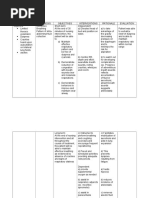
Assessment Nursing Diagnosis Background Knowledge Planning Interventions Rationale Evaluation Independent
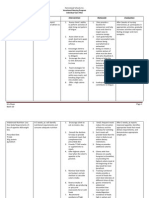
Assessment Nursing Diagnosis Background Knowledge Planning Interventions Rationale Evaluation Independent
Download as docx, pdf, or txt
You might also like
- Nursing Care Plan: CancerDocument6 pagesNursing Care Plan: Cancerneuronurse75% (8)
- NCP: Patient With Peptic Ulcer DiseaseDocument3 pagesNCP: Patient With Peptic Ulcer DiseaseICa Marlina0% (1)
- VII. Pathophysiology of PUDDocument1 pageVII. Pathophysiology of PUDJehmima Gloriani100% (1)
- Signs and Symptoms Nursing Diagnosis Rationale Objective Nursing Intervention Rationale EvaluationDocument5 pagesSigns and Symptoms Nursing Diagnosis Rationale Objective Nursing Intervention Rationale EvaluationRemuelMagsinoNo ratings yet
- Cholecystitis NCPDocument5 pagesCholecystitis NCPtsukino143No ratings yet
- Nursing Care Plan (Peptic Ulcer)Document4 pagesNursing Care Plan (Peptic Ulcer)JennyLapitanNo ratings yet
- NCP Peptic Ulcer DsDocument4 pagesNCP Peptic Ulcer Dsplug0650% (10)
- NCP For COLON Cancer PatientDocument4 pagesNCP For COLON Cancer PatientCarolina Tardecilla100% (1)
- Nursing Care Plan: Fluid Volume DeficitDocument2 pagesNursing Care Plan: Fluid Volume DeficitGenEsis CarandangNo ratings yet
- NCP HemothoraxDocument3 pagesNCP Hemothoraxroseonabreeze0% (2)
- NCP For UtiDocument3 pagesNCP For UtiAaron Sanchez100% (1)
- Liver Cirrhosis NCP 1Document6 pagesLiver Cirrhosis NCP 1Paolo Rafael D EsguerraNo ratings yet
- NAPREXDocument2 pagesNAPREXKarl EdemNo ratings yet
- NCP Liver CirrhosisDocument7 pagesNCP Liver CirrhosisIris Jimenez-BuanNo ratings yet
- NCP AppendicitisDocument2 pagesNCP AppendicitisArnel Luces Beato100% (1)
- NCP Imbalanced NutritionDocument3 pagesNCP Imbalanced NutritionAav Canlas100% (1)
- Problem Nursing Diagnosis Outcome Plan Intervention Evaluation Subjective Data: "Masakit Po Yung Sa Short Term: IndependentDocument2 pagesProblem Nursing Diagnosis Outcome Plan Intervention Evaluation Subjective Data: "Masakit Po Yung Sa Short Term: IndependentkyawNo ratings yet
- NCP DiabetesDocument3 pagesNCP DiabetesKartika MilaningrumNo ratings yet
- Case Study: Gastrointestinal System of Older People Case Scenario: LapayDocument1 pageCase Study: Gastrointestinal System of Older People Case Scenario: LapayAriaNo ratings yet
- NCPDocument10 pagesNCPMack Jhed AnarconNo ratings yet
- NCP Loss of AppetiteDocument5 pagesNCP Loss of AppetiteStenneli Gumban Trojillo50% (2)
- Ugib Case StudyDocument30 pagesUgib Case StudyVenus Glaze Verzola80% (5)
- Nur81 NCP GastroDocument4 pagesNur81 NCP GastroJordan Gonzales100% (1)
- NcpsDocument10 pagesNcpskotoirNo ratings yet
- NCP LymphomaDocument3 pagesNCP LymphomaJohn Emmanuel Tatad TudNo ratings yet
- NCP - Activity IntoleranceDocument3 pagesNCP - Activity Intolerancejanelee2824No ratings yet
- NCP DMDocument21 pagesNCP DMKate ManalastasNo ratings yet
- PUD PathophysiologyDocument1 pagePUD PathophysiologyHerbert A Serquina100% (1)
- Cues Nursing DX Objectives Nursing Interventions RationaleDocument5 pagesCues Nursing DX Objectives Nursing Interventions RationaleJamie IcabandiNo ratings yet
- Altered Bowel EliminationDocument1 pageAltered Bowel EliminationneoclintNo ratings yet
- NCP (Appendectomy)Document3 pagesNCP (Appendectomy)Joyce Anne Lambiquit RN100% (2)
- NCP Liver CirrosisDocument2 pagesNCP Liver CirrosisRosebud RoseNo ratings yet
- NCP Acute PainDocument3 pagesNCP Acute PainAlex MarieNo ratings yet
- Fluid Volume Deficit (GI Bleeding) NCPDocument2 pagesFluid Volume Deficit (GI Bleeding) NCPReina Samson100% (2)
