DOI:http://dx.doi.org/10.7314/APJCP.2015.16.16.7077
Do Human Papilloma Viruses Play Any Role in Oral Squamous Cell Carcinoma in North Indians?
RESEARCH ARTICLE
Do Human Papilloma Viruses Play Any Role in Oral Squamous
Cell Carcinoma in North Indians?
Vineeta Singh1,3, Nuzhat Husain1*, Naseem Akhtar2, Vijay Kumar2, Shikha
Tewari1, Sridhar Mishra1, Sanjeev Misra2, M.Y. Khan3
Abstract
Background: Oral squamous cell carcinoma (OSCC) is the most prevalent malignancy among males in
India. While tobacco and alcohol are main aetiological factors, human papilloma virus (HPV) presence has
surprisingly increased in head and neck Squamous Cell Carcinoma (HNSCC) in the past two decade but its
frequency in OSCCS is still uncertain. We aim to explore the frequency of HPV and its major genotypes in North
Indian patients and their association with clinicopathological and histopathological features and p16 expression
pattern. Materials and Methods: The study group comprised 250 histologically proven cases of OSCC. HPV
was detected by real time PCR in tumor biopsy specimens and confirmed by conventional PCR with PGMY09/
PGMY11 primers. Genotyping for high-risk types 16/ 18 was conducted by type specific PCR. p16 expression
was assessed by immunohistochemsitry. Results: HPV presence was confirmed in 23/250 (9.2%) OSCC cases, of
which 30.4% had HPV 16 infection, 17.4%were positive for HPV 18 and 26.1% had co-infections. HPV presence
was significantly associated with male gender (p=0.02) and habit of pan masala chewing (p=0.01). HPV positive
cases also had a history of tobacco consumption in 91.3% cases. p16 over expression was observed in 39.1%
of HPV positive cases but this was not significantly different from negative cases (p=0.54). Conclusions: The
frequency of HPV in OSCC is low in North-India and majority of cases are associated with a tobacco habit.
It appears that tobacco shows a confounding effect in HPV positive cases and use of p16 protein as a reliable
marker to assess the potential etiological role of HPV in OSCC in our population is not suggested.
Keywords: Oral squamous cell carcinoma - human papilloma virus - p16 - head & neck squamous cell carcinoma.
Asian Pac J Cancer Prev, 16 (16), 7077-7084
Introduction
Oral squamous cell carcinoma (OSCC) is one of the
most prevalent malignancy in India with approximately
83,000 new cases and more than 46,000 deaths occur
yearly (Bray et al., 2013). It ranks number one in terms of
incidence among men and third among women (Byakodi
et al., 2012). According to Indian Council of Medical
Research there is a sharp increase in the number of oral
cancer cases by 2020 is expected.
In India 16% population smoke tobacco, 20%
chew tobacco/pan masala and 30% either smoke or
chew tobacco (Rani et al., 2003) and these are the well
established risk factors for OSCC. The relative risk for
OSCC among tobacco and alcohol abusers is 20 times that
of non-smokers and non-drinkers (Hashibe et al., 2009).
An increased involvement of human papilloma virus
(HPV) in the Head &Neck Squamous Cell Carcinoma
(HNSCC) has been reported in past 10 years (Chaturvedi
et al., 2008) but its presence is not as consistent in it as in
cervical cancer and therefore its actual prevalence is still
vague in HNSCC and need the more solemn attention of
researchers in this direction.
HPV is a DNA virus that presents tropism for epithelial
cells, causing infection of the skin and mucous membrane.
Its presence is more allied to oropharyngeal cancer for
instance about 40-80% of oropharyngeal cancers are
caused by HPV in USA, whereas in Europe the proportion
varies from around 90% in Sweden to less than 20% in
communities with the highest rates of tobacco use (Marur
et al., 2010).
The etiologic role of HPV in HNSCC sites other
than oropharynx is still controversial. In India a wide
variation in HPV associated OSCC has been reported,
for instance in Western India only 15% OSCC patients
showed association with HPV, 33.6% cases in Eastern
India while its prevalence is surprisingly higher (70.6
%) in South Indian population (Balaram et al., 1995;
D’Costa et al., 1998; Priya et al., 2005; Alok et al., 2006;
Chaudhary et al., 2013). These variations might be due
1
Department of Pathology, Dr. Ram Manohar Lohia Institute of Medical Sciences, 2Department of Surgical Oncology, King
George’s Medical University, 3Department of Biotechnology, Babasaheb Bhimrao Ambedkar University, Lucknow, UP, India *For
correspondence: drnuzhathusain@hotmail.com
Asian Pacific Journal of Cancer Prevention, Vol 16, 2015
7077
�Vineeta Singh et al
to sensitivity of the employed technique, the sample size,
the state of conservation of the clinical specimens, and
epidemiological factors of the studied population.
