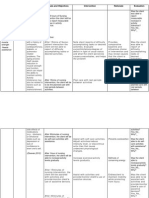
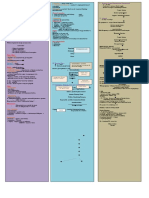
Psych - Nursing Interventions
Psych - Nursing Interventions
Download as doc, pdf, or txt
You might also like
- Techno-Elementals by David SpanglerDocument122 pagesTechno-Elementals by David Spanglerpunkmaster13000No ratings yet
- The Self-Worth Theory of Achievement MotivationDocument18 pagesThe Self-Worth Theory of Achievement Motivationkangalbert86No ratings yet
- Pathophysiology of DMDocument2 pagesPathophysiology of DMShelly_Ann_Del_9959No ratings yet
- 2 6 7 HypervolemiaDocument4 pages2 6 7 HypervolemiaMaica LectanaNo ratings yet
- Contemporary Nursing TheoriesDocument13 pagesContemporary Nursing Theoriessagami.gNo ratings yet
- NCM 107 Module 2M Ethico Moral Aspects of NursingDocument18 pagesNCM 107 Module 2M Ethico Moral Aspects of NursingTrisha ApillanesNo ratings yet
- NCLFNP - Mr. Robert McClelland CaseDocument4 pagesNCLFNP - Mr. Robert McClelland CaseAiresh Lamao50% (2)
- Buddhism BrochureDocument3 pagesBuddhism Brochuremarie55% (11)
- Process RecordingsDocument4 pagesProcess RecordingsJayakrishnan P KripNo ratings yet
- Monsalud - Drug StudyDocument5 pagesMonsalud - Drug StudyJanielle Christine MonsaludNo ratings yet
- Case Study FormatDocument5 pagesCase Study FormatEden OlasabNo ratings yet
- COPARDocument12 pagesCOPARGlenn Asuncion PagaduanNo ratings yet
- MseDocument11 pagesMseClyde R.OrtegaNo ratings yet
- Acute PainDocument3 pagesAcute PainGerardeanne ReposarNo ratings yet
- CASE SCENARIO and NCPDocument14 pagesCASE SCENARIO and NCPBeverly PagcaliwaganNo ratings yet
- Cultural Competence and Perceptions of Filipino Nurses On Effectiveness of Reducing Health Care DisparitiesDocument7 pagesCultural Competence and Perceptions of Filipino Nurses On Effectiveness of Reducing Health Care DisparitiesChristine Elaine Batusin IlaganNo ratings yet
- Republic of The Philippines Tamag, Vigan City 2700 Ilocos Sur Website: MailDocument2 pagesRepublic of The Philippines Tamag, Vigan City 2700 Ilocos Sur Website: MailRenea Joy ArruejoNo ratings yet
- Nursing Care PlanDocument13 pagesNursing Care Planyumiko0% (1)
- Reflection On Feeding Elderly ClientsDocument2 pagesReflection On Feeding Elderly ClientsLaydee GiaAmNo ratings yet
- Nursing InterventionDocument7 pagesNursing InterventionChia OliverNo ratings yet
- Week 5 NCM 419Document40 pagesWeek 5 NCM 419mateomarius64No ratings yet
- Week 3. COURSE TASK - Acute PancreatitisDocument3 pagesWeek 3. COURSE TASK - Acute PancreatitisqwertNo ratings yet
- Assessing General Health Status and Vital SignsDocument1 pageAssessing General Health Status and Vital SignsCyril Joy N. FernandoNo ratings yet
- Activity IntoleranceDocument4 pagesActivity IntoleranceShermane Criszen F. SallanNo ratings yet
- Meniere's Disease - Case StudyDocument3 pagesMeniere's Disease - Case StudyZORANASNNo ratings yet
- Gordon S 11 Functional Health PatternsDocument6 pagesGordon S 11 Functional Health PatternsMrs RehanNo ratings yet
- Movie AnalysisDocument7 pagesMovie Analysisapi-542795774No ratings yet
- Prof Ad Day 1Document136 pagesProf Ad Day 1Kareen ArnaizNo ratings yet
- NCM 100 Case AnaDocument3 pagesNCM 100 Case AnaCharissa Magistrado De LeonNo ratings yet
- CHN ReflectionDocument1 pageCHN ReflectionKen SimonNo ratings yet
