לזכרו של פרופ פוירשטיין
לזכרו של פרופ פוירשטיין
Download as pdf or txt
You might also like
- A Module in Forensic 2Document88 pagesA Module in Forensic 2Cristian Joshua C. SalibongcogonNo ratings yet
- Performance Task in Statistics and ProbabilityDocument4 pagesPerformance Task in Statistics and ProbabilityAnn Gutlay100% (3)
- Introduction To PsychoeducationDocument9 pagesIntroduction To PsychoeducationAneeh100% (1)
- Poster On Lifespan DevelopmentDocument1 pagePoster On Lifespan DevelopmentAntor ShahaNo ratings yet
- Analysis of Pender's Health Promotion Model: Context and Content of The TheoryDocument9 pagesAnalysis of Pender's Health Promotion Model: Context and Content of The TheoryAsih Siti SundariNo ratings yet
- Governmentality: Power and Rule in Modern Society, Second EditionDocument3 pagesGovernmentality: Power and Rule in Modern Society, Second EditionavriqueNo ratings yet
- Dci 2011Document28 pagesDci 2011אמיר סטרנס100% (2)
- PDF 74145 81369Document5 pagesPDF 74145 81369Joel AmetllerNo ratings yet
- SAKELLARI Et Al-2011-Journal of Psychiatric and Mental Health NursingDocument11 pagesSAKELLARI Et Al-2011-Journal of Psychiatric and Mental Health Nursingandreia_afonso_30No ratings yet
- Classwork 3 UNIT 6 Compare & Contrast Essay PART 2Document4 pagesClasswork 3 UNIT 6 Compare & Contrast Essay PART 2Genesis OrellanaNo ratings yet
- PsychoeducationDocument9 pagesPsychoeducationSrinivas Pandeshwar100% (1)
- Personhood of Counsellor in CounsellingDocument9 pagesPersonhood of Counsellor in CounsellingPrerna singhNo ratings yet
- Are Coping Strategies, Emotional Abilities, and Resilience Predictors of Well-Being? Comparison of Linear and Non-Linear MethodologiesDocument13 pagesAre Coping Strategies, Emotional Abilities, and Resilience Predictors of Well-Being? Comparison of Linear and Non-Linear MethodologiesBrittany Caroline BlackNo ratings yet
- SIL ATTITUDE TOWARDS MENTAL HEALTHDocument11 pagesSIL ATTITUDE TOWARDS MENTAL HEALTHvandana28012007No ratings yet
- Vandevelde Morisse Et Al IJDD 2014 - SED-R-with-cover-page-v2Document14 pagesVandevelde Morisse Et Al IJDD 2014 - SED-R-with-cover-page-v2Martina GuzmanNo ratings yet
- Mental Health Status of Student Leaders: Basis For An Enhancement ProgramDocument10 pagesMental Health Status of Student Leaders: Basis For An Enhancement ProgramPsychology and Education: A Multidisciplinary JournalNo ratings yet
- Module-I Introduction & Historical Overview StructureDocument9 pagesModule-I Introduction & Historical Overview StructureAmeena FairozeNo ratings yet
- HLTH 499 Literature ReviewDocument7 pagesHLTH 499 Literature Reviewapi-583311992No ratings yet
- Mental Health and Coping Strategies of Private Secondary School Teachers in The New Normal: Basis For A Psycho-Social Wellbeing Developmental ProgramDocument18 pagesMental Health and Coping Strategies of Private Secondary School Teachers in The New Normal: Basis For A Psycho-Social Wellbeing Developmental ProgramPsychology and Education: A Multidisciplinary JournalNo ratings yet
- Mental HealthDocument11 pagesMental Healthmahmoodosman91No ratings yet
- Metacognitive Reflection and Insight Therapy (Lysakker)Document11 pagesMetacognitive Reflection and Insight Therapy (Lysakker)Cesar BermudezNo ratings yet
- Lesson planDocument25 pagesLesson planNaz Naz BaclidNo ratings yet
