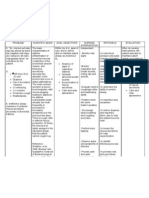
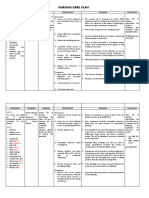
NCP Proper
NCP Proper
Download as docx, pdf, or txt
You might also like
- Claire P. Thomas - Home Body Guide PDFDocument94 pagesClaire P. Thomas - Home Body Guide PDFstuartedmondson100% (4)
- NCP For HemothoraxDocument12 pagesNCP For Hemothoraxroseonabreeze0% (1)
- TONSILITIS AND ADENOIDITIS - Baldoza.E.Document9 pagesTONSILITIS AND ADENOIDITIS - Baldoza.E.Monette Abalos MendovaNo ratings yet
- Ineffective Breathing PatternDocument3 pagesIneffective Breathing PatternReichelle Perlas64% (14)
- Suffixes: Adjective, Noun, Diminutive, Singular, Plural: Medical TerminologyDocument8 pagesSuffixes: Adjective, Noun, Diminutive, Singular, Plural: Medical Terminologystephanie eduarteNo ratings yet
- Pathophysiology CVADocument2 pagesPathophysiology CVASewyel Garburi100% (6)
- Data Ebook Antiage Ebook v1 2621 enDocument101 pagesData Ebook Antiage Ebook v1 2621 enAngel Luis Ortega ArevaloNo ratings yet
- Brain Health GuideDocument50 pagesBrain Health GuideLuis Alfonso Caravedo Cánepa100% (4)
- NCP Ineffective Airway Clearance For PneumoniaDocument5 pagesNCP Ineffective Airway Clearance For PneumoniaKullin Rain100% (1)
- Nursing Care Plan Proper CapcDocument4 pagesNursing Care Plan Proper CapcKit LaraNo ratings yet
- Ineffective Airway ClearanceDocument1 pageIneffective Airway ClearancejomerdalonaNo ratings yet
- Final NCPDocument13 pagesFinal NCPBAGUIO CATSNo ratings yet
- NCPDocument7 pagesNCPRuth MontebonNo ratings yet
- PRIORITY 2: Impaired Gas Exchange Related To Excessive or Thick Secretions Tree Secondary To PneumoniaDocument4 pagesPRIORITY 2: Impaired Gas Exchange Related To Excessive or Thick Secretions Tree Secondary To PneumoniaElay Pedroso100% (1)
- Impaired Gas Exchange NCPDocument4 pagesImpaired Gas Exchange NCPkimglaidyl bontuyanNo ratings yet
- Cues Nursing Diagnosis Inference Planning Nursing Intervention Rationale EvaluationDocument3 pagesCues Nursing Diagnosis Inference Planning Nursing Intervention Rationale EvaluationNichol John MalabananNo ratings yet
- Nursing Care Plan AnemiaDocument3 pagesNursing Care Plan AnemiaNat B. AntipoloNo ratings yet
- Scenario 4 - NCPDocument15 pagesScenario 4 - NCPVian RiveraNo ratings yet
- NCP-Drug Study 2Document4 pagesNCP-Drug Study 2hsiriaNo ratings yet
- NCM 112 LEC Topic 2 Oxygenation Current Health History Physical Examination Normal Abnormal Breath Sounds Breathing PatternsDocument7 pagesNCM 112 LEC Topic 2 Oxygenation Current Health History Physical Examination Normal Abnormal Breath Sounds Breathing PatternsViviene Faye FombuenaNo ratings yet
- Assessment Nursing Diagnosis Scientific Rationale Planning Nursing Interventions Rationale EvaluationDocument3 pagesAssessment Nursing Diagnosis Scientific Rationale Planning Nursing Interventions Rationale EvaluationMel Izhra N. MargateNo ratings yet
- NCP - ANAPHYLACTIC SHOCK..2pdfDocument6 pagesNCP - ANAPHYLACTIC SHOCK..2pdfLycah RotoneNo ratings yet
- NCP Ineffective Airway Clearance PediaDocument2 pagesNCP Ineffective Airway Clearance PediaFaith CalimlimNo ratings yet
