
directly attacked.
Person-to-person contagion is what will kill millions, tens of millions,
perhaps billions of people. In the modern era, with reasonably effective
antibiotics and sanitation, the most likely weapon to cause very large
numbers of deaths are viruses, because bacteria are too easy to control.
FUNDAMENTALS OF BIOLOGICAL WARFARE DEFENSE FOR
PLANNERS
Planners for a local region should keep in mind that the higher the level
of the attack, the more likely it is that a city or town will be on its own. If
casualties are excessive across a large region, the ability of federal and volunteer agencies such as the Federal Emergency Management Agency or
the Red Cross will be highly compromised. Thus, it makes sense for local
planners to put some thought into what they would do in such a situation.
Casualties are a primary concern for any response planner. The first priority for any responsible unit is how many casualties there are, who and
where they are, and how this will affect their ability to operate effectively.
If response units are unable to function, they cannot play a role in helping.
Biological weapons defense is like public health in general with one
main additional element. As with any public health matter, each individual needs to be able to avoid becoming infected by taking basic steps.
The additional element is that with biological weapons, attempts can be
made to try to detect perpetrators before and while they carry out their
plans. Intelligence personnel need to learn to detect signs that a clandestine bioweapons lab exists. They should also attempt to monitor the operations of people who have the motive and potentially the capacity for a
biological attack.
The earlier one can detect a dangerous organism, the earlier one can
respond to it. As in fire suppression, if nobody reports a fire to the fire
department, it can get out of control. The thought process is the same as
for setting up a secure perimeter. Just as there is no security without detection, there is no security without the ability to respond to events. All walls
can be breached, and there is nothing different about disease monitoring
systems. Current day monitoring systems are set up to notice death
events, mostly in healthy adults and children. For a serious attack
�270
Public Spaces and Social Institutions
scenario, by the time the first deaths appear, things should be—from the
attacker’s perspective—on track.
Monitoring for dangerous organisms falls into three major categories:
instrumentation, public health epidemiology, and human intelligence
work. Sophisticated air monitors for use over cities, stadiums, and in other public spaces are useful in that they are one of the few ways to detect an
attack as it is happening by aerosol application. There are low-cost manual options available for sale, which can work, that can be found through
Internet searches for those locales unable to afford expensive air monitors.
The basic limit of this instrumentation is that it will not detect what it was
not designed to detect—i.e., a new disease could go unnoticed.
Public health and the medical system is the most fundamental aspect of
biodefense at all levels. It should be the first priority before all others for
those in a limited funding situation. Public health is what finds those
odd cases that could indicate an epidemic is about to start. Public health
is also the segment which is going to find a disease which is “off the
charts” that an instrument will not notice. Care should be taken to find a
way to shore up public health and disease monitoring so that it reaches
all segments of society. It is in the strata of society not served by medical
care that an epidemic is most likely to take hold and gather steam invisibly. (In point of fact, this is already occurring due to inattention and fail47
ure due to natural disease, albeit in relatively minor ways at present.)
Like forest fires, epidemics are easiest to stop in the earliest stages. Once
epidemics really get rolling, the task becomes very difficult, if not impossible, and expands to a pandemic relatively easily.
Once a biological weapon has been detected, the modes of contagion
need to be identified, and a plan of action to stop the spreading of the disease must be established. The most contagious diseases can survive on a
48
surface for periods from minutes to, in extreme cases, weeks or months.
The primary ways a significant bioweapon disease is likely to enter the
body are through eye or pulmonary contact. Hand to eye or aerosol to
eye works because eye membranes are a prime way for viruses to enter
the body. Hand to mouth and aerosol to mouth are another way, as well
as hand or aerosol to food and then into the body, or hand or aerosol to
nose membranes and lungs.
While determining the mode of contagion, a general response that
focuses on cleanliness of hands and surfaces, avoiding touching hands
to eyes, nose, and mouth without washing, and possibly the use of filter
masks is in order. Training people not to touch their eyes, nose, mouth,
or food without careful washing of their hands will go a long way toward
interrupting the spread of infection. Wearing of simple masks can help by
lowering the amount of discharge through the air. Nonrated masks (ordi49
nary surgical masks, not N95-rated ) will be of some use for avoiding
inhaling droplets containing contagious organisms, but primarily they
�Bioterrorism and Biodefense for America’s Public Spaces and Cities
271
help to contain spreading of disease from the wearer to others. All masks
need to be replaced regularly and either disinfected or disposed of in a
sanitary manner or they can become a problem in and of themselves. A
mask that is left on a person’s face for long periods of time and reused
without disinfection can harbor infectious organisms in its fabric, which
stays nicely warmed and damp from breathing—a great environment
for most organisms to survive. Such a mask can itself become a possible
health hazard in an area where infectious disease is present.