- NCP MiDocument4 pagesNCP MiPitaca Madiam Annabehl PaulNo ratings yet
- Novilyn C. Pataray BSN - Ii: Assessment Diagnosi S Pathophysiolog Y Planning Interevention Rationale EvaluationDocument1 pageNovilyn C. Pataray BSN - Ii: Assessment Diagnosi S Pathophysiolog Y Planning Interevention Rationale EvaluationCharina AubreyNo ratings yet
- Imbalnce Nutrition Less Than Body RequirementsDocument3 pagesImbalnce Nutrition Less Than Body RequirementselheezaNo ratings yet
- NCP Fluid Volume DeficitDocument3 pagesNCP Fluid Volume DeficitNecheal BaayNo ratings yet
- NCP - Drug Study - Peptic UlcerDocument18 pagesNCP - Drug Study - Peptic UlcerEmi EspinoNo ratings yet
- Nursing Care Plan Problem: Acute Intermittent Moderate PainDocument1 pageNursing Care Plan Problem: Acute Intermittent Moderate PainDiana Laura Lei100% (3)
- NCP Arra AnemiaDocument2 pagesNCP Arra AnemiaShin GuevaraNo ratings yet
- Liver Cirrhosis NCPDocument3 pagesLiver Cirrhosis NCPSharmaine MadlaNo ratings yet
- Assessment Diagnosis Planning Interventions Rationale EvaluationDocument2 pagesAssessment Diagnosis Planning Interventions Rationale EvaluationStar Alvarez100% (2)
- NCP CholelithiasisDocument2 pagesNCP Cholelithiasiskmpg11100% (2)
- Upper Gastrointestin Al Bleeding: Case Presentation BSN 3-1Document80 pagesUpper Gastrointestin Al Bleeding: Case Presentation BSN 3-1Lanrose Parocha100% (1)
- NCP DiarrheaDocument2 pagesNCP DiarrheaMiguelMartinNo ratings yet
- Impaired Skin IntegrityDocument2 pagesImpaired Skin IntegrityLilet Dela CruzNo ratings yet
- Drug StudyDocument5 pagesDrug Studypaulkris_14100% (1)
- Abdominal Pain NCPDocument3 pagesAbdominal Pain NCPRo-anne Aku100% (1)
- JVJV NCP Risk For Fluid Volume DeficitDocument2 pagesJVJV NCP Risk For Fluid Volume DeficitvicenteturasNo ratings yet
- NCP-CKD LabcoDocument5 pagesNCP-CKD Labcojay kusainNo ratings yet
- NCP-DaqueDocument4 pagesNCP-Daquejillmonicadaquipil7No ratings yet
- NCP Nausea and VomitingDocument4 pagesNCP Nausea and VomitingKingJayson Pacman06No ratings yet
- GASTRITISDocument11 pagesGASTRITIStamannaNo ratings yet
- Nursing Care Plan: Assessment Nursing Diagnosis Rationale Desired Outcome Nursing Intervention Justification EvaluationDocument2 pagesNursing Care Plan: Assessment Nursing Diagnosis Rationale Desired Outcome Nursing Intervention Justification EvaluationDan MandigNo ratings yet
- Ectopic PregnancyDocument2 pagesEctopic PregnancyRex Dave Guinoden100% (1)
- NCP Case Analysis GastritisDocument7 pagesNCP Case Analysis GastritisSteffi GolezNo ratings yet
- Group 47 NCP Bicarbonate DisordersHyperbicarbonatemia and HypobicarbonatemiaDocument6 pagesGroup 47 NCP Bicarbonate DisordersHyperbicarbonatemia and HypobicarbonatemiaAngel Joyce MontezaNo ratings yet
- September 5, 2022: Date / Time Cues Nursing Diagnosis Rationale EvaluationDocument2 pagesSeptember 5, 2022: Date / Time Cues Nursing Diagnosis Rationale EvaluationCynelle AguilonNo ratings yet
- Nursing Care Plan Diarrhea Assessment Diagnosis Planning Interventions Rationale EvaluationDocument8 pagesNursing Care Plan Diarrhea Assessment Diagnosis Planning Interventions Rationale EvaluationKrah100% (1)
- Amelia Lorensia - Membandingkan Kejadian Gangguan - 2019Document24 pagesAmelia Lorensia - Membandingkan Kejadian Gangguan - 2019Mochammad Azis firmansyahNo ratings yet
- Nur 098 Module 1 8Document22 pagesNur 098 Module 1 8silvest3sterNo ratings yet
- Haley Mahr Resume 11-9-2021Document3 pagesHaley Mahr Resume 11-9-2021api-548262948No ratings yet
- Energy Medicine The Secrets of A Master Practitioner by Donna Eden Workbook SP 2018 PDFDocument14 pagesEnergy Medicine The Secrets of A Master Practitioner by Donna Eden Workbook SP 2018 PDFDavid Malagon Mata100% (3)
