Skeletal System1 241
Skeletal System1 241
Download as pptx, pdf, or txt
You might also like
- Major Themes of Ethio Poetry in English Tewodros Bogale TeferiDocument120 pagesMajor Themes of Ethio Poetry in English Tewodros Bogale Teferibela2011No ratings yet
- Acog Practice Bullet In: Management of Alloimmunization During PregnancyDocument9 pagesAcog Practice Bullet In: Management of Alloimmunization During PregnancyGeos KarNo ratings yet
- AnatomyDocument105 pagesAnatomyHelena Pascual PérezNo ratings yet
- Anaphy Chap 6Document38 pagesAnaphy Chap 6biancamariedejesusNo ratings yet
- Bone Tissue24Document79 pagesBone Tissue24JuhiJahan AmanullahNo ratings yet
- APP M1 The Skeletal SystemDocument9 pagesAPP M1 The Skeletal SystemZach TurnoNo ratings yet
- Bone Tissue and The Skeletal SystemDocument10 pagesBone Tissue and The Skeletal SystemUloko ChristopherNo ratings yet
- Skeletal System: Bones and Bone TissueDocument49 pagesSkeletal System: Bones and Bone TissueSumit100% (1)
- bone final 2Document78 pagesbone final 2pratyushanan325No ratings yet
- Lecture 6 Part 1Document185 pagesLecture 6 Part 1destin8y8No ratings yet
- (Manzanares) Skeletal System Study GuideDocument17 pages(Manzanares) Skeletal System Study GuideKyla ManzanaresNo ratings yet
- THE Skeletal System: A T E A MDocument27 pagesTHE Skeletal System: A T E A MMiss medNo ratings yet
- Bone-LDocument34 pagesBone-LurjaNo ratings yet
- Skeletal SystemDocument104 pagesSkeletal Systemsyafi zulNo ratings yet
- BonesDocument210 pagesBonesreynaldojavier66No ratings yet
- Skeletal System: - Composed of The Body's Bones and Associated Ligaments, Tendons, and Cartilages. - FunctionsDocument66 pagesSkeletal System: - Composed of The Body's Bones and Associated Ligaments, Tendons, and Cartilages. - FunctionsDenver TanhuanNo ratings yet
- Chapter 6 Osseous Tissue and Skeletal StructureDocument70 pagesChapter 6 Osseous Tissue and Skeletal StructureStefanie Henry100% (2)
- Chapter 6 Skeletal SystemDocument212 pagesChapter 6 Skeletal SystemMaine CarandangNo ratings yet
- BoneDocument19 pagesBoneSamyog ChaliseNo ratings yet
- Biol 111-Bones and Skeletal Tissue Part 1Document58 pagesBiol 111-Bones and Skeletal Tissue Part 1Jaedon AdamsNo ratings yet
- Bone TissueDocument66 pagesBone TissueFunikawati Baldiyah100% (1)
- 2 - HumanmovementsystemDocument44 pages2 - HumanmovementsystemLorence Mae MirandaNo ratings yet
- The Skeletal System:: Structure and Function of The BonesDocument10 pagesThe Skeletal System:: Structure and Function of The BonesSodoo BayarsaikhanNo ratings yet
- Biol 2401 21251 Lecture Exam N 2 Updated Study GuideDocument8 pagesBiol 2401 21251 Lecture Exam N 2 Updated Study GuidedeehteeNo ratings yet
- General Anatomy 3 Ann-2021Document104 pagesGeneral Anatomy 3 Ann-2021jb5463275No ratings yet
- 11 LS SkeletonDocument45 pages11 LS SkeletonAdhi PandayNo ratings yet
- Musculoskeletal System-Topic 8Document40 pagesMusculoskeletal System-Topic 8Heba TabchNo ratings yet
- Cartilage and BoneDocument54 pagesCartilage and BoneAGolosinoNo ratings yet
- Anaphy Notes MidtermDocument17 pagesAnaphy Notes MidtermCabello Katelyn C.No ratings yet
- 6 SkeletalDocument14 pages6 SkeletalprincessstephNo ratings yet
- Presentation 14 Skeletal SystemDocument14 pagesPresentation 14 Skeletal SystemJeff Bryan Arellano HimorNo ratings yet
- Relationship To Other Organ SystemsDocument11 pagesRelationship To Other Organ SystemsVern NuquiNo ratings yet
- Skeletal SystemDocument39 pagesSkeletal SystemDASHNo ratings yet
- Cartilage and Bone Tissue BSHB 2014 NewDocument65 pagesCartilage and Bone Tissue BSHB 2014 NewRizky Bayu LesmanaNo ratings yet