- Neuro Vital Signs Assessment Procedure and ChecklistDocument9 pagesNeuro Vital Signs Assessment Procedure and ChecklistJustine BayabosNo ratings yet
- NCM 112 Computation 2021Document3 pagesNCM 112 Computation 2021Marie Kelsey Acena Macaraig100% (1)
- Psych NCPDocument4 pagesPsych NCPnoman-053No ratings yet
- Precede-Proceed Model MyDocument6 pagesPrecede-Proceed Model MyGraciaNo ratings yet
- GitDocument302 pagesGitjgcriste100% (7)
- Nursing Case Analysis-AVFDocument19 pagesNursing Case Analysis-AVFChristopher MaNo ratings yet
- LFD PediaDocument1 pageLFD PediaLadybelle GototosNo ratings yet
- Discharge Plan For CVADocument1 pageDischarge Plan For CVAJeffrey Calicdan BucalaNo ratings yet
- Fdar Psyche 3Document1 pageFdar Psyche 3Aziil LiizaNo ratings yet
- LOG101 Exercise No. 2 - Types of Definitions 20230217091032Document2 pagesLOG101 Exercise No. 2 - Types of Definitions 20230217091032Daniella TimbolNo ratings yet
- Transcultural Nursing TheoryDocument6 pagesTranscultural Nursing TheoryLiiza G-GsprNo ratings yet
- Module 12Document12 pagesModule 12mirai desuNo ratings yet
- Meal Planning For A College Student: Saint Louis University School of NursingDocument7 pagesMeal Planning For A College Student: Saint Louis University School of NursingMaranatha BuenaventuraNo ratings yet
- CHNDocument34 pagesCHNCatherine RomeroNo ratings yet
- Political Caricatures and GrievancesDocument2 pagesPolitical Caricatures and GrievancesAshley BaldivinoNo ratings yet
- Chapter 056Document19 pagesChapter 056Michael SamaniegoNo ratings yet
- Nursing Opportunities AbroadDocument133 pagesNursing Opportunities Abroadrandz c thinksNo ratings yet
- Head Nursing - StudentDocument26 pagesHead Nursing - Studentstepcoy123100% (1)
- NCM 120Document5 pagesNCM 120Tiffany AdriasNo ratings yet
- Cholelithiasis NCP FINALDocument6 pagesCholelithiasis NCP FINALShreshthi VermaNo ratings yet
- Nursing DiagnosisDocument5 pagesNursing DiagnosisGeovanni Rai HermanoNo ratings yet
- Brief Description: Pleural EffusionDocument3 pagesBrief Description: Pleural EffusionJessica CatacutanNo ratings yet
- Cues Nursing Diagnosis Background Knowledge Goal and Objectives Nursing Interventions and Rationale Evaluation Subjective: Noc: NIC: Fluid ManagementDocument10 pagesCues Nursing Diagnosis Background Knowledge Goal and Objectives Nursing Interventions and Rationale Evaluation Subjective: Noc: NIC: Fluid ManagementSkyla FiestaNo ratings yet
- NCP FinalDocument4 pagesNCP FinalKathrina CraveNo ratings yet
- Nursing Care PlanDocument8 pagesNursing Care PlanssucbotNo ratings yet
- Decreased Cardiac OutputDocument5 pagesDecreased Cardiac Outputshuang81No ratings yet
- HernioplastyDocument6 pagesHernioplastyCherry Delos ReyesNo ratings yet
- NCP Con ConstipationDocument2 pagesNCP Con ConstipationChristine Marie Bucio OraizNo ratings yet
- Midpoint Reflection Journal ImmersionDocument3 pagesMidpoint Reflection Journal Immersionapi-433144546No ratings yet
- The Ride of Your Life: What I Learned about God, Love, and Adventure by Teaching My Son to Ride a BikeFrom EverandThe Ride of Your Life: What I Learned about God, Love, and Adventure by Teaching My Son to Ride a BikeRating: 4.5 out of 5 stars4.5/5 (2)
- Ventricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandVentricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- A Simple Guide to Pseudohypoparathyroidism, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Pseudohypoparathyroidism, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Additional Nursing Care Plans - SchizophreniaDocument26 pagesAdditional Nursing Care Plans - SchizophreniaJasmin Jacob100% (5)
- Geography of The BrainDocument1 pageGeography of The BrainmarieNo ratings yet
- Drug Study1Document3 pagesDrug Study1marieNo ratings yet
- Ordinary QuotesDocument1 pageOrdinary QuotesmarieNo ratings yet
- RNHeals AppformDocument1 pageRNHeals AppformmarieNo ratings yet
- MCN Print 3 NotesDocument1 pageMCN Print 3 NotesmarieNo ratings yet
- COPAR PREENTRY PHASE Preliminary Social InvestigationDocument3 pagesCOPAR PREENTRY PHASE Preliminary Social InvestigationmarieNo ratings yet
- Psychia Review Notes (Incmplt)Document3 pagesPsychia Review Notes (Incmplt)marieNo ratings yet
- Nursing Practice 1Document4 pagesNursing Practice 1marieNo ratings yet
- Founder: Categories Christianity Confucianism Buddhism Taoism Islam HinduismDocument3 pagesFounder: Categories Christianity Confucianism Buddhism Taoism Islam HinduismmarieNo ratings yet
- China BrochureDocument2 pagesChina BrochuremarieNo ratings yet
- Nasogastric Tube InsertionDocument3 pagesNasogastric Tube Insertionmarie100% (5)
- Nursing Action Rationale Preparatory PhaseDocument6 pagesNursing Action Rationale Preparatory Phasemarie100% (2)
- 11 Core Competencies Part 1 To Part 2Document4 pages11 Core Competencies Part 1 To Part 2marie100% (2)
- Administering An Enema EQUIPMENT Prepackaged Enema or Enema Container DisposableDocument3 pagesAdministering An Enema EQUIPMENT Prepackaged Enema or Enema Container Disposablemarie100% (2)
- The Aging Society: Its Effects On Health Care DeliveryDocument15 pagesThe Aging Society: Its Effects On Health Care Deliverymarie100% (2)
- Physiology of Aging 2005Document42 pagesPhysiology of Aging 2005marie100% (2)
- Colostomy ProcedureDocument2 pagesColostomy Proceduremarie100% (2)
- Hydronephrosis and OrifDocument2 pagesHydronephrosis and OrifmarieNo ratings yet
- Mechanical Ventilation: EMS Professions Temple CollegeDocument27 pagesMechanical Ventilation: EMS Professions Temple Collegemarie100% (2)
- Nasogastric Tube FeedingDocument6 pagesNasogastric Tube Feedingmarie100% (5)
- TracheostomyDocument1 pageTracheostomymarieNo ratings yet
- FNCP, Rnking and Scaling, Home Visit PlanDocument6 pagesFNCP, Rnking and Scaling, Home Visit Planmarie100% (10)
- Interpersonal Assertiveness: Inside The Balancing Act: Daniel Ames Alice Lee Abbie WazlawekDocument16 pagesInterpersonal Assertiveness: Inside The Balancing Act: Daniel Ames Alice Lee Abbie WazlawekSarah GracyntiaNo ratings yet
- Myra Estrin LevineDocument13 pagesMyra Estrin LevineLALRINTLUANGI CHHAKCHHUAKNo ratings yet
- Sensory ExperienceDocument12 pagesSensory ExperiencePraveen Kumar YadavNo ratings yet
- Edinburgh Research Explorer: Designing Learning Spaces For Children On The Autism SpectrumDocument17 pagesEdinburgh Research Explorer: Designing Learning Spaces For Children On The Autism SpectrumHouwaNo ratings yet
- A Blind Mobility Aid Modeled After Echolocation of Bats: A On in FM A in A Is 70 So As A A inDocument5 pagesA Blind Mobility Aid Modeled After Echolocation of Bats: A On in FM A in A Is 70 So As A A inSagor SahaNo ratings yet