- Ophthalmia NeonatorumDocument17 pagesOphthalmia NeonatorumIndranil DuttaNo ratings yet
- The Scope of Regulatory AffairsDocument7 pagesThe Scope of Regulatory AffairsSankarshan KvNo ratings yet
- Second Quarter Examination For MAPEH 7: Macabalan National High SchoolDocument4 pagesSecond Quarter Examination For MAPEH 7: Macabalan National High SchoolGab N MyamieNo ratings yet
- Screening For Health Fitness and WellnessDocument22 pagesScreening For Health Fitness and WellnessMuneeb Shahid Hussain50% (2)
- Combating Fungal Infections - Problems and RemedyDocument549 pagesCombating Fungal Infections - Problems and RemedyChristopher Phillips100% (1)
- Silabus Bimbingan Internal CBT UKMPPD FK ULM ReproduksiDocument5 pagesSilabus Bimbingan Internal CBT UKMPPD FK ULM ReproduksiDyah PutriNo ratings yet
- Keyana Resume 4 14 2024Document2 pagesKeyana Resume 4 14 2024api-745740782No ratings yet
- CounsellingDocument2 pagesCounsellingRavi YadavNo ratings yet
- RNTCP - Wikipedia, The Free EncyclopediaDocument5 pagesRNTCP - Wikipedia, The Free EncyclopediaakurilNo ratings yet
- Radiant HealthDocument2 pagesRadiant HealthMarcio GonçalvesNo ratings yet
- Cab o Sil M 5p MsdsDocument8 pagesCab o Sil M 5p MsdsAli AhmedNo ratings yet
- 1TM Cancer Pain - Introduction & Principles 2012 (Trainer's Guide)Document39 pages1TM Cancer Pain - Introduction & Principles 2012 (Trainer's Guide)khairulfatinNo ratings yet
- Intact (Polymeric/Blenderized) : Enteral Nutrition (Summary of Diet/Formula)Document2 pagesIntact (Polymeric/Blenderized) : Enteral Nutrition (Summary of Diet/Formula)Angela NeriNo ratings yet
- 3 Solution Focused TherapyDocument17 pages3 Solution Focused TherapyEllia WatersNo ratings yet
- Assignment 1 Introduction To MicroorganismsDocument4 pagesAssignment 1 Introduction To MicroorganismsVillanueva, AbegailNo ratings yet
- 616062692662Document34 pages616062692662ABHISHEK YADAVNo ratings yet
- Generic Shoulder Physiotherapy Exercises Sheet: Information For Patients Orthopaedic Shoulder ServiceDocument16 pagesGeneric Shoulder Physiotherapy Exercises Sheet: Information For Patients Orthopaedic Shoulder ServiceBence KlusóczkiNo ratings yet
- Kasus Saraf 2Document2 pagesKasus Saraf 2TessarinaNo ratings yet
- Draft CoS DinethmaDocument2 pagesDraft CoS DinethmaDinethma SauyrangiNo ratings yet
- Answer ALL Questions. 1 Read The Passage Below. Use The Information in The Passage and Your Own KnowledgeDocument3 pagesAnswer ALL Questions. 1 Read The Passage Below. Use The Information in The Passage and Your Own KnowledgeArif01721No ratings yet
- The Impact of Leadership Styles of Nurse Managers On Nurses' Motivation and Turnover Intention Among Jordanian NursesDocument12 pagesThe Impact of Leadership Styles of Nurse Managers On Nurses' Motivation and Turnover Intention Among Jordanian NursesIzabelle KallyNo ratings yet
- Cellular and Molecular Basis of Health - ScholisticoDocument55 pagesCellular and Molecular Basis of Health - ScholisticojoffuhNo ratings yet
- CPCHILD English Parent 5.0 WatermarkedDocument9 pagesCPCHILD English Parent 5.0 WatermarkedAz-Zahraa NaasNo ratings yet
- Clarithromycin Drug StudyDocument1 pageClarithromycin Drug StudyDivine LavaNo ratings yet
- Increasing The Access of The Poor and The Marginalized To Much Needed Health CareDocument411 pagesIncreasing The Access of The Poor and The Marginalized To Much Needed Health CareBasil FletcherNo ratings yet
- Physical Diagnosis: Nishalini RavindranDocument6 pagesPhysical Diagnosis: Nishalini RavindranShalini RavNo ratings yet