- Osteo Intro FinalDocument33 pagesOsteo Intro Finaljjjayakrishnan70No ratings yet
- Module 6A - Histology and Physiology of BonesDocument50 pagesModule 6A - Histology and Physiology of BonesMa. Andrea B. PALOMONo ratings yet
- Bone Tissues and The Skeletal System: Jahangir Moini, MD, MPHDocument108 pagesBone Tissues and The Skeletal System: Jahangir Moini, MD, MPHAngella CharlesNo ratings yet
- Chapter 6 Bones and Bone Structure 24Document44 pagesChapter 6 Bones and Bone Structure 24m4ghmfj7d2No ratings yet
- Anatomy and Physiology - The Skeletal SystemDocument20 pagesAnatomy and Physiology - The Skeletal Systemxuxi dulNo ratings yet
- Skeletal SystemDocument65 pagesSkeletal SystemRo'Zie SylvesterNo ratings yet
- Haversian System (Osteon) : Basic Structural UnitDocument7 pagesHaversian System (Osteon) : Basic Structural UnitJulius Matthew MarananNo ratings yet
- MIDTERMS AnatomyDocument6 pagesMIDTERMS AnatomyCHIKA IN A MINUTENo ratings yet
- Chapter 6 Bone Tissue 2304Document37 pagesChapter 6 Bone Tissue 2304Sav Oli100% (1)
- 6. Bone HistologyDocument25 pages6. Bone Histologyhaseebimtiaz829No ratings yet
- Unit 3.1 - Skeltal System: Functions of The BonesDocument4 pagesUnit 3.1 - Skeltal System: Functions of The BonesEricBuguinaNo ratings yet
- Ch. 6 - Osseous Tissue Bone StructureDocument54 pagesCh. 6 - Osseous Tissue Bone StructureHilary OliverioNo ratings yet
- Chapter 7 & 8 Notes - A&PDocument8 pagesChapter 7 & 8 Notes - A&PAshley MarieNo ratings yet
- Chapter 6 ANAPHY Skeletal SystemDocument6 pagesChapter 6 ANAPHY Skeletal Systemrobh0026No ratings yet
- OSSEOUS TISSUE AND BONE STRUCTURE-ch 6Document7 pagesOSSEOUS TISSUE AND BONE STRUCTURE-ch 6Joshua RubinsteinNo ratings yet
- (BioSci Lec) Chapter 6Document13 pages(BioSci Lec) Chapter 6Jemille Anne Maranan MoroñaNo ratings yet
- Bones, Joints, and CartilageDocument11 pagesBones, Joints, and CartilageClaresta JaniceNo ratings yet
- Human Skeletal SystemDocument106 pagesHuman Skeletal SystemNirasha KodituwakkuNo ratings yet
- Introduction To Skeletal 1Document196 pagesIntroduction To Skeletal 1Earl TrinidadNo ratings yet
- Skeletal SystemDocument7 pagesSkeletal SystemFranchezka YsabelNo ratings yet
- Skeletal System Types of Bone Tissue: Phosphorus)Document10 pagesSkeletal System Types of Bone Tissue: Phosphorus)Arthea DavidNo ratings yet
- Lecture 2 BoneDocument22 pagesLecture 2 BoneiamkpvemuriNo ratings yet
- Osteoarthritis and Joint Diseases 2023Document29 pagesOsteoarthritis and Joint Diseases 2023Abdullah MelhimNo ratings yet
- Axial SkeletonDocument69 pagesAxial SkeletonMaisNo ratings yet
- Anatomy and Physiology: Bone Histology Lecture OutlineDocument42 pagesAnatomy and Physiology: Bone Histology Lecture OutlineFokeerbux Zyad100% (1)
- Advanced farriery knowledge: A study guide and AWCF theory course companionFrom EverandAdvanced farriery knowledge: A study guide and AWCF theory course companionNo ratings yet
- New Criticism and FormalismDocument25 pagesNew Criticism and Formalismbela201178% (9)
- Major Trends of Literary Development (Literary Periods/Movements)Document26 pagesMajor Trends of Literary Development (Literary Periods/Movements)bela2011100% (1)
- Medieval Literary CriticismDocument10 pagesMedieval Literary Criticismbela2011No ratings yet
- Reader Response Criticism NewDocument9 pagesReader Response Criticism Newbela2011No ratings yet
- Feminist Literary CriticismDocument11 pagesFeminist Literary Criticismbela2011No ratings yet
- Presentation2 Oral Literature 2Document7 pagesPresentation2 Oral Literature 2bela2011100% (1)
