Pharmacology 10 11
Pharmacology 10 11
Download as docx, pdf, or txt
You might also like
- AMOEBIASISDocument44 pagesAMOEBIASISJorge Rabaja100% (1)
- Health Grade10 4th QuarterDocument40 pagesHealth Grade10 4th Quarterd-fbuser-33831503179% (186)
- Endorsement PDFDocument34 pagesEndorsement PDFCharlie Abagon100% (5)
- Graduate Personal Statement For Admission For MPH DegreeDocument2 pagesGraduate Personal Statement For Admission For MPH DegreeElizabeth33% (3)
- Pharmacology ReviewDocument8 pagesPharmacology ReviewEmerald SpanglerNo ratings yet
- Antifungal Drugs: Side Effects and Adverse Reactions of Amphotericin BDocument23 pagesAntifungal Drugs: Side Effects and Adverse Reactions of Amphotericin BElizabeth IdananNo ratings yet
- 14-Antiameobic Antifungal 2021Document22 pages14-Antiameobic Antifungal 2021Amr SalemNo ratings yet
- Veterinary Antimicrobial DrugsDocument5 pagesVeterinary Antimicrobial DrugsLaureece Salm ApduhanNo ratings yet
- Antibiotics PharmaDocument4 pagesAntibiotics PharmaJohn Dave V. VillarmenteNo ratings yet
- 3 - Antifungal DrugsDocument9 pages3 - Antifungal Drugsahmed7778258No ratings yet
- Antibiotics Cheat Sheet (Bootcamp)Document5 pagesAntibiotics Cheat Sheet (Bootcamp)ksonu521215No ratings yet
- NU115 Chapter 42 AntifungalDocument16 pagesNU115 Chapter 42 Antifungalsarah weissNo ratings yet
- AntibioticsDocument7 pagesAntibioticsRellie CastroNo ratings yet
- HCC Exam 4Document20 pagesHCC Exam 4Sheri BarlingNo ratings yet
- FTX Infeksi JamurDocument64 pagesFTX Infeksi JamurNafisah SofiaNo ratings yet
- Antibiotic Review & Resistance LectureDocument32 pagesAntibiotic Review & Resistance LecturesamritiNo ratings yet
- Chemotherapy Class 2Document29 pagesChemotherapy Class 2Yasir SalumNo ratings yet
- Phrama-Biotic NdocxDocument2 pagesPhrama-Biotic NdocxAzizullah NooriNo ratings yet
- Micro112 Antifungal DrugsDocument2 pagesMicro112 Antifungal Drugsfiskar327No ratings yet
- 2.5 Anti FungalDocument2 pages2.5 Anti FungalYra JhaneNo ratings yet
- BASES FARMACOLOGICAS - S12 - Infografias-OkDocument4 pagesBASES FARMACOLOGICAS - S12 - Infografias-OkCorazon Pamela Cortez SalinasNo ratings yet
- Erythromycin & Pneumococcal VaccineDocument6 pagesErythromycin & Pneumococcal VaccineNikki Joy NavarroNo ratings yet
- PHARMADocument25 pagesPHARMAAtteya Mogote AbdullahNo ratings yet
- Antiprotozoal DrugsDocument9 pagesAntiprotozoal DrugsneroxaktNo ratings yet
- Hand Out 7 - 110035Document12 pagesHand Out 7 - 110035Yollyally MapsNo ratings yet
- Antibiotics: Penicillium-Terrestrial Mold Cephalosporium - Marine Mold Bacillus - Bacteria Streptomyces - BacteriaDocument9 pagesAntibiotics: Penicillium-Terrestrial Mold Cephalosporium - Marine Mold Bacillus - Bacteria Streptomyces - BacteriavexicaNo ratings yet
- Occular Pharmacology - Short Notes6851443241353226538Document28 pagesOccular Pharmacology - Short Notes6851443241353226538Aashutosh KumarNo ratings yet
- Microbio Exam 3Document13 pagesMicrobio Exam 3Cathy LyNo ratings yet
- 2024.ENT - Trans03.pharmacology of ENTDocument6 pages2024.ENT - Trans03.pharmacology of ENTEADOH RO2No ratings yet
