CSF is produced in the brain's ventricles and normally flows and is absorbed through a series of connections between ventricles. Hydrocephalus occurs when there is excess CSF in the ventricles due to blocked flow or absorption. Common symptoms include headache, nausea, vision issues, and cognitive or motor problems. Treatment involves surgically inserting a shunt to drain CSF from the brain ventricles into the stomach or other areas of the body where it can be reabsorbed.
Copyright:
Attribution Non-Commercial (BY-NC)
Available Formats
Download as DOCX, PDF, TXT or read online from Scribd
CSF is produced in the brain's ventricles and normally flows and is absorbed through a series of connections between ventricles. Hydrocephalus occurs when there is excess CSF in the ventricles due to blocked flow or absorption. Common symptoms include headache, nausea, vision issues, and cognitive or motor problems. Treatment involves surgically inserting a shunt to drain CSF from the brain ventricles into the stomach or other areas of the body where it can be reabsorbed.
CSF is produced in the brain's ventricles and normally flows and is absorbed through a series of connections between ventricles. Hydrocephalus occurs when there is excess CSF in the ventricles due to blocked flow or absorption. Common symptoms include headache, nausea, vision issues, and cognitive or motor problems. Treatment involves surgically inserting a shunt to drain CSF from the brain ventricles into the stomach or other areas of the body where it can be reabsorbed.
Copyright:
Attribution Non-Commercial (BY-NC)
Available Formats
Download as DOCX, PDF, TXT or read online from Scribd
CSF is produced in the brain's ventricles and normally flows and is absorbed through a series of connections between ventricles. Hydrocephalus occurs when there is excess CSF in the ventricles due to blocked flow or absorption. Common symptoms include headache, nausea, vision issues, and cognitive or motor problems. Treatment involves surgically inserting a shunt to drain CSF from the brain ventricles into the stomach or other areas of the body where it can be reabsorbed.
Copyright:
Attribution Non-Commercial (BY-NC)
Available Formats
Download as DOCX, PDF, TXT or read online from Scribd
Download as docx, pdf, or txt
You are on page 1/ 4
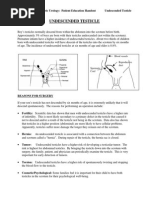
Pathophysiology The primary site of CSF formation is believed to be the choroid plexusus of the lateral ventricles.
CSF flows from the lateral ventricles through the foramen of Monro to the third ventricle, then through the aqueduct of Sylvius into the fourth ventricle through the foramen of Luschka and the midline foramen of Magendie into the cisterna magna. From there it flows to the cerebral and cerebellar subarachnoid spaces where ti is absorbed.
Introduction Hydrocephalus, also known as "water in the brain," is a medical condition in which there is an abnormal accumulation of cerebrospinal fluid (CSF) in the ventricles, or cavities, of the brain. This may cause increased intracranial pressure inside the skull and progressive enlargement of the head, convulsion, tunnel vision, and mental disability. Hydrocephalus can also cause death. The name derives from the Greek words - (hudro-) "water", and (kephalos) "head". Signs and symptoms
The clinical presentation of hydrocephalus varies with chronicity. Acute dilatation of the ventricular system is more likely to manifest with the nonspecific signs and symptoms of increased intracranial pressure. By contrast chronic dilatation (especially in the elderly population) may have a more insidious onset presenting, for instance, with Hakim's triad (Adams triad). Symptoms of increased intracranial pressure may include headaches, vomiting, nausea, papilledema, sleepiness or coma. Elevated intracranial pressure may result in uncal and/or cerebellar tonsill herniation, with resulting life threatening brain stem compression. Hakim's triad of gait instability, urinary incontinence and dementia is a relatively typical manifestation of the distinct entity normal pressure hydrocephalus (NPH). Focal neurological deficits may also occur, such as abducens nerve palsy and vertical gaze palsy (Parinaud syndrome due to compression of the quadrigeminal plate, where the neural centers coordinating the conjugated vertical eye movement are located). The symptoms depend on the cause of the blockage, the person's age, and how much brain tissue has been damaged by the swelling. In infants with hydrocephalus, CSF builds up in the central nervous system, causing the fontanelle (soft spot) to bulge and the head to be larger than expected. Early symptoms may also include:
Eyes that appear to gaze downward (Sundowning) Irritability Seizures Separated sutures Sleepiness
Vomiting
Symptoms that may occur in older children can include:
Brief, shrill, high-pitched cry Changes in personality, memory, or the ability to reason or think Changes in facial appearance and eye spacing Crossed eyes or uncontrolled eye movements Difficulty feeding Excessive sleepiness Headache Irritability, poor temper control Loss of bladder control (urinary incontinence) Loss of coordination and trouble walking Muscle spasticity (spasm) Slow growth (child 05 years) Slow or restricted movement Vomiting [1]
Communicating Communicating hydrocephalus, also known as non-obstructive hydrocephalus, is caused by impaired cerebrospinal fluid resorption in the absence of any CSF-flow obstruction between the ventricles and subarachnoid space. It has been theorized that this is due to functional impairment of the arachnoidal granulations (also called arachnoid granulations or Pacchioni's granulations), which are located along the superior sagittal sinus and is the site of cerebrospinal fluid resorption back into the venous system. Various neurologic conditions may result in communicating hydrocephalus, including subarachnoid/intraventricular hemorrhage, meningitis and congenital absence of arachnoid villi. Scarring and fibrosis of the subarachnoid space following infectious, inflammatory, or hemorrhagic events can also prevent resorption of CSF, causing diffuse ventricular dilatation.