- The Effect of Mediated Music Lessons On The Development of At-Risk Elementary School ChildrenDocument5 pagesThe Effect of Mediated Music Lessons On The Development of At-Risk Elementary School ChildrenKarina LópezNo ratings yet
- Boas - On Alternanting SoundsDocument9 pagesBoas - On Alternanting SoundsVictor Hugo BarretoNo ratings yet
- ORGANIZATIONAL BEHAVIOUR NOTES (MBA)Document19 pagesORGANIZATIONAL BEHAVIOUR NOTES (MBA)JyotiNo ratings yet
- Video Games and Aesthetic Contemplation: Paul Atkinson and Farzad ParsayiDocument19 pagesVideo Games and Aesthetic Contemplation: Paul Atkinson and Farzad ParsayiRecriarseNo ratings yet
- McLellan 2010 Genuine Vs Posed EmotionDocument17 pagesMcLellan 2010 Genuine Vs Posed EmotionMagda ChNo ratings yet
- 13 Areas of Assessment 1 6 RevisedDocument10 pages13 Areas of Assessment 1 6 RevisedSherena NicolasNo ratings yet
- Psychology 20 Chapter 5 True-FalseDocument1 pagePsychology 20 Chapter 5 True-Falseapi-2038142690% (1)
- Psychology ExperimentDocument11 pagesPsychology ExperimentZunair IlyasNo ratings yet
- From The Perspective of PhilosophyDocument11 pagesFrom The Perspective of PhilosophyArgieline FernandezNo ratings yet
- International Conference On Applied Science and HealthDocument6 pagesInternational Conference On Applied Science and HealthRystha BurgaNo ratings yet
- Impact of Teachers' Attitude On Motivation of The StudentsDocument2 pagesImpact of Teachers' Attitude On Motivation of The StudentsiaetsdiaetsdNo ratings yet
- Title: The Perception of Students of Higher Institutions About The Effects of Using Slangs On Their English Language ProficiencyDocument3 pagesTitle: The Perception of Students of Higher Institutions About The Effects of Using Slangs On Their English Language ProficiencyKamilah AznanNo ratings yet
- Lec 5 - VCODocument25 pagesLec 5 - VCOĐỗ Kiều Linh Chi 3TĐ-20ACNNo ratings yet
- Chapter 7 Consumer Learning: Consumer Behavior, 10e (Schiffman/Kanuk)Document34 pagesChapter 7 Consumer Learning: Consumer Behavior, 10e (Schiffman/Kanuk)Valeed Ch100% (1)
- Subliminal Perception and Extrasensory PerceptionDocument19 pagesSubliminal Perception and Extrasensory PerceptionAnne Jenette CastilloNo ratings yet
- On The Mystery of Time by Dr. Raju Chidambaram and Dr. Shobha ChidambaramDocument20 pagesOn The Mystery of Time by Dr. Raju Chidambaram and Dr. Shobha Chidambaramnarayananh100% (2)
- Full Organizational Behavior, 13th Edition (Ebook PDF) Ebook All ChaptersDocument49 pagesFull Organizational Behavior, 13th Edition (Ebook PDF) Ebook All Chaptersqubinahhiggh100% (1)
- Productive, Relational and EverywhereDocument20 pagesProductive, Relational and EverywhereCARLOS ALBERTO MOLINA GOMEZNo ratings yet
- Body, Movement and Dance in PsychotherapyDocument18 pagesBody, Movement and Dance in PsychotherapytaspreNo ratings yet
- Graham Harman - On Vicarious Causation PDFDocument18 pagesGraham Harman - On Vicarious Causation PDFvoyameaNo ratings yet
- Booklet - TOMATIS Method - EngDocument14 pagesBooklet - TOMATIS Method - EngjimmyNo ratings yet
- Taarup Esbensen 2018 Risk AnalysisDocument15 pagesTaarup Esbensen 2018 Risk AnalysisBetrika OktaresaNo ratings yet
- Mpa Thesis SampleDocument8 pagesMpa Thesis Samplefc5wsq30100% (1)