- Dr. Fouzia Alima Associate Professor Department of PharmacologyDocument19 pagesDr. Fouzia Alima Associate Professor Department of PharmacologyShokh ComputerNo ratings yet
- AntiProtozoal agentsDocument9 pagesAntiProtozoal agentsLavanyaNo ratings yet
- Pharmacology - Aminoglycosides Glycopaptides & Sulfonamides (For Editing)Document6 pagesPharmacology - Aminoglycosides Glycopaptides & Sulfonamides (For Editing)bublelicious911No ratings yet
- Cep Halo Sporin SDocument51 pagesCep Halo Sporin Smonir61No ratings yet
- Pharma Module 4Document4 pagesPharma Module 4Chelsy Sky Sacan100% (1)
- GIT NursingDocument8 pagesGIT NursingBasa, Rica Mae P.No ratings yet
- BenadrylDocument2 pagesBenadrylsamfandood10No ratings yet
- Cours farmaco antibiotiques(1)Document7 pagesCours farmaco antibiotiques(1)sarahvestric19No ratings yet
- Anti Protozoal DrugsDocument3 pagesAnti Protozoal Drugsdaku daddyNo ratings yet
- Antifungaldrugs 150519204813 Lva1 App6892Document54 pagesAntifungaldrugs 150519204813 Lva1 App6892Jennifer S ZiegenNo ratings yet
- Pharma Midterm ReviewerDocument7 pagesPharma Midterm Reviewercharicemae021415No ratings yet
- GIT Infections 2024-2025Document67 pagesGIT Infections 2024-2025m.m.mghyda3No ratings yet
- Bacterial Skin Diseases - Section 3 Fall 2024Document19 pagesBacterial Skin Diseases - Section 3 Fall 2024mgermino307No ratings yet
- Hand Out AntibioticsDocument13 pagesHand Out AntibioticsMinhwa KimNo ratings yet
- Antibiotics in EndodonticsDocument74 pagesAntibiotics in EndodonticsdrishyaNo ratings yet
- Pharmacology for Dummies 1Document114 pagesPharmacology for Dummies 1MariaNo ratings yet
- Part 1 AntifungalsDocument71 pagesPart 1 AntifungalsDR.NITHA WILLYNo ratings yet
- 12 July Antifungal_5eae57a7 e251 4b1b Ad14 5aa2b710b96bDocument11 pages12 July Antifungal_5eae57a7 e251 4b1b Ad14 5aa2b710b96bSahil KhanNo ratings yet
- Microbio Lec 7 - Clostridium and BacillusDocument5 pagesMicrobio Lec 7 - Clostridium and Bacillusapi-3743217100% (1)
- Antibiotics: Lecture 6: Antibiotics For Anaerobic InfectionsDocument12 pagesAntibiotics: Lecture 6: Antibiotics For Anaerobic InfectionsMuath AlqarniNo ratings yet
- Exotoxic Model Corynebacterium DiphteriaeDocument37 pagesExotoxic Model Corynebacterium Diphteriaekohinoor815256100% (1)
- Antimicrobials and Cytotoxic Drugs: DR Caroline Tetteyfio Koney 37 Military Hospital Accra Feb 2012Document58 pagesAntimicrobials and Cytotoxic Drugs: DR Caroline Tetteyfio Koney 37 Military Hospital Accra Feb 2012Fred OseiNo ratings yet
- M.02 AMINOGLYCOSIDES (Dr. Buñag) 03-07-2018 (PART 2)Document3 pagesM.02 AMINOGLYCOSIDES (Dr. Buñag) 03-07-2018 (PART 2)PAUL ALINGKAYONNo ratings yet
- Antifungal AgentsDocument23 pagesAntifungal AgentsDiriba feyisaNo ratings yet
- ANTI FungalDocument7 pagesANTI FungalSteve ShirmpNo ratings yet
- Antifungal Drugs: Anti-Infectives and Anti-Inflammatory: Ncm106 - Pharmacology 2 Semester, AY 2020-2021Document34 pagesAntifungal Drugs: Anti-Infectives and Anti-Inflammatory: Ncm106 - Pharmacology 2 Semester, AY 2020-2021imnas100% (1)
- Chapter 21: Nonfermenting Gram-Negative Bacilli: I. General CharacteristicsDocument5 pagesChapter 21: Nonfermenting Gram-Negative Bacilli: I. General CharacteristicsSamanthaNo ratings yet