- New Update 35 Laryngospasm PDFDocument4 pagesNew Update 35 Laryngospasm PDFRobertaNo ratings yet
- Nueva Ecija University of Science and Technology: Case 7Document7 pagesNueva Ecija University of Science and Technology: Case 7jomariNo ratings yet
- NCP, Drug StudyDocument9 pagesNCP, Drug StudyTresha CaliboNo ratings yet
- MCN NCPDocument4 pagesMCN NCPPEARL CHRISTINE CUDALNo ratings yet
- 1 Impaired Gas ExchangeDocument11 pages1 Impaired Gas ExchangeKristian Dave DivaNo ratings yet
- IPPA SampleDocument28 pagesIPPA Samplekimglaidyl bontuyanNo ratings yet
- NCP - AnthraxDocument3 pagesNCP - AnthraxbangtankklimbingclanNo ratings yet
- NCP FinalDocument16 pagesNCP FinalEuleen Tria PadrigoNo ratings yet
- NCP KoDocument1 pageNCP Kojiellianemae100% (1)
- Nursing Care Plan: Cues Analysis Nursing Diagnosis Goal and Objectives Intervention Rationale Evaluation SubjectiveDocument6 pagesNursing Care Plan: Cues Analysis Nursing Diagnosis Goal and Objectives Intervention Rationale Evaluation SubjectiveKristel PunoNo ratings yet
- Ncp-Ineffective Airway ClearanceDocument3 pagesNcp-Ineffective Airway Clearancelouanne0550% (2)
- Ineffective Airway Clearance - PTBDocument2 pagesIneffective Airway Clearance - PTBIrish Eunice FelixNo ratings yet
- Keperawatan Dasar 1 - Kebutuhan OksigenDocument11 pagesKeperawatan Dasar 1 - Kebutuhan OksigenMaulidya AyumiNo ratings yet
- Elena Ocyo (Pedia - NCP)Document3 pagesElena Ocyo (Pedia - NCP)elle leliNo ratings yet
- Nursing Care Plan Ineffective Airway Clearance Related To Tracheobronchial Secretions CAPDocument2 pagesNursing Care Plan Ineffective Airway Clearance Related To Tracheobronchial Secretions CAPLP Benoza100% (2)
- Bronchial Asthma (Parinas Rhoanne)Document10 pagesBronchial Asthma (Parinas Rhoanne)Carlojay IniegoNo ratings yet
- OXYGINATION FUNDA LEC BebeDocument8 pagesOXYGINATION FUNDA LEC BebediarosedoloresbsncNo ratings yet
- Thoracic and Lung Assessment: College of Nursing and Allied Health Sciences Maasin City, Southern LeyteDocument4 pagesThoracic and Lung Assessment: College of Nursing and Allied Health Sciences Maasin City, Southern LeytePrincess Diana Jean ModesteNo ratings yet
- Wong - NCP Pneumonia RedoDocument5 pagesWong - NCP Pneumonia RedoLecery Sophia WongNo ratings yet
- Kez NCPDocument12 pagesKez NCPShizuka Marycris AmaneNo ratings yet
- Nursing Intervention Respiratory Status: Ventilation Respiratory Status: Airway Patency Vital Sign StatusDocument12 pagesNursing Intervention Respiratory Status: Ventilation Respiratory Status: Airway Patency Vital Sign StatusSepti MemorisaNo ratings yet
- Nursing Diagnosis For AsthmaDocument6 pagesNursing Diagnosis For AsthmaJulia MendiolaNo ratings yet
- Ineffective Breathing Pattern - NCPDocument2 pagesIneffective Breathing Pattern - NCPHsintan HsuNo ratings yet
- NCP Difficulties in BreathingDocument4 pagesNCP Difficulties in BreathingKingJayson Pacman06No ratings yet
- AssessmentDocument1 pageAssessmentFat NrqzNo ratings yet
- Nursing Care Plan: Congestive Heart Failure-Deep Vein ThrombosisDocument19 pagesNursing Care Plan: Congestive Heart Failure-Deep Vein ThrombosisRiza Angela BarazanNo ratings yet