Diseases spread by feces, blood, semen, or other secretions are easily
preventable in an educated population and thus not a likely major bioweapons threat in the developed world. (However, as we have seen with
HIV, just because a disease is quite preventable does not mean it will not
spread significantly in a population.)
50
Person-to-person contagion takes place through networks of people.
Deal with the infectious connections between people and you will deal
with the disease transmission. This is the principle of quarantine as well
as sanitation and disease barriers such as masks, gloves, and eye protection. Quarantine is a powerful means of stopping the spread of disease if
applied effectively, but if done badly, an attempted quarantine can make
51
things worse. Quarantines have standards that should be met. As
defined by Ross Upshur, a public health expert at the University of Toronto, these are the following:
1. Standard of harm: clear and measurable harm to others will occur from the
disease.
2. Least restrictive: use of [the] least restrictive means appropriate to the goal of
disease control.
3. Reciprocity: if society asks people to accept loss of liberty, society has an obligation to help them.
4. Transparency: authorities have an obligation to communicate clearly the reasons for quarantine and allow for discussion and appeal of decisions.
Per Upshur, given the above four standards being met, small-scale quarantines such as that for SARS have been quite effective with mostly volun52
tary compliance. (Upshur records 22 involuntary detentions out of more
than 3,000 voluntarily requested detentions during the SARS epidemic, a
voluntary compliance rate of better than 99 percent.)
Public health planners should think intelligently about where and how
most disease transmission occurs in their communities by type of illness.
This is a significant aspect of quarantine planning and goes toward fulfilling the second standard that quarantines should be least restrictive. For
example, in Japan, holding young children at home during influenza epidemics and vaccinating healthy children has decreased mortality in the
53
elderly. The basics of what constitutes effective and ineffective
�272
Public Spaces and Social Institutions
interruption of disease transmission is something all public officials can
grasp. A community giving this some serious thought will be ahead of
the game.
Poorly implemented quarantine is worse than nothing at all. Anyone
considering imposition of quarantine on a large scale should understand
that what people are ordered to do and what they actually do are often
quite different things. This is one of the reasons for using the four principles above as standards. People motivated to escape quarantine have lied
about their condition and thereby spread a contagious disease in past
plagues. People who become desperate because they feel they have been
forgotten, or think they are certain to die if they do not escape, are likely
to act in a manner that can make real quarantine not only impossible,
but make any attempt to impose such a quarantine a sure way to spread
the disease even faster. This can become a very serious matter in a largescale biological attack pandemic.
A vaccination program is a different method of interrupting the network of transmission from person to person. Vaccination will work if a
vaccine is available. The problem with vaccines is that they take time to
develop and are unlikely to be available for novel organisms. There are
techniques that may possibly be applied in a high-level scenario to
attempt to vaccinate with a quickly developed, perhaps problematic vac54
cine. However, detailed discussion of vaccines is beyond the scope of
this chapter.
55
Care should be taken to always look forward during an epidemic.
Accurate information on where things stand is crucial, but this should
not be allowed to turn into a hindsight exercise by officials or responders.
An epidemic is like a slow-motion tsunami. Try to stay five to ten infection
cycles ahead of an epidemic with logistics. Understand that even if all
new infections stop on any particular day, those incubating the disease
have yet to show themselves. Since each infection usually takes 5 days
or so for the newly infected person to become infectious in his or her turn,
this means trying to keep 25 to 50 days’ forward projection on estimates,
supplies, facilities, and personnel. Rare outliers can develop a disease
much later than expected, which can potentially reignite an epidemic.
Planners should understand the legal tools that they have, as well as the
public health network that is set up. Basic recommendations include the
following:
1. Basic public health is very easy to let go, onerous, and rather thankless. For
these reasons there must be regular reviews and visits to public health offices
and personnel to evaluate whether any portion of a locale’s population is
falling through the cracks. This includes homeless who live in public spaces,
illegal immigrants, and others who are poor or marginal, particularly if they
may come into contact with the public. Prostitutes, drug addicts, drug dealers,
�Bioterrorism and Biodefense for America’s Public Spaces and Cities
273
slum dwellers, and others who shy away from authorities should not be
overlooked, and some method of accommodating access to them by public
health officials must be made. To do so may require working out deals
between public health officials, police, and the local district attorney’s office to
aid in accomplishing full coverage. It should be possible to coordinate with
the health care system in the area that serves the rest of us.