- 2021 Sustained, Multifaceted Improvements in Mental Well-Being Following Psychedelic ExperiencesDocument17 pages2021 Sustained, Multifaceted Improvements in Mental Well-Being Following Psychedelic ExperiencesMariana CastañoNo ratings yet
- RRLDocument4 pagesRRLMark CornejoNo ratings yet
- Document_0004-3Document12 pagesDocument_0004-3Bassam AlqadasiNo ratings yet
- LR Meo 2014-2Document10 pagesLR Meo 2014-2api-260733603No ratings yet
- Strengths Against Psychopathology in Adolescents: Ratifying The Robust Bu Emotional IntelligenceDocument13 pagesStrengths Against Psychopathology in Adolescents: Ratifying The Robust Bu Emotional IntelligenceJose Antonio Piqueras RodríguezNo ratings yet
- Chapter 1Document7 pagesChapter 1magtulismikeyvanNo ratings yet
- research-nga-gi-edit-ni-may-ann-karong-december-3-2024Document37 pagesresearch-nga-gi-edit-ni-may-ann-karong-december-3-2024elgen.alarcon01No ratings yet
- Spiritual Intelligence and Well-Being of Caregivers of Neurodevelopmental DisordersDocument10 pagesSpiritual Intelligence and Well-Being of Caregivers of Neurodevelopmental DisordersMarbe HmtNo ratings yet
- 02bfe50d98359a7de3000000 PDFDocument6 pages02bfe50d98359a7de3000000 PDFomkarenatorNo ratings yet
- Ijsret v10 Issue6 558Document5 pagesIjsret v10 Issue6 558Pramit DasNo ratings yet
- Mental Health ContohDocument5 pagesMental Health Contohalicia heraNo ratings yet
- ADHD Meditation 2015Document33 pagesADHD Meditation 2015Marlene LírioNo ratings yet
- 9p - Intellectual Disability and Mental Health - Is Psychology PreparedDocument9 pages9p - Intellectual Disability and Mental Health - Is Psychology Preparedtiagompeixoto.psiNo ratings yet
- Psychology - Selected PapersDocument342 pagesPsychology - Selected Papersrisc0s100% (2)
- Salud Mental Versus Enfermedad Mental: Una Perspectiva de Educación para La SaludDocument4 pagesSalud Mental Versus Enfermedad Mental: Una Perspectiva de Educación para La SaludJuan Rocha DurandNo ratings yet
- An Integrative Approach To Psychotherapy With Special Emphasis On Homeopathic Model.Document12 pagesAn Integrative Approach To Psychotherapy With Special Emphasis On Homeopathic Model.Homoeopathic PulseNo ratings yet
- A Salutogenic Mental Health Model Flourishing As ADocument13 pagesA Salutogenic Mental Health Model Flourishing As AAna EclipseNo ratings yet
- RESEARCHDocument3 pagesRESEARCHOlalia, Sophia Angela M.No ratings yet
- MH 02 PDFDocument11 pagesMH 02 PDFAllain BartolomeNo ratings yet
- Isa BongamDocument5 pagesIsa BongamPhil PendaNo ratings yet
- Ijerph 18 01387Document15 pagesIjerph 18 01387David QatamadzeNo ratings yet
- A Study of A Social-Emotional Learning Program For College Students Integrating MindfulnessDocument7 pagesA Study of A Social-Emotional Learning Program For College Students Integrating MindfulnessAlika Setia PutriNo ratings yet
- Introduction To Mental Health LiteracyDocument23 pagesIntroduction To Mental Health LiteracyWinter sozinyoNo ratings yet
- Essay On Branches of Psychology - Ipshita BagchiDocument11 pagesEssay On Branches of Psychology - Ipshita Bagchiipshita bagchiNo ratings yet
- A Pilot Trial of Mindfulness Meditation Training For AttentionDeficit Hyperactivity Disorder in AdulthoodDocument26 pagesA Pilot Trial of Mindfulness Meditation Training For AttentionDeficit Hyperactivity Disorder in AdulthoodParla CardoNo ratings yet