- Types of Poetry-UpdatedDocument31 pagesTypes of Poetry-Updatedbela2011No ratings yet
- Unit 1 Fundamentals of Literature: Definition of Basic ConceptsDocument24 pagesUnit 1 Fundamentals of Literature: Definition of Basic Conceptsbela201188% (8)
- Fundamentals of Literature Oral LiteratureDocument13 pagesFundamentals of Literature Oral Literaturebela2011100% (1)
- 1.3 Why Study LiteratureDocument17 pages1.3 Why Study Literaturebela2011No ratings yet
- 1.2 Unique Features or Characteristics of LiteratureDocument10 pages1.2 Unique Features or Characteristics of Literaturebela201178% (9)
- 2hematology ExaminationDocument4 pages2hematology ExaminationAmparo BailonNo ratings yet
- (Lesson 10-1) - Quality Assurance, Hemocytometry, Thoma PipetsDocument22 pages(Lesson 10-1) - Quality Assurance, Hemocytometry, Thoma PipetselleNo ratings yet
- Exercise 3 RBC CountDocument6 pagesExercise 3 RBC CountJohn Paul Dian100% (1)
- Tutorial: Section A: Multiple Choice Question (Mcqs T/F)Document7 pagesTutorial: Section A: Multiple Choice Question (Mcqs T/F)Harith AsriNo ratings yet
- Wa0007.Document2 pagesWa0007.endapallikartheeNo ratings yet
- Cross Match TechniqueDocument5 pagesCross Match TechniqueANDREW MWITI100% (3)
- Introduction To Hematology 2Document39 pagesIntroduction To Hematology 2irishgopez24No ratings yet
- Blood Grouping 3X10 ML: Intended UseDocument5 pagesBlood Grouping 3X10 ML: Intended Useshirsenduhaldar4No ratings yet
- How To Use A Haemostat (Celox Range)Document30 pagesHow To Use A Haemostat (Celox Range)drfabriciofigueiredoNo ratings yet
- Deep Vein Thrombosis DissertationDocument7 pagesDeep Vein Thrombosis DissertationPaperWriterUK100% (2)
- 267 812 1 PBDocument9 pages267 812 1 PBKenari XeiNo ratings yet
- Hematology PDFDocument11 pagesHematology PDFMaybelline Tan100% (1)
- Platlets DisorderDocument177 pagesPlatlets DisorderFatimah A Al-dawoodNo ratings yet
- Lec1 - PlateletsDocument26 pagesLec1 - PlateletsClaire GonoNo ratings yet
- Antiphospholipid Antibody SyndromeDocument37 pagesAntiphospholipid Antibody SyndromeAhmad Reshad AslamNo ratings yet
- Haemostatic Support in Postpartum Haemorrhage A.5Document10 pagesHaemostatic Support in Postpartum Haemorrhage A.5Sonia Loza MendozaNo ratings yet
- Class Ix Biology TissueDocument3 pagesClass Ix Biology TissueAnushka ManatwalNo ratings yet
- Narrative Report - NSTP 2nd Sem Chapter 3Document1 pageNarrative Report - NSTP 2nd Sem Chapter 3Clint Kove YtemNo ratings yet
- Rheology of Leukocytes, Leukocyte Suspensions and Blood in LeukemiaDocument9 pagesRheology of Leukocytes, Leukocyte Suspensions and Blood in Leukemiaashgee1No ratings yet
- HistologyDocument65 pagesHistologyAlliana FlorenzaNo ratings yet
- Blood TypesDocument2 pagesBlood TypesPRINTDESK by DanNo ratings yet
- Describe The Principles of Blood Cell MaturationDocument11 pagesDescribe The Principles of Blood Cell MaturationnotsoninjaninjaNo ratings yet
- Chapter 6Document10 pagesChapter 6neil092904No ratings yet
- ABC Blood Letting InvitationDocument2 pagesABC Blood Letting InvitationKeeshia Tenise BadillesNo ratings yet
- Nerve Cell PPT 1Document16 pagesNerve Cell PPT 1Zhen ObelidorNo ratings yet
- Blood Transfusion - Hatem AlsrourDocument18 pagesBlood Transfusion - Hatem Alsrourhatem alsrour100% (2)
- Chapter 42Document3 pagesChapter 42Soc Gerren TuasonNo ratings yet
- Chapter 6 Bone Tissue 2304Document37 pagesChapter 6 Bone Tissue 2304Sav Oli100% (1)
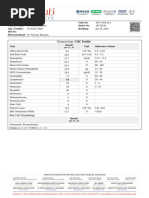
- Haematology - CBC ProfileDocument1 pageHaematology - CBC ProfileShaheer JamalNo ratings yet