2. Get local government, district attorneys, police, forensics, public health officials, and others appropriate to meet together to improve communications
and understanding of issues. All parties should have a basic grasp of the law,
what can happen, how contagious disease works, who is responsible for what,
and what the challenges are for other departments. In the midst of an epidemic crisis is not the time to be setting up systems and figuring out what to
do, and higher level state, federal, or transnational officials may or may not be
56
prepared.
3. Develop and review plans that do not leave out scenarios wherein federal and
state agencies may be incapable of helping for a prolonged period.
4. Keep public areas sanitary and clean. This most basic of steps is, nevertheless,
of great importance for public health in cities and public spaces.
5. Have on hand basic protective gear appropriate to an epidemic. Basic gear
includes gowns, gloves, N95-rated respirator masks, eye protection, and disinfectant. As many people as possible should be trained in sanitation, infection routes into the body, how to scrub clean, use of basic protective gea,r and
habits appropriate to an infectious area. As a note, high-end isolation suits are
sometimes desirable, but they require careful maintenance, and they are quite
cumbersome and hot to wear. A person can be comfortable in shirtsleeves in
freezing temperatures inside an isolation suit. (Personnel who decontaminate
illegal drug production labs know all about the problems with wearing such
equipment.) Additionally, medical personnel have survived epidemics of
Ebola in Africa while using standard gear and less, even simple washing with
soap together with liberal use of disinfectants like Clorox. Personnel under the
same circumstances using protective gear have died awful deaths from simple
mistakes such as brushing their eyes before washing their hands.
6. Keep apprised on current recommendations made for dealing with any epidemic or pandemic potential disease that is believed to be of significant
probability. In the current public health environment, this means awareness of
the need to stockpile oseltamivir (used in the treatment of the infection caused
by the flu virus) or similar drugs.
CONCLUSIONS AND RECOMMENDATIONS FOR RESEARCH
No type of attack except nuclear weapons has as much capacity to create mass death as bioterrorism. For terrorist groups unable to field large
numbers of nuclear tipped ICBMs, even nuclear weapons are relatively
small when compared to bioterrorism potentials. The historical and
potential capability of disease and bioterrorism to create mass death quite
�274
Public Spaces and Social Institutions
simply boggles the mind when examined carefully. The fact is that tens of
thousands of people die each year of infectious disease already. This will
continue, and we must prepare for the inevitable incidence of both manmade and natural infectious disease plagues that make large inroads into
our population. It is difficult for those of us in this modern era to conceive,
but overwhelming plagues are possible. Death rates of 50 percent to
95 percent have not occurred on a large scale in the past 100 years, but
they have occurred on a small scale on the islands in the Pacific in the cur57
rent era as recorded by Thor Heyerdahl. Even relatively minor biological
attacks outlined in this chapter would be considered catastrophic by any
reasonable yardstick.
The most fundamental priority for biodefense is to support public health in
order to make disease problems visible as rapidly as possible. Public health with
disease is like transparency of accounting in finance. If you cannot see it,
you cannot do anything about a problem. Of special concern is ensuring
that public health officials contact, monitor, and treat the invisible uninsured, the poor, the illegal immigrant, the prostitute, the underclass drug
abusers, the homeless, and similar people relative to infectious disease.
This underclass is the most vulnerable to epidemic disease, least likely
to take precautions, and most in need of money, causing them to go to jobs
while infectious and seriously ill. Most important, this underclass physically permeates our society virtually everywhere. These people clean our
offices, work as nannies, get picked up as day labor for all kinds of projects, make beds in hotels, prepare food in kitchens, clean our cars, enter
our homes as maids or ladies of the night, and lie in doorways at night
all while society looks the other way. They are the most likely to be malnourished, weakened from fatigue, overwork, or drug use, and most
likely to be ignorant and fearful of authorities. They are, in short, the perfect invisible network for epidemic disease to take hold in and get passed
on to the more wealthy layers of our society. That disease can be natural or
man-caused. A smart attacker will understand their value for penetrating
into our society.
There is no substitute for good human intelligence in bioterrorism. Proposing
to detect bioterrorism before or even at the outset of an attack is mostly
impossible by any other means. (The one known exception is aerosol
attack if a monitored organism is used.) Consequently, improvements in
intelligence gathering and detective work should be made in the area of
biological weapons. These people should be trained in biological weapons
development and scenarios, so that they are capable of understanding
what is going on in a laboratory they may encounter. They need to be able
to work with and understand the types of scientist personalities that they
will meet. They should be good at human networking and developing
trust in the scientific community. However, they must also be cognizant
of dark human motivations and capable of dealing with them.