Apart from having a different epidemiology and
aetiology, the HPV-positive HNSCC are different clinicopathologically and showed distinct histopathology. These
are usually poorly differentiated, nonkeratinizing and have
a basaloid appearance (Gillison et al., 2000). Furthermore,
patients with HPV-positive HNSCC in general tend to
be younger at time of diagnosis (Smith et al., 2004) and
generally have a better survival and favorable prognosis
compared to the HPV-negative patients (Hafkamp et al.,
2008; Lassen et al., 2009).
HPV positive oral cancer also represents a distinct
molecular phenotype with a unique mechanism of
tumorigenesis, independent of the mutagenic effect of
tobacco and alcohol. A characteristic over expression of
p16, tumor suppressor protein, has been observed in HPV
positive HNSCC. Two viral onco-proteins E6 and E7 cause
inactivation of p53 and retinoblastoma (Rb) respectively,
this event leads further activation of CDKN2A gene and
increased expression of p16 has occurred. Thus, p16 overexpression is an indicator of an aberrant expression of
viral oncogenes and considered as a surrogate biomarker
for HPV presence (Klussmann et al., 2009; Ahmed et
al., 2012).
Therefore, the present study aims to explore the
frequency of HPV association in OSCC, distribution of
its major high risk types and correlation with other risk
factors in North Indian population.
Materials and Methods
Study Population: A total of 250 clinically and
histologically proven cases of OSCC were included
prospectively in the study between Oct 2013 to Jan
2015. Tissue biopsies were collected from department of
Surgical Oncology, King George’s Medical University
(KGMU) Lucknow after obtaining approval from the
Institutional Ethics Committee and written informed
consent from the patients.
Sample Collection: Tissue biopsies were collected
in 10% buffered formalin at RT for histopathological
diagnosis and in 1X phosphate buffer saline (PBS, pH
7.4) and stored at -80°C for molecular analysis. The
demographic and clinical details of the patients were
recorded on the standard questionnaire.
DNA Extraction: The DNA from biopsy tissues was
isolated by commercially available Genomic DNA Mini
kit (Invitrogen, USA) as per manufacturer’s instructions.
The extracted DNA was eluted in 80μl of the elution buffer
(provided in the kit) and kept at -80°C until further use.
All the DNA samples were qualitatively confirmed on
0.8% agarose gel electrophoresis and the concentration
and purity was checked by DS-11 spectrophotometer
(Denovix, USA) at 260/280 nm wavelengths.
HPV detection: HPV detection was performed by using
the following methodology
Real Time PCR based methodology for HPV detection:
Presence of HPV in OSCC samples were detected by Real
7078
Asian Pacific Journal of Cancer Prevention, Vol 16, 2015
time PCR (Biorad CFX 96TM) using 13 HIGH RISK HPV
REAL TIME PCR KIT (Hybribio Limited, China) as per
manufacturer’s instructions. Briefly, each PCR reaction
contained 17.5µl of PCR master mix, 0.5µl of Taq DNA
polymerase and 2µl of DNA. The PCR amplification
protocol was as follows- initial denaturation at 95°C for
10min and 45 cycles of - denaturation for 3min at 95°C,
annealing for 60sec at 60°C, and extension at 72°C for
20sec. The amplification was followed by a 5sec final
extension step at 38°C. Presence or absence of HPV DNA
was confirmed by the Ct values obtained for the sample.
Conventional PCR based methodology: Further
validation of HPV was done using PGMY09/11 primers
as reported by P.E.Gravitt et al; 2000, designed to amplify
a 450bp HPV L1 gene fragment. This region is used
because it is highly conserved between different HPV
types but has sufficient variation for the identification of
each one. Cervical cancer cases which were confirmed
previously for HPV presence were used as positive
control. PCR amplification was carried out in a volume
of 20μl containing 50ng/μl of genomic DNA, 4mM
of MgCl2 (Invitrogen, USA), 200µM of each dNTPs.
Concentration of PGMY09/11 primers was reduced
from 10pmol as previously used to 5pmol, also the final
concentration of AmpliTaq DNA polymerase (Invitrogen,
USA) was reduced from 7.5U/µl to 5U/µl. Amplification
was performed in thermal cycler (S100TM, Biorad, USA)
under the following conditions: initial denaturation
at 95ºC for 9min, followed by 35 cycles of - 95ºC for
1min (denaturation), primer annealing at 55°C for 1min,
extension at 72ºC for 1min and a final extension at
72ºC for 5min. Positive and negative controls were run
simultaneously.
