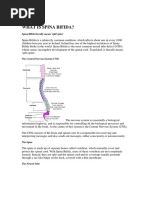
Spina bifida is a birth defect where the spine and spinal cord do not develop properly, leaving an opening where the spinal cord and membranes can protrude. It ranges in severity from spina bifida occulta, where there is a small gap in vertebrae often without symptoms, to myelomeningocele where the most severe form where the spinal cord and membranes protrude through the open spine. Risk factors include folate deficiency, family history, some medications, diabetes, obesity, and fever during early pregnancy. Diagnosis may involve ultrasounds, MRI, and tests of amniotic fluid. Treatment is usually early surgery to close the opening and address any complications.
Spina bifida is a birth defect where the spine and spinal cord do not develop properly, leaving an opening where the spinal cord and membranes can protrude. It ranges in severity from spina bifida occulta, where there is a small gap in vertebrae often without symptoms, to myelomeningocele where the most severe form where the spinal cord and membranes protrude through the open spine. Risk factors include folate deficiency, family history, some medications, diabetes, obesity, and fever during early pregnancy. Diagnosis may involve ultrasounds, MRI, and tests of amniotic fluid. Treatment is usually early surgery to close the opening and address any complications.
Spina bifida is a birth defect where the spine and spinal cord do not develop properly, leaving an opening where the spinal cord and membranes can protrude. It ranges in severity from spina bifida occulta, where there is a small gap in vertebrae often without symptoms, to myelomeningocele where the most severe form where the spinal cord and membranes protrude through the open spine. Risk factors include folate deficiency, family history, some medications, diabetes, obesity, and fever during early pregnancy. Diagnosis may involve ultrasounds, MRI, and tests of amniotic fluid. Treatment is usually early surgery to close the opening and address any complications.
Spina bifida is a birth defect where the spine and spinal cord do not develop properly, leaving an opening where the spinal cord and membranes can protrude. It ranges in severity from spina bifida occulta, where there is a small gap in vertebrae often without symptoms, to myelomeningocele where the most severe form where the spinal cord and membranes protrude through the open spine. Risk factors include folate deficiency, family history, some medications, diabetes, obesity, and fever during early pregnancy. Diagnosis may involve ultrasounds, MRI, and tests of amniotic fluid. Treatment is usually early surgery to close the opening and address any complications.
Download as DOCX, PDF, TXT or read online from Scribd
Download as docx, pdf, or txt
You are on page 1/ 17
SPINA BIFIDA
INTRODUCTION
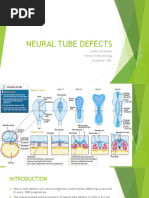
Spina bifida is a birth defect that occurs when the spine and spinal cord don't form properly. It falls under the broader category of neural tube defects. It is part of a group of birth defects called neural tube defects caused by a defect in the neural arch generally in the lumbosacral region, spina bifida is a failure of the posterior laminae of the vertebrae to close; this leaves an opening through which the spinal meninges and spinal cord may protrude The neural tube is the embryonic structure that eventually develops into the baby's brain and spinal cord and the tissues that enclose them. Normally, the neural tube forms early in pregnancy, and it closes by the 28th day after conception. In babies with spina bifida, a portion of the neural tube fails to develop or close properly, causing defects in the spinal cord and in the bones of the spine. Spina bifida can range from mild to severe, depending on the type of defect, size, location and complications. When early treatment for spina bifida is necessary, it's done surgically, although such treatment doesn't always completely resolve the problem.
DEFINITION
Spina bifida is a congenital defect of the spine in which part of the
spinal cord and its meninges are exposed through a gap in the backbone. It often causes paralysis of the lower limbs, and sometimes learning difficulties.
