NCP Drug
NCP Drug
Download as docx, pdf, or txt
You might also like
- Haiderpur Water Treatment PlantDocument23 pagesHaiderpur Water Treatment Plantakshay malik67% (6)
- Valdez Reflective-Questions PDFDocument3 pagesValdez Reflective-Questions PDFDexel Lorren ValdezNo ratings yet
- Subjective Data:: Assessme NT Diagnos IS Planning Intervention Rationale EvaluationDocument1 pageSubjective Data:: Assessme NT Diagnos IS Planning Intervention Rationale EvaluationCuttie Anne GalangNo ratings yet
- Drugs Study and Discharge Plan Arnold and SelwynDocument17 pagesDrugs Study and Discharge Plan Arnold and SelwynArnold ZamoroNo ratings yet
- Hypothyroidism (Drug Study)Document2 pagesHypothyroidism (Drug Study)Krisianne Mae Lorenzo FranciscoNo ratings yet
- Clinical Problem Solving in Periodontology and ImplantologyDocument195 pagesClinical Problem Solving in Periodontology and ImplantologyEshan Verma100% (21)
- MCN Case Presentation Group 2 1Document68 pagesMCN Case Presentation Group 2 1Mary-Ann JagonobNo ratings yet
- Tetralogy of FallotDocument4 pagesTetralogy of FallotLiezelle ArrozalNo ratings yet
- Intrapartum Assessment: Jonelle Baloloy, MD MCMC Ob GyneDocument39 pagesIntrapartum Assessment: Jonelle Baloloy, MD MCMC Ob GyneJonelle baloloyNo ratings yet
- VenoferinfDocument10 pagesVenoferinfzerin_atinNo ratings yet
- NCP IcuDocument2 pagesNCP IcuDiana MuañaNo ratings yet
- I Patient Assessment Data BaseDocument12 pagesI Patient Assessment Data BaseJanice_Fernand_1603No ratings yet
- Hemolytic Disease of The Newborn: (Erythroblastosis Fetalis)Document17 pagesHemolytic Disease of The Newborn: (Erythroblastosis Fetalis)sandeepv08No ratings yet
- Assessment Nursing Diagnosis Planning Intervention Rationale Core CompetenciesDocument13 pagesAssessment Nursing Diagnosis Planning Intervention Rationale Core CompetenciesMina RacadioNo ratings yet
- Module4 Promabortion Week 8Document21 pagesModule4 Promabortion Week 8Emmy Flor ValmoriaNo ratings yet
- Drug Study SpironolactoneDocument2 pagesDrug Study SpironolactonePau-pau BasiNo ratings yet
- Chapter 1. Physical Activity and Exercise: Learning OutcomesDocument5 pagesChapter 1. Physical Activity and Exercise: Learning OutcomesKrish NalingNo ratings yet
- Acetaminophen (Tylenol)Document2 pagesAcetaminophen (Tylenol)amelia hearonNo ratings yet
- Name of Drug Mechanism of Action Indications Contra-Indications Side Effects Nursing ConsiderationsDocument10 pagesName of Drug Mechanism of Action Indications Contra-Indications Side Effects Nursing ConsiderationsmidskiescreamzNo ratings yet
- Lower Limb Trauma - 5Document12 pagesLower Limb Trauma - 5Renee RoSeNo ratings yet
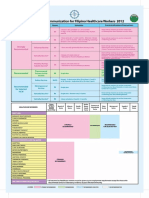
- Recommended Immunization For Filipino Healthcare Workers 2012Document1 pageRecommended Immunization For Filipino Healthcare Workers 2012SMRNo ratings yet
- Risk NCP Decreased Cardiac OutputDocument2 pagesRisk NCP Decreased Cardiac OutputMICHELLE FACTONo ratings yet
- Nursing Care Plan DMDocument8 pagesNursing Care Plan DMnikaaraaaNo ratings yet
- Learning Derived (Lysha)Document1 pageLearning Derived (Lysha)Choy DavidNo ratings yet
- Care Plan PedsDocument7 pagesCare Plan PedsdjbhetaNo ratings yet
- NCPDocument2 pagesNCPNichole Audrey SaavedraNo ratings yet
- Antepartum Haemorrhage MXDocument22 pagesAntepartum Haemorrhage MXAmir Hilmi Abd AzizNo ratings yet
- Case Pres Cerebrovascular DiseaseDocument34 pagesCase Pres Cerebrovascular DiseaseADRIATICO JAROSLUVNo ratings yet
- Phenobarbital Risk For Injury EAMCDocument4 pagesPhenobarbital Risk For Injury EAMCkeitacNo ratings yet
- RLE314 CU4 MedicationDocument7 pagesRLE314 CU4 MedicationVAL ASHLIE ACEBARNo ratings yet