�Bioterrorism and Biodefense for America’s Public Spaces and Cities
275
A highly controversial area of bioterrorism intelligence gathering, particularly domestic, is targeting of select religious cults for infiltration or
monitoring. Monitors can be recruited from the organization, or, in select
cases, infiltrators could be placed. The reason is simple; such groups have
been the source of most bioterror attacks and attempts of known origin in
the past 50 years. The constitutional issues in the United States are not
small. However, in this case we can correctly say that “The Constitution
is not a suicide pact.”
These organizations are not primarily made up of hardened criminals,
58
but of alternate theology idealists. In most cases of religious cults, since
members of such groups are typically poor, there is always a wide range
of adherence to the tenets, and many find themselves wanting to feel more
powerful over time, a simple recruitment by advertisement or site visits
followed by “social recruitment” or payment of members to be monitors
could be quite effective.
Improvements in technological monitoring/diagnostic capability are
an area that biodefense needs to continuously develop. The reason for this
is that the main line of defense is prevention of new infection and containment of existing infections, not treatment. That means that the earlier
infection can be diagnosed, the more likely it is that the infection can be
prevented from spreading to others. Again, the transparency metaphor
in finance is an apt one. Even today, infectious disease “accounting”
would not pass muster for a finance accountant. What accountant would
accept that somewhere between $700,000 and $2.7 million is spent on a
program? And yet, that is what our disease statisticians are able to
account for about malaria deaths, through no fault of their own. We can
do better, and we should.
Two high-return proposals for improvements in disease monitoring
follow:
• Backing the development of low-cost consumer use disease diagnostics. This would
create a device about the size and cost of a cell phone, which could be used by
any consumer to diagnose what organisms are infecting them. This device
would have to be capable of diagnosing hundreds of disease organisms simultaneously. The disposable diagnostic element should cost no more than $5 each,
preferably less. With 17 million mothers in the United States, such a device
could be popular enough with consumers to self-fund once it got rolling. An
early patriotic push to get people to buy and use them once they have sufficient
breadth of enough diagnostic ability could also work to get a critical mass of
users for mass production self-sustenance. This will function as a kind of DEW
(Distant Early Warning radar for incoming ICBM and enemy aircraft) line for
disease in the public. It should provide much improved public health information and improve our ability to track infectious disease of all types. Such devices
could be based on either antibody or DNA/RNA detection using today’s
technology.
�276
Public Spaces and Social Institutions
A device of this kind faces serious business obstacles and needs government
intervention to be deployed. Laboratories do not want to lose business to a
consumer device, which in fact has prevented a major European supplier from
fielding a consumer diagnostic device of this general class. A further problem is
that venture capitalists want to see patent protection for a product. While there
are a variety of technologies that have patent potential, there are many that do
not that could be equally effective and less expensive. This tends to curtail private investment at the critical stages past initial conception. Last, there are
serious regulatory hurdles, and the cost of certifying each separate diagnostic
test is large. Multiply those hurdles and certifications by 100 to 500 organisms
and one has a prohibitively high investment cost with too little return on
investment for the level of perceived risk for private money—hence the need
for government involvement.
• The proposal of the Viral Defense Foundation to sample excess blood serum across
the country and analyze it for viruses is the most sensible mass-monitoring proposal on
59
record. The purpose of this effort is twofold. First is to establish a baseline of
true morbidity (i.e., what is really normally present in humans) from which to
compare. Second is to allow us to have a chance to detect pathogens that may
not be immediately obvious and to do so quickly in order to allow rapid
response. To accomplish this at a reasonable cost requires further research and
development in mass sequencing of viruses to identify them. That research and
development is occurring. This project will represent an ongoing cost, well
worth the investment for epidemiology data and biodefense. This elegant
approach avoids the inherent “needle in a haystack” problem of monitoring the
environment that is home to astronomically large numbers of microorganisms,
mostly benign.
Additionally, there is a need for improvements to vaccine development and pro60
duction that are technical, financial, and regulatory. Current efforts have
begun to stimulate vaccine providers to be willing to put research and
development money into influenza, smallpox, and other vaccines. It is
good that legislators have begun to grapple with the issues. That should
continue and expand.