- Minduflness Entrenamiento Richard DavidsonDocument10 pagesMinduflness Entrenamiento Richard DavidsonElizabethNo ratings yet
- Dissertation Mental Health NursingDocument8 pagesDissertation Mental Health NursingHelpWritingPapersUK100% (2)
- The Model For Sustainable Mental Health Future DirDocument10 pagesThe Model For Sustainable Mental Health Future Dirjmielcarek1No ratings yet
- Learning To BREATHE A Pilot Trial of A MindfulnessDocument12 pagesLearning To BREATHE A Pilot Trial of A Mindfulnessyujiachen2395No ratings yet
- Training in mental health promotionDocument37 pagesTraining in mental health promotionAkhil ChandranNo ratings yet
- Teaching Empathy Through Movies: Reaching Learners' Affective Domain in Medical EducationDocument13 pagesTeaching Empathy Through Movies: Reaching Learners' Affective Domain in Medical EducationSorina NataliaNo ratings yet
- The Influence of Art and Music On Cognitive Function and Mental Health Well Being pr1Document7 pagesThe Influence of Art and Music On Cognitive Function and Mental Health Well Being pr1Patricia CayabyabNo ratings yet
- Psychosocial Interventions DraftDocument12 pagesPsychosocial Interventions DraftDwane PaulsonNo ratings yet
- 1-Article_Text-61-1-10-20210202Document12 pages1-Article_Text-61-1-10-20210202Alvian Rizqi AndrianaNo ratings yet
- Lifespan DevelopemntDocument10 pagesLifespan DevelopemntAntor ShahaNo ratings yet
- Group Intervention For Youth Depression and Anxiety: Outcomes of A Randomized Trial With Adolescents in KenyaDocument33 pagesGroup Intervention For Youth Depression and Anxiety: Outcomes of A Randomized Trial With Adolescents in KenyaTom OsbornNo ratings yet
- Does Mindfulness Meditation Increase EmpathyDocument20 pagesDoes Mindfulness Meditation Increase EmpathyzaezelzsNo ratings yet
- Transpersonal ASSDocument6 pagesTranspersonal ASSheaven shadreckNo ratings yet
- Conferencia Dr. CondonDocument5 pagesConferencia Dr. CondonAlexa Yakeline MenesesNo ratings yet
- Mind Magic: Building a Foundation for Emotional Well-BeingFrom EverandMind Magic: Building a Foundation for Emotional Well-BeingNo ratings yet
- Rapid Core Healing Pathways to Growth and Emotional Healing: Using the Unique Dual Approach of Family Constellations and Emotional Mind Integration for Personal and Systemic Health.From EverandRapid Core Healing Pathways to Growth and Emotional Healing: Using the Unique Dual Approach of Family Constellations and Emotional Mind Integration for Personal and Systemic Health.No ratings yet
- Naomi CV - English, Updated Lan 2018Document24 pagesNaomi CV - English, Updated Lan 2018אמיר סטרנסNo ratings yet
- Naomi CV - English, Updated Lan 2018Document24 pagesNaomi CV - English, Updated Lan 2018אמיר סטרנסNo ratings yet
- 11 TSJPSpecIssueFeuerstein2014 - Noami Hadas Lidor - 219 220Document2 pages11 TSJPSpecIssueFeuerstein2014 - Noami Hadas Lidor - 219 220אמיר סטרנסNo ratings yet
- לזכרו של פרופ פוירשטייןDocument19 pagesלזכרו של פרופ פוירשטייןאמיר סטרנסNo ratings yet
- Dominos SowDocument17 pagesDominos SowSuprotaNo ratings yet
- Guidance On Good Manufacturing PracticeDocument153 pagesGuidance On Good Manufacturing PracticeOanh NguyễnNo ratings yet