HPV genotyping: Samples that were positive for
HPV presence were proceeded further for high risk
HPV 16 & 18 genotyping. HPV genotyping was done
with the previously described type specific primers for
HPV 16 and 18 (Sharma et al., 2005). PCR amplification
was carried out in a 20μl reaction volume containing
50ng/μl of genomic DNA, 10pmol each of forward and
reverse primer, 2mM MgCl2 (Invitrogen, USA), 200µM
of each dNTPs, 0.5U/µl of AmpliTaq DNA polymerase
(Invitrogen, USA) along with 10X (NH4)2SO4 buffer
(Invitrogen, USA). Amplification was performed in
thermal cycler (S100TM, Biorad, USA) under the following
PCR conditions: An initial denaturation at 94ºC for
10min, followed by 35 cycles of 94ºC for 1min (cycle
denaturation), primer annealing at 52°C for 1min for
HPV 16 & 62°C for 1min for HPV 18, extension at 72ºC
for 1min and a final extension of 72ºC for 5min. PCR
products were confirmed for their respective amplicon
size on 2% agarose gel electrophoresis and visualized
by UV-transillumination (Gel Doc XR+ , Biorad, USA).
Expression of p16 by Immunohistochemsitry (IHC):
Paraffin-embedded tissues were sectioned, 4μm, using a
microtome (Leica, Germany), and transferred to tissue
bond-coated slides (Biocare, USA). After overnight
incubation in a 60°C dry oven, paraffin-embedded
sections were deparaffinized in xylene and rehydrated
through graded ethanol series 100%, 70% and 50%.
Endogenous peroxidase activity was blocked with 3%
�DOI:http://dx.doi.org/10.7314/APJCP.2015.16.16.7077
Do Human Papilloma Viruses Play Any Role in Oral Squamous Cell Carcinoma in North Indians?
hydrogen peroxide in methanol for 30min. Antigen
retrieval was done by placing the slides in Tris-EDTA
buffer (pH 9.0) in Pascal. These sections after cooling to
room temperature (RT) were incubated with p16 primary
antibody (Biogenex) at RT for one hour, followed by
treatment with polymer based secondary antibody kit
with DAB (DAKO, Denmark). Positive reactions were
visualized using diaminobenzidine, DAB (1:50). Sections
were finally counter-stained with 0.1% hematoxylin.
The positive cells expressing the p16 positivity were
assessed for cytoplasmic as well as nuclear staining at
higher magnification.A tumor was recorded positive if
more than 10% of tumor cells showed immunoreactivity
(Names et al., 2006).
Data analysis: The diagnostic criteria used for the
detection of HPV considered only those OSCC cases that
were positive by at least two methods described above
(Real time PCR, PCR, 16 PCR & 18 PCR). The real time
PCR data was analyzed using Bio-Rad CFX Manager
software v3.0. The results are presented in mean±SD and
percentages. The Chi-square test was used to compare the
dichotomous/categorical variables and unpaired t-test was
used to compare the continuous variables. The univariate
binary logistic regression was carried out to find the
strength of associations. The odds ratio with its confidence
interval was calculated. The p-value<0.05 was considered
significant. Kaplan-Meier survival curve was made and
survival time was compared by using Log rank test. All
the analysis was carried out by using SPSS 16.0 version
(Chicago, Inc., USA).