Also, focus should be put on how to quickly develop and deploy a useful—even if imperfect—vaccine against novel pathogenic viruses for use
in extreme situations. With the note that not all viruses can have a vaccine,
this research should set a goal of initiation to deployment in 21 to 28 days
or better, which is a number currently considered impossible. While it
may be an impossible standard to meet, there is reason for this goal, and
challenging goals do have a way of eventually being met once seriously
sought. The reason for this three to four week deployment goal is that if
a novel pathogen is engineered and deployed successfully in a high-level
sophisticated attack, a short time may be available to interrupt its spread
before an epidemic takes hold. However, if it does take hold, epidemics
have a cycle time dependent on the time it takes for the pathogen to cause
�Bioterrorism and Biodefense for America’s Public Spaces and Cities
277
a new individual to become infectious, which is, with most viruses,
approximately five to seven days. The number of potentially infected people will tend to rise logarithmically, but after three to four weeks, there
will still be a large proportion of the population as yet uninfected.
There would be several basic aims of this high-speed vaccine development research. One is to identify ways that are reasonably reliable at presenting antigens in a way that causes the adaptive immune system to
respond, one possible example being the work of Verardi et al. and Yilma
61
et al. It should not, however, be construed that the mentioned methods
are the only or best, since this is a new area to explore. Another aim is to
identify ways to get the vaccine produced and out to the population rapidly. (One example strategy is to use a modified live virus and have those
who receive the initial vaccine become the culture medium for intentionally spreading the vaccine virus.) Also, this research should identify vaccine methods of this kind that are likely to cause minimal casualties from
the vaccine itself. The vaccine produced in this way would be used only in
the most unusual circumstances, when it would be the best option available to deal with a high-level biowarfare attack. Research and study in
this area is needed.
Improved, longer wearing, and comfortable isolation suits should be
developed. Current technology in this area dates back half a century in
its concept. The equipment is hot, clumsy, and prone to rips, tears, and
abrasion. It needs careful maintenance. It does not seal itself or respond
to damage even for a short period of time. The surfaces require careful
decontamination after use, as they are not self-cleaning in any way. Additionally, current protective gear is very expensive. We can do better in all
respects, and we should. We should aim to make comfortable, longwearing, virtually self-maintaining gear available to the general public
at a price they can afford.
Disease organisms, used as bioweapons, have a terrible capacity to
cause harm. Officials and responders who do find themselves in the midst
of a serious epidemic, be it man-made or natural in origin, are not powerless even if they have little or nothing to address it with. If they understand how infectious disease spreads, and how the specific disease they
are experiencing spreads, then they can do their best to interrupt the chain
of transmission from person to person. The primary work in this area is
very practical, focused on prevention and seeing to it that no segment of
society is allowed to “fall off the radar.” Prevention by straightforward
measures such as soap, water, cleanliness, and disinfectants interrupt the
spread and are excellent methods because viral diseases are generally
quite difficult to treat. There are few drugs available, though they do exist.
Cleanliness, treating patients for symptoms with supportive therapy, and
teaching people how to avoid infecting themselves can work. However,
no one should be fooled by the basic nature of much that is necessary to
�278
Public Spaces and Social Institutions
address bioterrorism into not taking it seriously. Our high-tech age has a
tendency to do so. Addressing bioterrorism is a pragmatic combination
of simple low-tech methods with very advanced high-tech methods
where it makes sense.
Last, we should never forget: disease has reshaped the politics of the
world multiple times already—we are all descendants of the survivors.
Disease is likely to do so again. World-changing disease in the modern
world is most likely to appear from the hand of man. We must be
prepared.
ACKNOWLEDGMENTS
This discussion will be considerably expanded in a forthcoming book on biological warfare and biodefense by the authors.
NOTES
1. Ole Jorgen Benedictow, The Black Death 13461353: The Complete History (New
York: Boydell Press, Woodbridge, Suffolk, & Rochester, 2004).
2. Giovanni Boccaccio, The Decameron (New York: Dell, 1972).
3. Ibid.
4. Johannes Nohl, The Black Death (New York and Evanston: Harper & Row,
1969).
5. Fray Toribio Motolinia, Historia de los indios de la Nueva Espana, trans. Elizabeth Andros Foster (Berkeley, CA: Cortes Society, 1568).
6. William Bradford. Of Plimoth Plantation 1620–1647 (New York: Modern
Library, 1981); and Henry F. Dobyns, Their Number Become Thinned: Native American Population Dynamics in Eastern North America (Knoxville: University of Tennessee Press, 1983).