- A Comparative Analysis of Online and Traditional Class To The Academic Performance of Selected University StudentsDocument13 pagesA Comparative Analysis of Online and Traditional Class To The Academic Performance of Selected University StudentsasdasdaNo ratings yet
- English4 Q1 DLP Week6 PrefixesDocument4 pagesEnglish4 Q1 DLP Week6 PrefixesTGie OczNo ratings yet
- Admission Into Full and Part Time Postgraduate Programmes For The 20202021 Academic Session - 1601403975Document63 pagesAdmission Into Full and Part Time Postgraduate Programmes For The 20202021 Academic Session - 1601403975dunmiju victoryNo ratings yet
- GSP WeekDocument9 pagesGSP WeekANALYN LANDICHONo ratings yet
- ACI Structural JournalDocument10 pagesACI Structural JournalAbdifatah HassanNo ratings yet
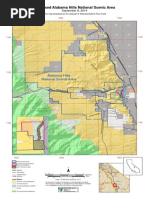
- Alabama Hills Legislation MapDocument1 pageAlabama Hills Legislation MapRep. Paul CookNo ratings yet
- LO 4: Clean Up On Completion of Cropping Work According To Company Standard ProceduresDocument37 pagesLO 4: Clean Up On Completion of Cropping Work According To Company Standard ProceduresRizaLeighFigues100% (2)
- Mandibular Canine IndexDocument5 pagesMandibular Canine Indexyordin deontaNo ratings yet
- AP Chemistry The Origin of Flame ColorsDocument2 pagesAP Chemistry The Origin of Flame ColorsNWong 63604No ratings yet
- Worksheet ADocument3 pagesWorksheet AM Riel Cim AlbancesNo ratings yet
- Bayesian Updating: Probabilistic Prediction Class 12, 18.05 Jeremy Orloff and Jonathan BloomDocument4 pagesBayesian Updating: Probabilistic Prediction Class 12, 18.05 Jeremy Orloff and Jonathan BloomMd CassimNo ratings yet
- The Six Major Subfields of LinguisticsDocument2 pagesThe Six Major Subfields of LinguisticsNoelia NoeliaNo ratings yet
- GAAP Updated Profile 2022Document10 pagesGAAP Updated Profile 2022Som BoyNo ratings yet
- The Tendency of Hotel Rooms Division Managers To Create BudgetaryDocument14 pagesThe Tendency of Hotel Rooms Division Managers To Create BudgetarySolomon ZewduNo ratings yet
- Rilsan Fine Powders Physical PropertiesDocument2 pagesRilsan Fine Powders Physical Propertiesธนาชัย เต็งจิรธนาภาNo ratings yet
- ITMProposers Day2022020v6Document32 pagesITMProposers Day2022020v6熊俊捷No ratings yet
- Tutorial Sheet OneDocument3 pagesTutorial Sheet Onemesho posoNo ratings yet
- HANA Consistency CheckTableConsistency Results 1.00.100+Document8 pagesHANA Consistency CheckTableConsistency Results 1.00.100+Rafael Gonzalez HernándezNo ratings yet
- Additional Mock CAT VARC Test 3Document28 pagesAdditional Mock CAT VARC Test 3mayank palNo ratings yet
- Quantity Surveyor Job in Canterbury Naver Love - SEEKDocument4 pagesQuantity Surveyor Job in Canterbury Naver Love - SEEKKanil RanaweeraNo ratings yet
- Chapter 14 15e Lecture Slide HandoutDocument6 pagesChapter 14 15e Lecture Slide HandoutSamuel Owusu DonkoNo ratings yet
- Algorithms and FlowchartsDocument4 pagesAlgorithms and FlowchartsgeetharjunforeverNo ratings yet
- Depositional Environments Lec. 10 Carbonate Platforms: Dr. Ehab M. Assal Damietta UniversityDocument37 pagesDepositional Environments Lec. 10 Carbonate Platforms: Dr. Ehab M. Assal Damietta UniversityAbram Louies HannaNo ratings yet
- Writing Assessment Criteria: CEFR B2Document3 pagesWriting Assessment Criteria: CEFR B2Cambridge EmpowerNo ratings yet
- ESAF Small Finance BankDocument1 pageESAF Small Finance BankVishwajit GoudNo ratings yet