Nursing Care Plan - Ineffective Airway Clearance
Nursing Care Plan - Ineffective Airway Clearance
Download as doc
At a glance
Powered by AI
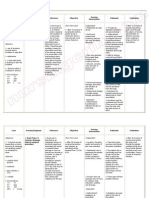
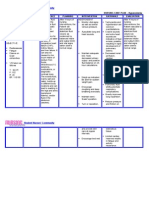
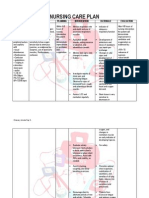
The document describes a nursing care plan for a patient with an ineffective airway clearance. It outlines goals, interventions, and assessments to maintain an open airway and monitor breathing.
The long term goal is for the patient to maintain a patent airway. Short term goals include having clear lung sounds, being free from dyspnea, and demonstrating correct breathing techniques.
Interventions described include assessing the airway for patency, inspecting for potential obstructions, auscultating lung sounds, administering supplemental oxygen, positioning the patient, and assisting with coughing and deep breathing exercises.
You might also like
- Nursing Care Plan - Impaired Gas ExchangeDocument3 pagesNursing Care Plan - Impaired Gas ExchangeYum C86% (65)
- Case Study 1 Mrs. Hogan AsthmaDocument4 pagesCase Study 1 Mrs. Hogan Asthmaissaiahnicolle100% (2)
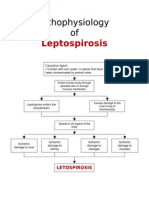
- Physiology of LeptospirosisDocument1 pagePhysiology of LeptospirosisYum C83% (6)
- Nursing Care Plan 6 Impaired Gas ExchangeDocument9 pagesNursing Care Plan 6 Impaired Gas Exchangedbryant0101100% (12)
- Nursing Care Plan For Ineffective Airway ClearanceDocument7 pagesNursing Care Plan For Ineffective Airway Clearancearlee marquez96% (118)
- Nursing Care PlanDocument37 pagesNursing Care Planpia lestrange100% (6)
- Sample SOAPIEDocument1 pageSample SOAPIEYum C100% (1)
- Nutritional Supplements For Muscle MassDocument13 pagesNutritional Supplements For Muscle MassZaagerNo ratings yet
- Impaired Gas ExchangeDocument3 pagesImpaired Gas ExchangeBenedicto RosalNo ratings yet
- Immobility Care Plan For NursesDocument3 pagesImmobility Care Plan For NursesColleen Murray67% (9)
- NCP Ineffective Tissue Perfusion and Self Care DeficitDocument5 pagesNCP Ineffective Tissue Perfusion and Self Care DeficitFrances Anne Pasiliao100% (3)
- Nursing Care PlanDocument10 pagesNursing Care PlanElijah S GomezNo ratings yet
- Nursing Care Plan Ineffective Airway ClearanceDocument3 pagesNursing Care Plan Ineffective Airway Clearancederic100% (13)
- NCP Impaired Gas ExchangeDocument4 pagesNCP Impaired Gas ExchangeKen Simon100% (1)
- NCP Impaired Gas ExchangeDocument1 pageNCP Impaired Gas ExchangeLaidy Aizahlyn Indoc Angod0% (3)
- Pneumonia-Ineffective Airway ClearanceDocument2 pagesPneumonia-Ineffective Airway ClearanceNursesLabs.com86% (7)
- Impaired Urinary EliminationDocument2 pagesImpaired Urinary EliminationHaon Anasu67% (3)
- Endorsement SheetDocument1 pageEndorsement Sheeteihjay-bravo-8041100% (1)
- Plan of ActivitiesDocument1 pagePlan of ActivitiesYum CNo ratings yet
- DRUGSTUDY: Dolfenal - Mefenamic AcidDocument2 pagesDRUGSTUDY: Dolfenal - Mefenamic AcidYum CNo ratings yet
- Long-Life Asphalt Pavements - Technical2007Document24 pagesLong-Life Asphalt Pavements - Technical2007Sen Hu100% (1)
- Final NCP Ineffective Airway ClearanceDocument8 pagesFinal NCP Ineffective Airway ClearanceHazel EndayaNo ratings yet