7. Bradford, Of Plimoth; Dobyns, Their Number Become Thinned; James Axtell,
“Europeans, Indians, and the Age of Discovery in American History Textbooks,”
American Historical Review 92 (1987): 627; Alfred Crosby, Ecological Imperialism:
The Biological Expansion of Europe, 900–1900 (Cambridge: Cambridge University
Press, 1993); Thor Heyerdahl, Aku-Aku (Chicago: Rand McNally, 1958); Charles
M. Segal and David C. Stineback, Puritans, Indians, and Manifest Destiny (New
York: Putnam, 1977); and Russell Thornton, American Indian Holocaust and Survival:
A Population History since 1492 (Norman: University of Oklahoma Press, 1987).
8. Bradford, Of Plimoth; Dobyns, Their Number Become Thinned; Axtell, “Europeans, Indians, and the Age of Discovery”; Crosby, Ecological Imperialism; Heyerdahl, Aku-Aku; Segal and Stineback, Puritans, Indians, and Manifest Destiny; and
Thornton, American Indian Holocaust and Survival.
9. Laurie Garret, Betrayal of Trust: The Collapse of Global Public Health (New York:
Hyperion, 2000).
10. Jared Diamond, Guns, Germs and Steel: The Fates of Human Societies (New
York: W. W. Norton and Company, 1999).
�Bioterrorism and Biodefense for America’s Public Spaces and Cities
279
11. Avert.org. World estimates of the HIV and AIDS epidemics at the end of 2004
(2005) http://www.avert.org/worldstats.htm (accessed October 12, 2005).
12. “Africa Aids Orphans ‘May Top 18m,” BBC News, October 25, 2005, http://
news.bbc.co.uk/2/hi/africa/4373576.stm (accessed November 3, 2005).
13. Centers for Disease Control and Prevention (CDC), “Influenza: The Disease,” 2004, http://www.cdc.gov/flu/about/disease.htm (accessed October 29,
2005).
14. United Nations, “AIDS: Report on the Global HIV/AIDS Epidemic,”
December 1997.
15. Gregory Armstrong, Laura Conn, and Robert Pinner, “Trends in Infectious
Disease Mortality in the United States during the 20th century,” Journal of the American Medical Association 281 (January 6, 1999): 61–66.
16. Armstrong, Conn, and Pinner, “Trends in Infectious Disease Mortality.”
17. Ibid.
18. Zbigniew Brzezinski, Out of Control: Global Turmoil on the Eve of the TwentyFirst Century (New York: Scribner, 1993).
19. CDC, “Malaria Facts” (National Center for Infectious Diseases, Division of
Parasitic Diseases, 2004). http://www.cdc.gov/malaria/facts.htm#WorldMalaria
(accessed October 29, 2005).
20. B. Hearn, “Malaria Clock” (2002), http://www.junkscience.com/
malaria_clock.htm (accessed October 27, 2005).
21. UN, “AIDS: Report on the Global HIV/AIDS Epidemic,” December 1997.
22. CDC, “Information About Influenza Pandemics” (2005), http://
www.cdc.gov/flu/avian/gen-info/pandemics.htm (accessed October 29, 2005).
23. Phil Hirschkom, “New York Reduces 9/11 Death Toll by 40,” CNN, October 29, 2003, http://www.cnn.com/2003/US/Northeast/10/29/wtc.deaths
(accessed October 27, 2005).
24. Maria Jesus Prades, “Three Charged In Madrid Bombing,” CBS News,
March 19, 2004, http://www.cbsnews.com/stories/2004/03/22/world/
main607757.shtml (accessed October 27, 2005).
25. CDC, “Influenza.”
26. This chapter covers scenarios that range from relatively low (less than 1 percent of the targeted population dying) to those at the high end of very serious military significance (up to 95 percent of the targeted population dying) that could
result from bioterrorism. For general background reading on public health issues,
the reader is referred to Laurie Garret, Betrayal of Trust: The Collapse of Global Public
Health (New York: Hyperion, 2000); and Jared Diamond, Guns Germs and Steel: The
Fates of Human Societies (New York: W.W. Norton and Company, 1999).
27. Sun Ai Raillard et al. “Novel Enzyme Activities and Functional Plasticity
Revealed by Recombining Highly Homologous Enzymes,” Chemistry & Biology 8
(September 2001), 891–98; and Jon E. Ness et al. “Synthetic Shuffling Expands
Functional Protein Diversity by Allowing Amino Acids to Recombine Independently,” Nature Biotechnology 20 (December 2002): 1251–55.