- Pathophysiology of Empty Nose Syndrome: Contemporary ReviewDocument5 pagesPathophysiology of Empty Nose Syndrome: Contemporary ReviewTheodore LiwonganNo ratings yet
- Pulmonary Tuberculosis G3Document12 pagesPulmonary Tuberculosis G3Cuttie Anne GalangNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument4 pagesAssessment Diagnosis Planning Intervention Rationale EvaluationTrisha Suazo100% (1)
- A Case Study of Bronchial Asthma in Acute Exacerbation (Baiae)Document10 pagesA Case Study of Bronchial Asthma in Acute Exacerbation (Baiae)Janina RojoNo ratings yet
- Cues Diagnosi S Desired Outcome Interventions Rationale EvaluationDocument2 pagesCues Diagnosi S Desired Outcome Interventions Rationale EvaluationYamete KudasaiNo ratings yet
- Pom MTDocument14 pagesPom MTRianne MagalongaNo ratings yet
- Snoring, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandSnoring, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Modern Anaesthesia:: A Concise Guide to the Study and Practice of Anaesthesia.From EverandModern Anaesthesia:: A Concise Guide to the Study and Practice of Anaesthesia.No ratings yet
- A Simple Guide to the Nose and Its Disorders, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to the Nose and Its Disorders, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Your Family Doctor Asthma: Understanding Asthma / Avoiding Allergies / Proper Use of InhalersFrom EverandYour Family Doctor Asthma: Understanding Asthma / Avoiding Allergies / Proper Use of InhalersNo ratings yet
- Barosinusitis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandBarosinusitis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Course On The Crisis of Capitalism and Why The Global Economy Is Teetering On The Verge of CollapseDocument3 pagesCourse On The Crisis of Capitalism and Why The Global Economy Is Teetering On The Verge of Collapsestephanie eduarteNo ratings yet
- Wedding DanceDocument2 pagesWedding Dancestephanie eduarte100% (4)
- No Pardon For MeDocument3 pagesNo Pardon For Mestephanie eduarte67% (3)
- Laudato Si SummaryDocument10 pagesLaudato Si Summarystephanie eduarteNo ratings yet
- NCP ProperDocument9 pagesNCP Properstephanie eduarteNo ratings yet
- ContentServer AspDocument8 pagesContentServer Aspstephanie eduarteNo ratings yet
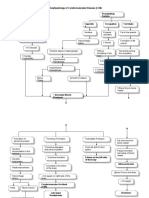
- Diagram PathophysiologyDocument1 pageDiagram Pathophysiologystephanie eduarteNo ratings yet
- Centesis - Ectomy - Lysis - Pexy - Plasty - Rrhaphy - SDocument2 pagesCentesis - Ectomy - Lysis - Pexy - Plasty - Rrhaphy - Sstephanie eduarteNo ratings yet
- Diagram PathophysiologyDocument1 pageDiagram Pathophysiologystephanie eduarteNo ratings yet
- Health & Safety Policy HSPol003 Feb2013Rev FinalDocument11 pagesHealth & Safety Policy HSPol003 Feb2013Rev FinalRajendraNo ratings yet
- Dialog 2 WWDocument4 pagesDialog 2 WWILHAM FERDIANSAHNo ratings yet
- LayoutDocument1 pageLayoutNina OaipNo ratings yet
- Treatment Resistant OcdDocument70 pagesTreatment Resistant Ocddrkadiyala2100% (1)