- Anti-Fungal Drugs - KatzungDocument2 pagesAnti-Fungal Drugs - Katzungsarguss14100% (2)
- ClostridiumDocument8 pagesClostridiumlianysusantiNo ratings yet
- Prepared by The: Antibiotic Guidelines 3 Edition 2011Document82 pagesPrepared by The: Antibiotic Guidelines 3 Edition 2011araNo ratings yet
- PEDIA Bacterial Infections Part 2 Dr. E. Lim FinalDocument5 pagesPEDIA Bacterial Infections Part 2 Dr. E. Lim FinalClaire DuNo ratings yet
- 2023.ENT - Trans02.pharmacology of ENTDocument3 pages2023.ENT - Trans02.pharmacology of ENTEADOH RO2No ratings yet
- Antifungal Drugs: Dr. K. Sreedhara R. Pai Professor Department of Pharmacology Mcops, Mahe, MANIPAL-576 104Document88 pagesAntifungal Drugs: Dr. K. Sreedhara R. Pai Professor Department of Pharmacology Mcops, Mahe, MANIPAL-576 104jhanavi rajeshNo ratings yet
- Antifungal and Antiviral AgentsDocument14 pagesAntifungal and Antiviral AgentsFrancis ChegeNo ratings yet
- Newborn Assessment: A Reading OnDocument14 pagesNewborn Assessment: A Reading OnCharlie AbagonNo ratings yet
- Rabies Elimination Services Program CHN RotDocument9 pagesRabies Elimination Services Program CHN RotCharlie AbagonNo ratings yet
- Icu - SG 2 2Document230 pagesIcu - SG 2 2Charlie AbagonNo ratings yet
- BSN2A PreClin Group 5 PA PimentelDocument41 pagesBSN2A PreClin Group 5 PA PimentelCharlie AbagonNo ratings yet
- FCT Updated 2Document3 pagesFCT Updated 2Charlie AbagonNo ratings yet
- AntihpnDocument3 pagesAntihpnCharlie AbagonNo ratings yet
- IIII :::: : S EsentDocument22 pagesIIII :::: : S EsentCharlie AbagonNo ratings yet
- Sinabawan G Gulay: Presented By: Group 1 of BSN 2JDocument21 pagesSinabawan G Gulay: Presented By: Group 1 of BSN 2JCharlie AbagonNo ratings yet
- CHN Implementing Family Care PlanDocument2 pagesCHN Implementing Family Care PlanCharlie Abagon100% (1)
- Family Planning CHN RotDocument7 pagesFamily Planning CHN RotCharlie AbagonNo ratings yet
- Chapter 13 - Lymphatic SystemDocument4 pagesChapter 13 - Lymphatic SystemCharlie AbagonNo ratings yet
- Thai-K-C Drama, BL Series, BTS, Tice, Itzy, BalckpinkDocument2 pagesThai-K-C Drama, BL Series, BTS, Tice, Itzy, BalckpinkCharlie AbagonNo ratings yet
- BEDMAKINGDocument7 pagesBEDMAKINGCharlie AbagonNo ratings yet
- Site of The First MassDocument6 pagesSite of The First MassCharlie AbagonNo ratings yet
- Little Girl Lost: A Case Study On Defective Cellular OrganellesDocument7 pagesLittle Girl Lost: A Case Study On Defective Cellular OrganellesClarissa CaroNo ratings yet
- LEsson-Guide-G9-Biology Module 1 On TemplateDocument29 pagesLEsson-Guide-G9-Biology Module 1 On Templateconstancia G, caraan0% (1)
- 3 Altered Renal Tissue Perfusion Chronic Renal Renal Failure Nursing Care PlansDocument4 pages3 Altered Renal Tissue Perfusion Chronic Renal Renal Failure Nursing Care Planssapiah raman100% (1)
- Summer 23Document11 pagesSummer 23MUHAMMAD09No ratings yet
- Sorcery and Fortune TellingDocument27 pagesSorcery and Fortune TellingKishor Kumar100% (1)
- Biological HazardDocument2 pagesBiological HazardBryan JamesNo ratings yet