28. Keith A. Powell et al. “Directed Evolution and Biocatalysis,” Angewandte
Chemie International (English Edition) 40 (November 5, 2001): 3948–59.
�280
Public Spaces and Social Institutions
29. Larry P. Wackett, “Directed Evolution of New Enzymes and Pathways for
Environmental Biocatalysis,” Annals of the New York Academy of Sciences 864
(December 13, 1998), 142–52; and Linda A. Castle et al., “Discovery and Directed
Evolution of a Glyphosate Tolerance Gene,” Science 304 (May 21, 2004), 1151–54.
30. Judith Miller, Stephen Engelberg, and William Broad, Germs: Biological
Weapons and America’s Secret War (New York: Simon & Schuster, 2001).
31. Arnold M. Ludwig, King of the Mountain: The Nature of Political Leadership
(Lexington: University Press of Kentucky, 2002).
32. Ken Alibek and Stephen Handelman, Biohazard: The Chilling True Story of the
Largest Covert Biological Weapons Program in the World—Told from the Inside by the
Man Who Ran It (Random House, New York, 1999).
33. Larry Henry, “Harris’ Troubled Past Includes Mail Fraud, White Supremacy,” Las Vegas Sun, February 23, 1998, http://www.lasvegassun.com/dossier/
crime/bio/harris.html.
34. Testimony of General John Abizaid, senior officer in Central Command, to
the Senate Armed Services Committee on September 29, 2005; see Jim Garamone,
“Will, Resolve Key to Defeating Terror, Leaders Say,” American Forces Information
Services, September 29, 2005, http://www.defenselink.mil/news/Sep2005/
20050929_2885.html; and David von Drehle, “Wrestling with History,” Washington
Post, November13, 2005, W12.
35. Marc Sageman, Understanding Terror Networks (University of Pennsylvania
Press, Philadelphia, 2004).
36. Ibid.
37. Rick A. Ross, “Osho/Rajneesh” (Jersey City, NJ: The Rick A. Ross Institute,
2001), http://www.rickross.com/groups/rajneesh.html (accessed October 29,
2005); and Christopher Calder, “Osho, Bhagwan Rajneesh, and the Lost Truth”
(2000), http://home.att.net/~meditation/Osho.html (accessed October 29, 2005).
38. Robert J. Lifton, “‘In the Lord’s Hands’—America’s Apocalyptic Mindset,”
World Policy Journal 20, no. 59 (Fall 2003).
39. For example, see Bruce Hoffman, The Logic of Suicide Terrorism: Lessons
from Israel that the U.S. Must Learn,” The Atlantic Monthly (June 2003); and Robert
Pape, The Strategic Logic of Suicide Terrorism, in Homeland Security and Terrorism:
Readings and Interpretations, ed. Russell Howard, James Forest, and Joanne Moore
(New York: McGraw-Hill, 2005).
40. Alan M. Dershowitz, Why Terrorism Works: Understanding the Threat,
Responding to the Challenge (New Haven and London: Yale University Press, 2002).
41. Dershowitz, Why Terrorism Works.
42. Dershowitz, Why Terrorism Works.
43. Ken Alibek and Stephen Handelman, Biohazard: The Chilling True Story,
1999.
44. Lawrence M. Wein, and Yifan Liu, “Analyzing a Bioterror Attack on the
Food Supply: The Case of Botulinum Toxin in Milk,” Proceedings of the National
Academy of Sciences 102 (July 12, 2005): 9984–89.
45. For more on this topic, please see the forthcoming volume by the authors of
this chapter.
�Bioterrorism and Biodefense for America’s Public Spaces and Cities
281
46. Miller, Broad, and Engelberg, Germs: Biological Weapons and America’s Secret
War.
47. Laurie Garret, Betrayal of Trust: The Collapse of Global Public Health (Hyperion, New York, 2000).
48. Ibid.
49. This designation means that the mask is 95 percent effective against any
particle that is over 1 micron.
50. Gerardo Chowell and Carlos Castillo-Chavez, “Worst Case Scenarios and
Epidemics,” in Bioterrorism: Mathematical Modeling Applications in Homeland Security, ed. Carlos Castillo-Chavez and H.T. Banks (Philadelphia: SIAM, 2003), 35–51;
Stephen G. Eubank, “Social Networks and Epidemics” (Los Alamos National Laboratory, 2003), http://www.ima.umn.edu/talks/workshops/11-3-6.2003/
eubank/eubank.ppt (accessed October 28, 2005); and Matt J. Keeling and Ken T.