- Visual Impairment and BlindnessDocument4 pagesVisual Impairment and Blindnessapi-242024640No ratings yet
- The DSM Diagnostic Criteria For Female Sexual Arousal DisorderDocument16 pagesThe DSM Diagnostic Criteria For Female Sexual Arousal DisorderLucia TarhonNo ratings yet
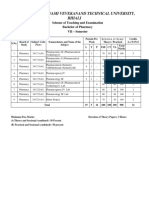
- 7th Sem BPharmaDocument11 pages7th Sem BPharmamanurajguNo ratings yet
- Chapter 41: The Child With An Infectious Disease Test Bank: Multiple ChoiceDocument10 pagesChapter 41: The Child With An Infectious Disease Test Bank: Multiple ChoiceNurse UtopiaNo ratings yet
- Fracture Nursing Care PlansDocument14 pagesFracture Nursing Care PlansSheryl Ann Barit PedinesNo ratings yet
- Accident Incident Reporting Procedure 1719013603Document26 pagesAccident Incident Reporting Procedure 1719013603mata manuelNo ratings yet
- Jo Roby Statement of HarmDocument13 pagesJo Roby Statement of HarmMichael_Lee_RobertsNo ratings yet
- Syndromic Notification and Laboratory Investigation Manual: MOH / K / EPI / 38.04 (HB)Document63 pagesSyndromic Notification and Laboratory Investigation Manual: MOH / K / EPI / 38.04 (HB)Kyaw Han Thar MyintNo ratings yet
- Jurnal 3Document13 pagesJurnal 3Santi SantideswitaNo ratings yet
- TESDA Circular No. 051-2019 PDFDocument60 pagesTESDA Circular No. 051-2019 PDFebc07No ratings yet
- Piling Larang ModuleDocument4 pagesPiling Larang Moduleleslie sabateNo ratings yet
- Personal Hygiene in Food Production - DowloadDocument30 pagesPersonal Hygiene in Food Production - Dowloadanish_habiba80% (10)
- Thesis Hospital DesignDocument4 pagesThesis Hospital Designgbv7kahm100% (2)
- P. Inorganic Chemistry Lab ManualDocument45 pagesP. Inorganic Chemistry Lab ManualDean PharmacyNo ratings yet
- Week 7 Sensing Connecting and EngagingDocument64 pagesWeek 7 Sensing Connecting and Engagingvickytang22072002No ratings yet
- Samberigi Water ProjectDocument3 pagesSamberigi Water Projectmax kende100% (1)
- Safety For Business Travel PolicyDocument14 pagesSafety For Business Travel PolicyZaitoon NadeemNo ratings yet
- Final Draft MTDP 2014-2017 LanmmaDocument269 pagesFinal Draft MTDP 2014-2017 LanmmaKwasi AdarkwaNo ratings yet
- OrifDocument2 pagesOrifGene Edward D. ReyesNo ratings yet
- Cagayan State University: Unit 1 Topic 3. Understanding Principles of Training Lesson ObjectivesDocument9 pagesCagayan State University: Unit 1 Topic 3. Understanding Principles of Training Lesson ObjectivesRichee LunnayNo ratings yet
- ID Gambaran Perilaku Tenaga Kesehatan Terhadap Pelayanan Prima Di Puskesmas TomuanDocument9 pagesID Gambaran Perilaku Tenaga Kesehatan Terhadap Pelayanan Prima Di Puskesmas TomuannovallNo ratings yet
- Patient Joseph Alvarez: Not Yet Answered Marked Out of 12.00Document8 pagesPatient Joseph Alvarez: Not Yet Answered Marked Out of 12.00jyka100% (1)
- Um 209 Benchmarking Learning Activity On Learning Continuity and Recovery Plan (LCRP) & Looping Strategy in TeachingDocument2 pagesUm 209 Benchmarking Learning Activity On Learning Continuity and Recovery Plan (LCRP) & Looping Strategy in TeachingHarline AbanNo ratings yet