- Assessment Explanation of The Problem Objectives Nursing Interventions Rationale EvaluationDocument5 pagesAssessment Explanation of The Problem Objectives Nursing Interventions Rationale EvaluationTedd CamilingNo ratings yet
- Warfarin - Drug InformationDocument23 pagesWarfarin - Drug InformationTestesteNo ratings yet
- NCP & Drug Study (Tondo Med)Document5 pagesNCP & Drug Study (Tondo Med)Kevin_Remollo_2431No ratings yet
- Abruptio PlacentaDocument10 pagesAbruptio PlacentaDoc DudayNo ratings yet
- Assessment Nursing Diagnosis Scientific Basis Planning Interventions RationaleDocument3 pagesAssessment Nursing Diagnosis Scientific Basis Planning Interventions RationaleJose Rey BuenavistaNo ratings yet
- Drug Study 12Document4 pagesDrug Study 12Nathalie kate petallarNo ratings yet
- Galantine HBRDocument5 pagesGalantine HBRArone SebastianNo ratings yet
- Febrile Seizures NCPDocument9 pagesFebrile Seizures NCPNurul IrhamnaNo ratings yet
- Pathophysiology (Normal Spontaneous Vaginal Delivery)Document2 pagesPathophysiology (Normal Spontaneous Vaginal Delivery)Jose Bryan NacillaNo ratings yet
- Measuring Blood Glucose LevelDocument7 pagesMeasuring Blood Glucose LevelHuda BehroozNo ratings yet
- Ineffective Tissue PerfussionDocument2 pagesIneffective Tissue Perfussionmonico39No ratings yet
- Drug Study Pyrantel & CefuroximeDocument2 pagesDrug Study Pyrantel & CefuroximeMikhael Briones ApasNo ratings yet
- BFS Uti 111Document65 pagesBFS Uti 111JemsMei Comparativo MensuradoNo ratings yet
- Discharge PlanDocument5 pagesDischarge PlanrraksNo ratings yet
- Drug StudyDocument4 pagesDrug StudyAli Longasa CortezNo ratings yet
- Javier, Jomar A. BSN121 Group 83 Nursing Care Plan (Pediatric Patient)Document7 pagesJavier, Jomar A. BSN121 Group 83 Nursing Care Plan (Pediatric Patient)Julie AnnNo ratings yet
- Pharmacology m7 Post Task CaparasDocument3 pagesPharmacology m7 Post Task CaparasGretta CaparasNo ratings yet
- Case Study, Chapter 42, Management of Patients With Musculoskeletal TraumaDocument2 pagesCase Study, Chapter 42, Management of Patients With Musculoskeletal TraumaAhmad BaolayyanNo ratings yet
- Drug PepcidDocument2 pagesDrug PepcidSrkocher0% (1)
- Young InfantDocument69 pagesYoung InfantAurora Doris BatagaNo ratings yet
- Post-Operative Nutrition: Things You Need To Know AboutDocument2 pagesPost-Operative Nutrition: Things You Need To Know AboutJannen Casas100% (1)
- Drugs Study For Surgery WardDocument4 pagesDrugs Study For Surgery WardMariquita BuenafeNo ratings yet
- Drug StudyDocument33 pagesDrug Studyjefwy8No ratings yet
- NCP Impaired Physical MobilityDocument1 pageNCP Impaired Physical MobilityLorraine Punla PanganNo ratings yet
- San Francisco St. Butuan City 8600, Region XIII Caraga, PhilippinesDocument3 pagesSan Francisco St. Butuan City 8600, Region XIII Caraga, Philippineskuro hanabusaNo ratings yet
- Placino HIRSCHPRUNG DX PDFDocument15 pagesPlacino HIRSCHPRUNG DX PDFSiena PlacinoNo ratings yet
- Lack of Insulin Decreases Available Glucose For CellDocument1 pageLack of Insulin Decreases Available Glucose For CellvicenteturasNo ratings yet
- IbuprofenDocument2 pagesIbuprofenKate AbadNo ratings yet
- Drugs StudyDocument6 pagesDrugs StudyMark_Rebibis_8528No ratings yet
- Nursing Care Plan (NCP) For SchizophreniformDocument8 pagesNursing Care Plan (NCP) For SchizophreniformRisa Sol AriasNo ratings yet
- Preterm Labor Prevention of DeliveryDocument10 pagesPreterm Labor Prevention of Deliverynursereview100% (1)
- The Ride of Your Life: What I Learned about God, Love, and Adventure by Teaching My Son to Ride a BikeFrom EverandThe Ride of Your Life: What I Learned about God, Love, and Adventure by Teaching My Son to Ride a BikeRating: 4.5 out of 5 stars4.5/5 (2)