D. Eames, “Modeling Dynamic and Network Heterogeneities in the Spread of Sexually Transmitted Diseases,” Proceedings of the National Academy of Sciences 99
(2002): 13330–35.
51. Ross E. Upshur, “Principles for Justification of Public Health Intervention,”
Canadian Journal of Public Health 93 (2002): 101–3.
52. Ibid.
53. W. Paul Glezen, “Influenza Vaccination for Healthy Children,” Current
Opinion in Infectious Diseases 15 (June 2002), 283–87.
54. Paulo H. Verardi et al., “Long-term Sterilizing Immunity to Rinderpest in
Cattle Vaccinated with a Recombinant Vaccinia Virus Expressing High Levels of
the Fusion and Hemaglutinin Glycoproteins,” Journal of Virology 76 (January
2002): 484–91; and Tilhun D. Yilma et al., “Inexpensive Vaccines and Rapid Diagnostic Kits Tailor-Made for the Global Eradication of Rinderpest, and Technology
Transfer to Africa and Asia,” Developmental Biology 114 (2003): 99–111.
55. Jaro Kotalik, “Preparing for an Influenza Pandemic: Ethical Issues,” Bioethics 19 (August 2005): 422–31.
56. Bradley T. Smith et al., “Navigating the Storm: Report and Recommendations from the Atlantic Storm Exercise,” Biosecurity and Bioterrorism: Biodefense
Strategy, Practice and Science 3 (2005), 256–57.
57. Thor Heyerdahl, Aku-Aku (Chicago: Rand McNally, 1958).
58. David G. Bromley and Anson D. Shupe, Strange Gods (Beacon Press, Boston,
1981).
59. Norman G. Anderson and Leigh Anderson, VIROME project—Rapid
Detection/Rapid Response (Kensington, MD: Viral Defense Foundation, 2003),
http://www.viraldefense.org (accessed November 10, 2005).
60. Jaro Kotalik, “Preparing for an Influenza Pandemic”; Lars Noah, “Triage in
the Nation’s Medicine Cabinet: The Puzzling Scarcity of Vaccines and Other
Drugs,” South Carolina Law Review 54 (Winter 2002): 371–403; K. Groeneveld and
J. van der Noorda, “Use of Antiviral Agents and Other Measures in an Influenza
Pandemic,” Netherlands Journal of Medicine 63 (October 2005): 339–43; Thomas C.
Jones, “A Call to Restructure the Drug Development Process: Government OverRegulation and Non-Innovative Late Stage (Phase III) Clinical Trials are Major
Obstacles to Advances in Health Care,” Science and Engineering Ethics 11 (October
�282
Public Spaces and Social Institutions
2005): 575–87; and Monica Shoch-Spana, Joseph Fitzgerald, and Bradley R. Kramer
(UPMC Influenza Task Force), “Influenza Vaccine Scarcity 2004-05: Implications
for Biosecurity and Public Health Preparedness,” Biosecurity and Bioterrorism: Biodefense Strategy, Practice and Science 3 (2005): 224–34.
61. Paulo H. Verardi et al., “Long-Term Sterilizing Immunity,”; and Tilhan D.
Yilma et al., “Inexpensive Vaccines.”
�
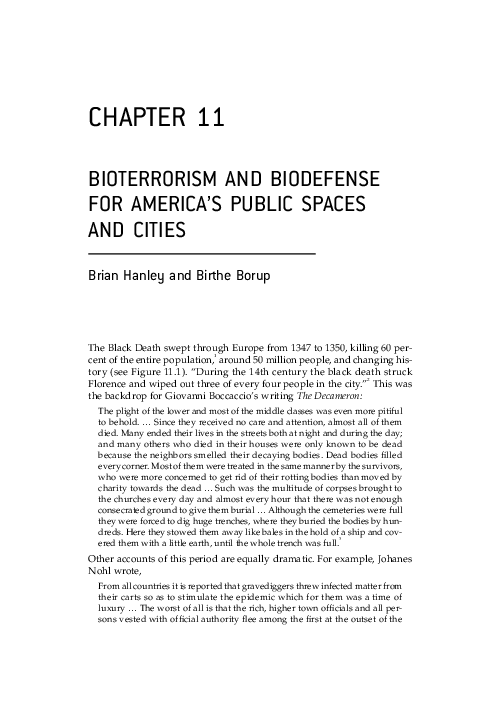
 Brian Hanley
Brian Hanley