- NCP Difficulty of Breathing R/T SecretionDocument3 pagesNCP Difficulty of Breathing R/T Secretionherscentasiascribd50% (8)
- Pneumonia NCPDocument7 pagesPneumonia NCPitsmeaya100% (3)
- Nursing Care PlanDocument4 pagesNursing Care PlanAdreanah Martin RañisesNo ratings yet
- Risk For Ineffective Tissue PerfusionDocument5 pagesRisk For Ineffective Tissue PerfusionElle Oranza100% (1)
- NCP - Impaired Gas ExchangeDocument1 pageNCP - Impaired Gas ExchangeRryje Salleva100% (1)
- NCP Ineffective Airway ClearanceDocument1 pageNCP Ineffective Airway ClearanceImation DataNo ratings yet
- Nursing Care Plan - Acute PainDocument1 pageNursing Care Plan - Acute PainLei Ortega100% (6)
- Hypervolemia NCPDocument2 pagesHypervolemia NCPAlroi Abrantes50% (2)
- Nursing Care Plan: Cystic FibrosisDocument4 pagesNursing Care Plan: Cystic FibrosisYael EzraNo ratings yet
- Impaired Gas ExchangeDocument22 pagesImpaired Gas ExchangecheenapberberNo ratings yet
- Ineffective Breathing PatternDocument5 pagesIneffective Breathing PatternruguNo ratings yet
- Asthma Impaired Gas ExchangeDocument2 pagesAsthma Impaired Gas ExchangeNedeve Ozned100% (5)
- Ineffective Tissue PerfusionDocument2 pagesIneffective Tissue PerfusionClaidelyn De Leyola100% (1)
- NCP Inffective Tissue PerfusionDocument3 pagesNCP Inffective Tissue PerfusionPaul Cubacub0% (1)
- Nursing Care Plan For Ineffective Airway ClearanceDocument3 pagesNursing Care Plan For Ineffective Airway ClearanceRodel Yacas67% (3)
- Cues Nursing Diagnosis Scientific Rationale Goals Nursing Interventions Rationale EvaluationDocument3 pagesCues Nursing Diagnosis Scientific Rationale Goals Nursing Interventions Rationale EvaluationIngrid Nicolas100% (1)
- FocusDocument15 pagesFocusSergio Rivas100% (3)
- NCP - CopdDocument3 pagesNCP - CopdhystericoNo ratings yet
- NCPDocument9 pagesNCPTracy Camille EscobarNo ratings yet
- Teaching Plan For Adult PneumoniaDocument5 pagesTeaching Plan For Adult PneumoniaAldrin Maer100% (2)
- Risk For AspirationDocument3 pagesRisk For Aspirationcotyboy0% (2)
- NCPDocument2 pagesNCPDidith AbanNo ratings yet
- NCP-Impaired Physical MobilityDocument3 pagesNCP-Impaired Physical MobilityradarsoulNo ratings yet
- Ncp-Impaired Gas ExchangeDocument2 pagesNcp-Impaired Gas ExchangeSJ Abunda0% (1)
- Nursing Care Plan Risk For Skin BreakdownDocument3 pagesNursing Care Plan Risk For Skin BreakdownShelli Miller Pryor82% (11)
- Risk For InfectionDocument18 pagesRisk For InfectionValiant Baybay0% (1)
- Nursing Care Plan: References: Nurse's Pocket Guide Pages 151-155Document1 pageNursing Care Plan: References: Nurse's Pocket Guide Pages 151-155Caroline ChaNo ratings yet
- ND - Risk For SuicideDocument3 pagesND - Risk For SuicideHu Dawi100% (2)
- NCP Sleep DisturbanceDocument1 pageNCP Sleep DisturbanceKrystel Cate DelaCruz DamianNo ratings yet
- Impaired Gas ExchangeDocument5 pagesImpaired Gas ExchangeKM67% (3)
- Activity Intolerance Care PlanDocument4 pagesActivity Intolerance Care Planapi-315890029No ratings yet
- NCP - CapDocument4 pagesNCP - CapSherryNo ratings yet
- Impaired Gas ExchangeDocument2 pagesImpaired Gas ExchangeHanya Bint PotawanNo ratings yet
- Activity Intolerance (NCP)Document3 pagesActivity Intolerance (NCP)Sonia Letran Singson100% (3)