INCIDENCE The rate of myelomeningocele and other neural tube defects has declined since the late 20th century. The average worldwide incidence of spina bifida is 1 case per 1000 births, but marked geographic variations occur. According to the CDC, the prevalence of spina bifida in the United States is higher in the white and Hispanic populations (2 and 1.96, respectively, per 10, 000 live births) than in the black population (1.74 per 10, 000 live births).Data from state and national surveillance systems from 1983-1990 found the birth prevalence rate of myelomeningocele to be slightly higher in females than in males (1.2:1).
RISK FACTORS
Spina bifida is more common among whites and Hispanics, and females are affected more often than males. Although doctors and researchers don't know for sure why spina bifida occurs, they have identified some risk factors:
1.Folate deficiency.
Folate (vitamin B-9) is important to the healthy development of a
baby. Folate is the natural form of vitamin B-9. The synthetic form, found in supplements and fortified foods, is called folic acid. A folate deficiency increases the risk of spina bifida and other neural tube defects.
2.Family history of neural tube defects.
Couples who've had one child with a neural tube defect have a slightly higher chance of having another baby with the same defect. That risk increases if two previous children have been affected by the condition. In addition, a woman who was born with a neural tube defect has a greater chance of giving birth to a child with spina bifida. However, most babies with spina bifida are born to parents with no known family history of the condition.
3.Some medications. For example, anti-seizure medications, such as valproic acid seem to cause neural tube defects when taken during pregnancy, possibly because they interfere with the body's ability to use folate and folic acid.
4.Diabetes.
Women with diabetes who don't control their blood sugar well have a higher risk of having a baby with spina bifida.
5.Obesity.
Pre-pregnancy obesity is associated with an increased risk of neural
tube birth defects, including spina bifida.
6.Increased body temperature.
Some evidence suggests that increased body temperature
(hyperthermia) in the early weeks of pregnancy may increase the risk of spina bifida. Elevating your core body temperature, due to fever or the use of saunas or hot tubs, has been associated with a possible slight increased risk of spina bifida.
TYPES
Spina bifida can occur in different forms: spina bifida occulta,
meningocele or myelomeningocele. The severity of spina bifida depends on the type, size, location and complications.
1. Spina bifida occulta
"Occulta" means hidden. The mildest form, spina bifida occulta results in a small separation or gap in one or more of the bones of the spine (vertebrae). Many people who have spina bifida occulta don't even know it, unless the condition is discovered during an imaging test done for unrelated reasons. It is a defect which results from failure of formation of bony arch around the spinal cord, but spinal cord and meninges are normal. It is not visible externally and is asymptomatic. This type of defects occurs in 5% cases of spina
2.Spina bifida cystica
Spina bifida cystica is a defect in the closure of posterior vertebral
arch with protrusion of spinal cord and meninges through the defect.
a. Meningocele
In a form of spina bifida called meningocele, the protective membranes
around the spinal cord (meninges) push out through the opening in the vertebrae, forming a sac filled with fluid. But this sac doesn't include the spinal cord, so nerve damage is less likely, though later complications are possible.
b. Myelomeningocele
Also known as open spina bifida, myelomeningocele is the most severe
form. The spinal canal is open along several vertebrae in the lower or middle back. The membranes and spinal nerves push through this opening at birth, forming a sac on the baby's back, typically exposing tissues and nerves. This makes the baby prone to life-threatening infections. PATHOPHYSIOLOGY
Spina bifida occurs because of defect in the orderly closure of vertebral
column and formation of spinal cord during 4th to 6th week of gestation .
During the 3rd week of gestation, a depression forms in the dorsal of the ectoderm in embryo.
This depression becomes deeper and its margins close dorsally to create a neural tube.
The ends of the neural tube close by the end of the 4th week of gestation.
The walls of neural tube thicken and become spinal cord and brain. The neural canal become ventricles and central canal of the spinal cord
The vertebral column is formed simultaneously with the neural tube.
Occurrence of the defect due to neural tube fails to close normally or
rupture after having once closed
CLINICAL FEATURES
1.Paralysis.