- Alberta Infant Motor Scale (AIMS) - A Clinical Refresher and Update On Evaluation of Normative DataDocument8 pagesAlberta Infant Motor Scale (AIMS) - A Clinical Refresher and Update On Evaluation of Normative DataCamila AlmeidaNo ratings yet
- Pertinent Papers For Fidelity Bond (SY 2020-2021) : Department of EducationDocument7 pagesPertinent Papers For Fidelity Bond (SY 2020-2021) : Department of EducationGregor Chio Jr.No ratings yet
- Position PaperDocument3 pagesPosition Paperapi-385384164No ratings yet
- 1349072656CV Dr. Shaheen N KhanDocument17 pages1349072656CV Dr. Shaheen N KhanTanveer Abbas JafriNo ratings yet
- Technical Rescue Program: Development ManualDocument252 pagesTechnical Rescue Program: Development Manualscoutscathox100% (2)
- Ethics Bush 2005 CasebookDocument27 pagesEthics Bush 2005 CasebookSFMultiservice -No ratings yet
- GSIS V PauigDocument4 pagesGSIS V PauigLovely CondeNo ratings yet
- Ethical Paper Senior SemDocument6 pagesEthical Paper Senior Semapi-643481686No ratings yet
- Omicron Webinar AHSDocument16 pagesOmicron Webinar AHSDian AkbariNo ratings yet
- Green Party Platform 2011Document12 pagesGreen Party Platform 2011chorgsNo ratings yet
- Sample Drug-And-Alcohol-Evaluations-ExampleDocument3 pagesSample Drug-And-Alcohol-Evaluations-ExampleasksundaydealsNo ratings yet
- Manajemen Surveilans Covid-19 Di Wilayah Kerja Bandar Udara Internasional Hang NadimDocument9 pagesManajemen Surveilans Covid-19 Di Wilayah Kerja Bandar Udara Internasional Hang NadimClaudia PataloNo ratings yet
- DLL - Mapeh 6 - Q1 - W1Document4 pagesDLL - Mapeh 6 - Q1 - W1Laine Agustin SalemNo ratings yet
- Construction Method StatementDocument35 pagesConstruction Method StatementHoang ThiNo ratings yet
- Sindrome de Pies UrentesDocument4 pagesSindrome de Pies UrentesIdelberto Torres BenitezNo ratings yet
- NG Sample v6.2Document18 pagesNG Sample v6.2pedro.medina.riosNo ratings yet
- Biopsychosocial ApproachDocument4 pagesBiopsychosocial ApproachUnknown WandererNo ratings yet
- Get The Expectant Father 5th Edition Jennifer Ash Rudick PDF ebook with Full Chapters NowDocument52 pagesGet The Expectant Father 5th Edition Jennifer Ash Rudick PDF ebook with Full Chapters Nowsuyaniewudzi100% (1)
- Maternal and Child Health Nursing (MCN 107) : Joel D. Federico, RN, MAN InstructorDocument28 pagesMaternal and Child Health Nursing (MCN 107) : Joel D. Federico, RN, MAN InstructorJesz E GarciaNo ratings yet
- Perdosri MukernasDocument26 pagesPerdosri MukernasMad MadNo ratings yet
- Shine Medical Technologies PitchBook Company ProfileDocument17 pagesShine Medical Technologies PitchBook Company ProfileJeff BuchananNo ratings yet
- 10.3job Hazard Analysis Worksheet-001Document9 pages10.3job Hazard Analysis Worksheet-001alsakhaa.serviceNo ratings yet
- 2.0 Drug Statistics and TrendsDocument108 pages2.0 Drug Statistics and TrendsAnkita Kaliraman100% (1)
- 5 Sciatica Exercises For Pain Relief (With Pictures) : Back IntelligenceDocument26 pages5 Sciatica Exercises For Pain Relief (With Pictures) : Back Intelligenceanand sahu100% (1)
- Inspeccion Tecnica Edificios.20121016.002759Document2 pagesInspeccion Tecnica Edificios.20121016.002759anon_803524693No ratings yet
- Running Head: Mental Illness As A Cause of Homelessness 1Document12 pagesRunning Head: Mental Illness As A Cause of Homelessness 1api-286680238No ratings yet
- Liberty Quarry DeniedDocument33 pagesLiberty Quarry DeniedThe Press-Enterprise / pressenterprise.comNo ratings yet
- Echinacea: Research ArticleDocument10 pagesEchinacea: Research Articlenadin nNo ratings yet