Normal pressure hydrocephalus (NPH) is a particular form of communicating hydrocephalus, characterized by enlarged cerebral ventricles, with only intermittently elevated cerebrospinal fluid pressure. The diagnosis of NPH can be established only with the help of continuous intraventricular pressure recordings (over 24 hours or even longer), since more often than not instant measurements yield normal pressure values. Dynamic compliance studies may be also helpful. Altered compliance (elasticity) of the ventricular walls, as well as increased viscosity of the cerebrospinal fluid, may play a role in the pathogenesis of normal pressure hydrocephalus.
Main article: normal pressure hydrocephalus
Hydrocephalus ex vacuo also refers to an enlargement of cerebral ventricles and subarachnoid spaces, and is usually due to brain atrophy (as it occurs in dementias), post-traumatic brain injuries and even in some psychiatric disorders, such as
schizophrenia. As opposed to hydrocephalus, this is a compensatory enlargement of the CSF-spaces in response to brain parenchyma loss - it is not the result of increased CSF pressure.
Non-communicating Non-communicating hydrocephalus, or obstructive hydrocephalus, is caused by a CSF-flow obstruction ultimately preventing CSF from flowing into the subarachnoid space (either due to external compression or intraventricular mass lesions).
Foramen of Monro obstruction may lead to dilation of one or, if large enough (e.g., in Colloid cyst), both lateral ventricles. The aqueduct of Sylvius, normally narrow to begin with, may be obstructed by a number of genetically or acquired lesions (e.g., atresia, ependymitis, hemorrhage, tumor) and lead to dilation of both lateral ventricles as well as the third ventricle. Fourth ventricle obstruction will lead to dilatation of the aqueduct as well as the lateral and third ventricles (e.g., Chiari malformation). The foramina of Luschka and foramen of Magendie may be obstructed due to congenital failure of opening (e.g., Dandy-Walker malformation).
Congenital Main articles: Arnold-Chiari malformation and Dandy-Walker malformation The cranial bones fuse by the end of the third year of life. For head enlargement to occur, hydrocephalus must occur before then. The causes are usually genetic but can also be acquired and usually occur within the first few months of life, which include 1) intraventricular matrix hemorrhages in premature infants, 2) infections, 3) type II Arnold-Chiari malformation, 4) aqueduct atresia and stenosis, and 5) Dandy-Walker malformation. In newborns and toddlers with hydrocephalus, the head circumference is enlarged rapidly and soon surpasses the 97th percentile. Since the skull bones have not yet firmly joined together, bulging, firm anterior and posterior fontanelles may be present even when the patient is in an upright position. The infant exhibits fretfulness, poor feeding, and frequent vomiting. As the hydrocephalus progresses, torpor sets in, and the infant shows lack of interest in his surroundings. Later on, the upper eyelids become retracted and the eyes are turned downwards (due to hydrocephalic pressure on the mesencephalic tegmentum and paralysis of upward gaze). Movements become weak and the arms may become tremulous. Papilledema is absent but there may be reduction of vision. The head becomes so enlarged that the child may eventually be bedridden. About 80-90% of fetuses or newborn infants with spina bifidaoften associated with meningocele or myelomeningoceledevelop hydrocephalus.
Effects Because hydrocephalus can injure the brain, thought and behavior may be adversely affected. Learning disabilities including short-term memory loss are common among those with hydrocephalus, who tend to score better on verbal IQ than on performance IQ, which is thought to reflect the distribution of nerve damage to the brain. However the severity of hydrocephalus can differ considerably between individuals and some are of average or above-average intelligence. Someone with hydrocephalus may have motion and visual problems, problems with coordination, or may be clumsy. They may reach puberty earlier than the average child (see precocious puberty). About one in four develops epilepsy.
Treatment Hydrocephalus treatment is surgical, generally creating various types of cerebral shunts. It involves the placement of a ventricular catheter (a tube made of silastic), into the cerebral ventricles to bypass the flow obstruction/malfunctioning arachnoidal granulations and drain the excess fluid into other body cavities, from where it can be resorbed. Most shunts drain the fluid into the peritoneal cavity (ventriculo-peritoneal shunt), but alternative sites include the right atrium (ventriculo-atrial shunt), pleural cavity (ventriculo-pleural shunt), and gallbladder. A shunt system can also be placed in the lumbar space of the spine and have the CSF redirected to the peritoneal cavity (Lumbar-peritoneal shunt). An alternative treatment for obstructive hydrocephalus in selected patients is the endoscopic third ventriculostomy (ETV), whereby a surgically created opening in the floor of the third ventricle allows the CSF to flow directly to the basal cisterns, thereby shortcutting any obstruction, as in aqueductal stenosis. This may or may not be appropriate based on individual anatomy. This is the treatment.