If the opening occurs at the top of the spine, the patient’s legs are more likely to be completely paralyzed, and there will be other problems with movement elsewhere in the body.
2.Cognitive symptoms.
Problems occurring in the neural tube have a negative effect on brain
development; the main part of the brain (cortex), especially the frontal part does not develop properly, leading to some cognitive problems.
3.Arnold-Chiari malformation.
There may also be Type 2 Arnold-Chiari malformation, an abnormal brain
development involving the cerebellum – this may affect the patient’s language processing and physical coordination skills.
4.Birthmark.
There may be a small birthmark, dimple or tuft of hair on the skin where the spinal defect is. 5.Learning difficulties:
People with spina bifida have normal intelligence. However, learning
difficulties can occur, leading to problems with attention, solving problems, reading, understanding spoken language, making plans, and grasping abstract concepts.
6.Bowel and urinary incontinence: These are common.
7.Meningitis:
There is a higher risk of meningitis among people with spina bifida. This can be life-threatening.
8.Other problems: In time, the individual may experience skin problems,
gastrointestinal problems, latex allergies, and depression. Skin can be more easily damaged if the person lacks sensation in the legs. They may injure or burn themselves without realizing.
DIAGNOSTIC FINDINGS
1.AFP levels.
Elevated maternal alpha fetoprotein levels in the maternal seruma nd
the amniotic fluid indicates the probability of CNS abnormalities.
2.Ultrasonography.
Ultrasonographic examination of the fetus may show an incomplete neural
tube.
3.Clinical examination. Diagnosis of spina bifida is made from clinical observation and examination.
4.Other imaging studies.
Additional evaluation of the defect may include magnetic resonance
imaging (MRI), computed tomography (CT), and myelography.
5.Amniocentesis
If a blood test shows high levels of AFP in the blood but the ultrasound is normal, the doctor may offer amniocentesis. An analysis of the sample indicates the level of AFP present in the amniotic fluid. A small amount of AFP is normally found in amniotic fluid. However, when an open neural tube defect is present, the amniotic fluid contains an elevated amount of AFP because the skin surrounding the baby's spine is gone and AFP leaks into the amniotic sac.
MANAGEMENT
Surgical Management
Surgery before birth
Fetal surgery for myelomeningocele, the most severe form of spina bifida, is a delicate surgical procedure where fetal surgeons open the uterus and close the opening in the baby's back while they are still in the womb. Fetal spina bifida surgery is shown to offer significantly better results than traditional repair after birth. Because spinal cord damage is progressive during gestation, prenatal repair of myelomeningocele may prevent further damage. Surgery after birth
If the baby has been diagnosed with spina bifida during pregnancy, need to deliver at a high-risk pregnancy centre. After delivery, the sac cannot stay outside of the body for a long time. It may tear or get infected, or it may already be ruptured exposing its delicate contents. The baby will have surgery to repair the sac within two or three days of birth. A neurosurgeon will do the operation. A neurosurgeon is a doctor who operates on the brain and spinal cord.
The baby may need an MRI before their operation to help the surgeons to better see the spinal cord. An MRI is a scan that takes special pictures of the inside of the body. An MRI scan requires a person to be still while the pictures are being taken. Some children may need medicine to help them keep still during the tests.
The purpose of the operation is to:
close the skin over the sac
prevent infection and further damage to the spinal cord
Nursing Management
Goals
The major goals for the patient are to:
Prevent infection. Maintain skin integrity. Prevent trauma related to disuse. Increase family coping skills, education about the condition, and support. Nursing interventions
The newborn child has a condition such as spina bifida can naturally cause the family to feel grief, anger, frustration, fear and sadness, however, nurses are there to help the family cope and understand the defect the child has.
1.Prevent infection.
Monitor the newborn’s vital signs, neurologic signs, and behavior frequently; administer prophylactic antibiotic as ordered; carry out routine aseptic technique; cover the sac with a sterile dressing moistened in a warm sterile solution and change it every 2 hours; the dressings may be covered with a plastic protective covering.