- BIO 101 - General Biology 1 November 2024Document50 pagesBIO 101 - General Biology 1 November 2024christianahtianah9No ratings yet
- Serra Pep TaseDocument3 pagesSerra Pep TaseOdessa FileNo ratings yet
- Driving and Your Health: A Guide For Road Transport OperatorsDocument29 pagesDriving and Your Health: A Guide For Road Transport OperatorsNgaire TaylorNo ratings yet
- Risk Factors For Granulocytopenia in Patients With Graves' Disease Receiving Antithyroid DrugsDocument5 pagesRisk Factors For Granulocytopenia in Patients With Graves' Disease Receiving Antithyroid DrugsInterna UnhasNo ratings yet
- Daftar Diagnosa Borang Dokter InternsipDocument13 pagesDaftar Diagnosa Borang Dokter InternsipAnonymous WKPdl5rTNo ratings yet
- Question 1hDocument3 pagesQuestion 1hItharshan IndreswaranNo ratings yet
- The Potential Hypoglycemic Activity of Pinus Merkusii Bark Ethanolic Extract in Streptozotocin-Induced Diabetic Rats PDFDocument12 pagesThe Potential Hypoglycemic Activity of Pinus Merkusii Bark Ethanolic Extract in Streptozotocin-Induced Diabetic Rats PDFBung ChusNo ratings yet
- GROUP - 1 Introduction To Emerging and Re-Emerging DiseasesDocument23 pagesGROUP - 1 Introduction To Emerging and Re-Emerging DiseasesZubairiya afrin Abdul kareemNo ratings yet
- 9 Edition Antithrombotic Therapy and Prevention of Thrombosis Guidelines: Summary Prevention of VTE CHEST 2012Document3 pages9 Edition Antithrombotic Therapy and Prevention of Thrombosis Guidelines: Summary Prevention of VTE CHEST 2012Jason NiskyNo ratings yet
- Straube, Toxic Bodies - Ticks, Trans Bodies, and The Ethics of Response-Ability in Art and Activist WritingDocument23 pagesStraube, Toxic Bodies - Ticks, Trans Bodies, and The Ethics of Response-Ability in Art and Activist Writing_diklic_No ratings yet
- The Power Within YouDocument11 pagesThe Power Within YoucezarmirunaNo ratings yet
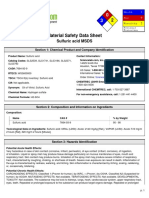
- MSDS Sulphuric Acid PDFDocument7 pagesMSDS Sulphuric Acid PDFshaik rafi100% (2)
- AntacidsDocument2 pagesAntacidsMegan Samson0% (1)
- Post Operative Complications and Post Operative MonitoringDocument21 pagesPost Operative Complications and Post Operative MonitoringMNo ratings yet
- Short and Long Term Impacts of COVID-19 On The Pharmaceutical SectorDocument7 pagesShort and Long Term Impacts of COVID-19 On The Pharmaceutical SectorPeyman KazemianhaddadiNo ratings yet
- Excitotoxins The Taste That Kills Russell Blaycock, MDDocument8 pagesExcitotoxins The Taste That Kills Russell Blaycock, MDyamada yamadaNo ratings yet
- 1 - Paroxysmal DisordersDocument48 pages1 - Paroxysmal DisorderszhoujNo ratings yet
- The Transatlantic Slave TradeDocument3 pagesThe Transatlantic Slave Tradeshanoya.linton1009No ratings yet
- Laporan Kegiatan p2kb AmalDocument16 pagesLaporan Kegiatan p2kb AmalAulia Urrahmah100% (1)
- Is Basic Technique Used For The Examination of Movement and For Initiating Movement Into A Program of Therapeutic InterventionDocument9 pagesIs Basic Technique Used For The Examination of Movement and For Initiating Movement Into A Program of Therapeutic InterventionEric Carlos YumulNo ratings yet
- Text EvaluationDocument2 pagesText EvaluationClarixcNo ratings yet