- NCP Fdar Fin.Document8 pagesNCP Fdar Fin.Bissette DomingoNo ratings yet
- Nursing DiagnosisDocument4 pagesNursing DiagnosisKrizzia CarlosNo ratings yet
- Nursing Care PlanDocument22 pagesNursing Care PlanjamNo ratings yet
- Nursing Care PlanDocument14 pagesNursing Care PlanVin Landicho100% (1)
- Ineffective Airway Clearance R/T Tracheobronchial ObstructionDocument23 pagesIneffective Airway Clearance R/T Tracheobronchial ObstructionGuia Rose SibayanNo ratings yet
- Case Study Nursing Diagnosis of PneumothoraxDocument8 pagesCase Study Nursing Diagnosis of PneumothoraxJansen Arquilita RiveraNo ratings yet
- Rapid Sequence Intubation ReportDocument55 pagesRapid Sequence Intubation Reportlorkan19100% (1)
- Chest TraumaDocument14 pagesChest TraumaMary Rose BatagaNo ratings yet
- Endotracheal TubeDocument19 pagesEndotracheal TubeSarvess Muniandy100% (1)
- PALS Guidelines For HypotensionDocument19 pagesPALS Guidelines For HypotensionAnil SharmaNo ratings yet
- Lung Cancer: Midterm BSN Iv - BDocument6 pagesLung Cancer: Midterm BSN Iv - BYum CNo ratings yet
- Reported By:: Castrillo, Mariam P. BSN Iv - B Group 4Document17 pagesReported By:: Castrillo, Mariam P. BSN Iv - B Group 4Yum CNo ratings yet
- Schedule For Nurses SampleDocument1 pageSchedule For Nurses SampleYum CNo ratings yet
- Peritoneal DialysisDocument45 pagesPeritoneal DialysisYum CNo ratings yet
- Nursing Management Process and FunctionsDocument151 pagesNursing Management Process and FunctionsYum CNo ratings yet
- Leadership and ManagementDocument216 pagesLeadership and ManagementYum C75% (4)
- Paracetamol (Aeknil), Metoclopramide (Plasil), Cotrimoxazole Susp. (Macromed), PedialyteDocument4 pagesParacetamol (Aeknil), Metoclopramide (Plasil), Cotrimoxazole Susp. (Macromed), PedialyteYum C100% (2)
- Urinary System: Anatomy and PhysiologyDocument42 pagesUrinary System: Anatomy and PhysiologyYum C100% (3)
- Leukemia Cells & ColorectalDocument40 pagesLeukemia Cells & ColorectalYum CNo ratings yet
- Sample Laboratory ResultsDocument1 pageSample Laboratory ResultsYum CNo ratings yet
- "Cholera": Uph-Djgtmu College of NursingDocument26 pages"Cholera": Uph-Djgtmu College of NursingYum C100% (1)
- MeaslesDocument32 pagesMeaslesYum C100% (2)
- Pathophysiology of AGEDocument1 pagePathophysiology of AGEYum CNo ratings yet
- DRUG STUDY: Metoprolol - BetalocDocument1 pageDRUG STUDY: Metoprolol - BetalocYum C100% (1)
- DRUG STUDY: Rocephin - Ceftriaxone SodiumDocument1 pageDRUG STUDY: Rocephin - Ceftriaxone SodiumYum C100% (1)
- Breast Mass Bilateral To Consider FibroadenomaDocument5 pagesBreast Mass Bilateral To Consider FibroadenomaYum CNo ratings yet
- DRUG STUDY: Bactidol - HexetidineDocument2 pagesDRUG STUDY: Bactidol - HexetidineYum CNo ratings yet
- DRUG STUDY: Fenofibrate - TricorDocument2 pagesDRUG STUDY: Fenofibrate - TricorYum CNo ratings yet
- DRUG STUDY: Biogesic - ParacetamolDocument1 pageDRUG STUDY: Biogesic - ParacetamolYum C100% (1)
- Breast MassDocument3 pagesBreast MassYum CNo ratings yet
- Lesson Plan (Sample)Document2 pagesLesson Plan (Sample)Yum C100% (4)
- WT198CDocument2 pagesWT198CaaquilNo ratings yet