2.Promote skin integrity.
Placing a protective barrier between the anus and the sac may prevent contamination with fecal material, and diapering is not advisable with a low defect.
3.Prevent contractures of lower extremities.
Newborns with spina bifida often have talipes equinovarus (clubfoot)
and congenital hip dysplasia (dislocation of the hips); if there is loss of motion in the lower limbs because of the defect conduct range-of-motion exercises to prevent contractures; position the newborn so that the hips are abducted and the feet are in a neutral position; massage the knees and other bony prominences with lotion regularly, then pad them, and protect them from irritation.
4.Proper positioning of the newborn.
Maintain the newborn in a prone position so that no pressure is placed on the sac; after surgery, continue this positioning until the surgical site is well healed.
5.Promote family coping.
Be especially sensitive to their needs and emotions; encourage family members to express their feelings and emotions as openly as possible; provide privacy as needed for the family to mourn together over their loss; encourage the family members to cuddle and touch the newborn using proper precautions for the safety of the defect.
6.Provide family teaching.
Give family members information about the defect and encourage them to discuss their concerns and ask questions; provide information about the newborn’s present state, the proposed surgery, and follow-up care; information shall be provided in small segments to facilitate comprehension; after the surgery, teach the family to hold the newborn’s head, neck, and chest slightly raised in one hand during feeding; also teach them that stroking the newborn’s cheeks helps stimulate sucking. Pre-operative Care
1. Nursing Diagnosis: Risk of impaired skin integrity related to altered
motor and sensoryfunctions.
NursingInterventions
a.Avoid positioning the baby on back to prevent pressure on the sac.
b.Change the position of the baby frequently.
c.Provide meticulous skin and back care to keep the skin clean and dry.
d.Skin may be massaged periodically to stimulate blood circulation, with
special attention to bony prominences.
2. Nursing Diagnosis: Risk of injury and infection to the sac.
Nursing Interventions a. Do not position the baby on the back, as pressure over the sac may lead to rupture of sac.
b. Clean the sac aseptically using normal saline.
c. Cover the sac with sterile gauze pieces dipped in normal saline. This prevents the sac from dryness and rupture.
d. Change the wet saline gauze dressings every 2-4 hours, in order to keep the sac moist.
e. Prevent contamination of the sac with urine and feces. So, do not put diaper, as passing wine or stool inside the diaper keeps care giver unaware of soiling.
f.Frequently check the sac for any CSF leakage.
g.Prophylactic antibiotics must be administered to the infant. h.Infant must be handled canefully while feeding or giving care, to prevent injury to the sac. i.While the infant is placed in side lying position, keep a pillow behind the bad to prevent sudden rolling of infant on the bad. ' 3. Nursing Diagnosis: Impaired bladder and bowel function related to neurological deficit.
Nursing Interventions
a. Children with spina bifida may have the problem of retention of urine so intermittent catheterization is done and also taught to parents. b. Since bladder is an abdominal organ in infancy, pressure is applied gently on the lower abdomer‘ to manually express urine.
c. Monitor for sign and symptoms of urinary tract infection like cloudy or foul- smelling urine, fever etc. Administer prophylactic antibiotics to decrease the risk of urinary tract infection among patients who are catheterized.
d. Administer increased amount of fluids to the child as it helps in flushing out
the bladder and urinary tract.
e. If the chiild has urine incontinence, then also catheterization is essential. In
case of bowel incontinence, keep the child clean and dry.
f. Provide, frequent buttod( care and perianal care to infants with fecal incontinence, to prevent excoriation of perianal skin.
g. Provide soft bland food to the child having fecal incontinence. In case, the child has constipation administer laxatives as prescribed.
4. Nursing Diagnosis: Inadequate cerebral tissue perfusion related to
complications like hydrocephalus.