- Course Caterpillar c6 6 Engines Acert Technology BenefitsDocument34 pagesCourse Caterpillar c6 6 Engines Acert Technology BenefitsGanapati Hegde100% (10)
- Standard Costing and Variance Analysis FormulasDocument2 pagesStandard Costing and Variance Analysis FormulasAnuraag GuptaaNo ratings yet
- An Example of Outstanding Rubens Forgery-1Document7 pagesAn Example of Outstanding Rubens Forgery-1Stephanie Two-TwoNo ratings yet
- A Handbook of CosmeticsDocument134 pagesA Handbook of CosmeticsAlifa Syafira Putri76% (25)
- CE CGR: This Datasheet Has Been Downloaded From at ThisDocument7 pagesCE CGR: This Datasheet Has Been Downloaded From at ThisFarooq AhmedNo ratings yet
- AlvinT Price List 2016 - IDR - Okt2016 PDFDocument5 pagesAlvinT Price List 2016 - IDR - Okt2016 PDFDavid Epson Mayer0% (1)
- Rubin William S Dada Surrealism and Their Heritage 1968 PDFDocument256 pagesRubin William S Dada Surrealism and Their Heritage 1968 PDFFaHflores100% (2)
- Supplier Quality ManualDocument32 pagesSupplier Quality ManualEliane CostaNo ratings yet
- Animal Totem MeditationDocument6 pagesAnimal Totem MeditationBalajiNo ratings yet
- Nama: Raihan Valentino Jaya Saputra NIM: 5111418055Document8 pagesNama: Raihan Valentino Jaya Saputra NIM: 5111418055JamesNo ratings yet
- Acceptance Check ListDocument2 pagesAcceptance Check ListMohamed HamdyNo ratings yet
- Gas Tungsten Arc WeldingDocument15 pagesGas Tungsten Arc Weldingsushant47No ratings yet
- LRFD Compression Member DesignDocument236 pagesLRFD Compression Member DesignWayne Alegria JumawanNo ratings yet
- 129 Poojasharma 190-195Document6 pages129 Poojasharma 190-195Nitesh kumarNo ratings yet
- Classified: Your Local MarketplaceDocument3 pagesClassified: Your Local MarketplaceDigital MediaNo ratings yet
- Reading For Supporting Irrelevant Details PDFDocument9 pagesReading For Supporting Irrelevant Details PDFashmita 260199No ratings yet
- 5 - Trichomonas VaginalisDocument16 pages5 - Trichomonas Vaginalisعبد الرحمن حامدNo ratings yet
- MATOUWANG-Publication and Routing ChartDocument6 pagesMATOUWANG-Publication and Routing Charttharindu hasarangaNo ratings yet
- Simulation and Visualisation Workshop FlyerDocument2 pagesSimulation and Visualisation Workshop Flyerالمهندس زاهر بكريNo ratings yet
- Benling India Energy and Technology Pvt. Ltd.Document1 pageBenling India Energy and Technology Pvt. Ltd.akshatsaini640No ratings yet
- TDTS06 Computer NetworksDocument7 pagesTDTS06 Computer NetworksShalu TutejaNo ratings yet
- Bosch Motronic Basic Motronic 1.1 1.2 1Document53 pagesBosch Motronic Basic Motronic 1.1 1.2 1Danniel PizattoNo ratings yet
- A Comprehensive Carbon Footprint Analysis of Different Wastewater Treatment Plant ConfigurationspdfDocument11 pagesA Comprehensive Carbon Footprint Analysis of Different Wastewater Treatment Plant ConfigurationspdfgbenincaNo ratings yet
- Annex A Wood Specifications & Accepted Crack DetailsDocument2 pagesAnnex A Wood Specifications & Accepted Crack DetailsAbdullahNo ratings yet
- Annual APCG Flea Market A Success!: Bay ErosionDocument4 pagesAnnual APCG Flea Market A Success!: Bay Erosionjhartmann13No ratings yet
- Occupied BedDocument2 pagesOccupied BedZJ GarcianoNo ratings yet
- Compiled AssistantshipsDocument15 pagesCompiled AssistantshipsROBI PAULNo ratings yet