Nursing Interventions
a. Monitor for signs of hydrocephalus like irritability, feeding difficulty, reduced
alertness, tense or bulging fontanelle etc.
b. Administer diuretics like Mannitol and Acetazolamide as prescribed, to reduce
the intra cranial pressure. Postoperative Care 1.Nursing Diagnosis: Ineffective themioregulation related to surgery.
Nursing Interventions
a. Monitor the vital signs frequently after surgery.
b. Keep the infant warm, using radiant warmer or incubator. c. Avoid exposing the child unnecessarily. w. Maintain thennoneutral environment.
2. Nursing Diagnosis: Risk of development of infection related to surgery.
Nursing Interventions
a. Keep the operated site clean and dry. Observe for any drainage from the operated site.
b. Keep the baby in prone position, to avoid pressure on the operated site.
c. Dressing of the site should be done using aseptic techniques.
d. Administer the prescribed antibiotics.
3. Nursing Diagnosis: Altered nutrition less than body requirement related to
disease process.
Nursing Intervention a. Administer intravenous fluids as ordered.
b. . Maintain intake and output chart
c. Begin oral feeds as soon as infant starts tolerating the feeds.
d. Feed the infant in side lying position.
e. The baby can be held gently for feeding as soon as the surgical area is sufficiently healed.
f. Burp the infant frequently between the feeds.
4. Nursing Diagnosis: Risk of development of complications related to the
disease process.
Nursing Intervention a. In order to prevent development of hip or joint deformity, the nurse must pay attention to the position in which the infant is placed.
b. An infant with associated hip dysplasia is placed in prone position with legs slightly to moderately abducted. A pillow is placed between the knees to counteract hip subluxation.
c.In order to reduce chances of CSF leakage from the incision site, the infant may be placed in low trendelenburg's position as this helps in reducing CSF pressure at the site.
d. Monitor for development of hyd rocephalus.
e. lf hydrocephalus is suspected, elevate the head end of bed to reduce the intracranial pressure.
f. Provide passive range of motion exercises to prevent development of
contractures. g. Educate the parents regarding surgeries that may be needed for correction of deformities or . contractures .Such surgeries must be performed before the infant begins to walk.
h. Clubfoot may be corrected by repeated application of plaster cast.
SUMMARY
As far we discussed about spina bifida, its definition,types,causes and clinical
features, diagnostic findings and management
CONCLUSION Spina bifida is a birth defect that occurs when the spine and spinal cord don't form properly. It falls under the broader category of neural tube defects. The neural tube is the embryonic structure that eventually develops into the baby's brain and spinal cord and the tissues that enclose them.Normally, the neural tube forms early in pregnancy, and it closes by the 28th day after conception. In babies with spina bifida, a portion of the neural tube fails to develop or close properly, causing defects in the spinal cord and in the bones of the spine.Spina bifida can range from mild to severe, depending on the type of defect, size, location and complications. When early treatment for spina bifida is necessary, it's done surgically, although such treatment doesn't always completely resolve the problem BIBLIOGRAPHY
1. Wong L. Donna, Caton Hockenberry Marilyn, (2002) “WONG’S ESSENTIAL OF
PAEDIATRIC NURSING” 6th edition, published by Harcourt India (p) Ltd New Delhi Page No 911 – 917 2. Ghai O.P& Gupta piyush, Paul V.K.(2005) “GHAI ESSENTIAL PAEDICTRICS” 6th edition, published by CBS publishers & distributors New Delhi Page No – 338. 3. AssumaBeevi, (2009) ''TEXT BOOK OF PEDIATRIC NURSING'' I st edition, published by Elsevier publishers Noida UP Page No 136-138. 4. Achar's Text book of pediatrics,Fourth edition ,Universities publishers ,India. 5. R.Kulshesthra(2006) "COMMON PROBLEMS IN PEDIATRIC SURGERY"Second edition.CBS Publication.Newdelhi