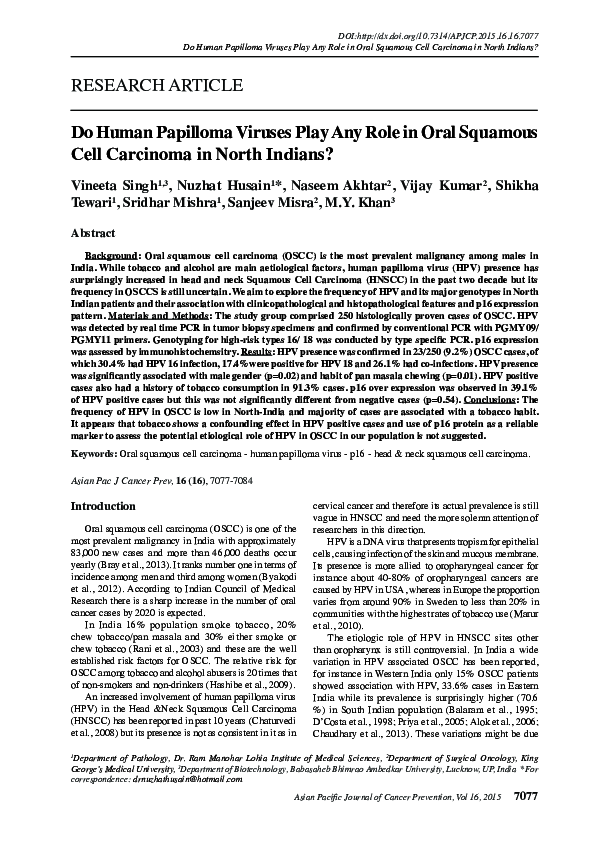
Figure 1. Detection of HPV by real time and
conventional PCR. (A) Amplification Plot by Real Time
PCR, (B) 2% Agarose gel with amplified product of HPV (450bp)
by PGMY09/11 primers-M: 100bp DNA ladder, L1: Positive
control, L2: Negative control, L3-L7: HPV in cases. (C) 2%
Agarose gel with amplified product of HPV 16 (223bp) M: 100bp
DNA ladder, L7: Positive control, L6: Negative control, L1-L5:
HPV 16 in cases. (D) 2% Agarose gel with amplified product of
HPV 18 (217bp) M: 100bp DNA ladder, L12: Positive control,
L13: Negative control, L1-L11: Samples
Results
The study encompasses 250 histologically proven
cases of OSCC. Out of these HPV presence was confirmed
in 23(9.2%) cases (Figure 1A&B) according to diagnostic
criteria predefined in data analysis. Table 1 summarizes the
clinical, histopathological, demographic and behavioral
characteristics of patients in HPV positive and negative
cases.
The mean age of HPV positive patients was 47.17
while HPV negative cases had mean age 47.69, but this
difference was statistically insignificant. HPV presence
associated significantly with male gender [p=0.02*,OR
(95%CI) =0.34 (0.13-0.83)]. Buccal Mucosa was the most
frequent site (52.2%) in patients. Most of HPV positive
cases were well differentiated SCC (60.9%), eight cases
were moderately differentiated or keratinized while only
4.3% cases showed a basaloid morphology (Figure 2A).
HPV positivity did not find to be associated with age,
marital status, domicile, sub-site, stage, tumor grade, nodal
status and outcome.
In HPV positive cases 91.3% had taken tobacco in
any form while only 8.7% patients had no history of any
risk factor. History of multiple risk factors was present
in 13.00% cases. HPV positivity significantly associated
with habit of pan masala chewing [p=0.01*,OR (95%CI)
= 0.32 (0.13-0.79)].
HPV subtypes in OSCC: Out of 23 HPV positive cases
30.4% cases had HPV 16 infection while 17.4% were
positive for HPV 18. Six cases (26.1%) co-expressed
Figure 2. Microphotograph showing. (A) Basaloid
morphology, (B) p16 expression in HPV positive cases (DAB
x 200 x digital magnification)
Figure 3. Kaplan-Meier survival curve of patients. (A)
According to HPV status, (B) According to HPV16 status,
(C) According to HPV18 status.
Asian Pacific Journal of Cancer Prevention, Vol 16, 2015
7079
�Vineeta Singh et al
Table 1. Association of HPV with Clinicopathological, Histopathological, Demographic and Behavioral
Characteristics in OSCC Patients
HPV
Characteristics
Positive
Negative
(n=23)
(n=227)
OR
95%CI
p -value1
No.
%
No.
%
<30
2
8.7
7
3.1
2.57
0.39-16.86
0.32
30-40
5
21.7
73
32.2
0.616
0.15-2.43
0.49
41-50
7
30.4
69
30.4
0.91
0.25-3.32
0.89
51-60
5
21.7
42
18.5
1.07
0.26-4.29
0.92
>60
4
17.4
36
15.9
1
Ref.
Male
14
60.9
186
81.9
0.34
0.13-0.83
Female
9
39.1
41
18.1
1
Ref.
Married
23
100
223
98.2
Unmarried
0
0
4
1.8
NA
NA
Age in years
Gender
0.02*
Marital status
Residence
Rural
16
69.6
159
70
0.97
0.38-2.48
Urban
7
30.4
68
30
1
Ref.
0.96
BM
12
52.2
115
50.7
0.99
0.35-2.77
FM
0
0
4
1.8
-
-
LA
4
17.4
40
17.6
0.95
0.25-3.58
0.94
Palate/Upper alveolus
0
0
6
2.6
-
-
0.58
Subsite
RMT
1
4.3
5
2.2
1.9
0.18-19.06
Tongue
6
26.1
57
25.1
1
Ref.
0.08
Site
Left
16
69.6
116
51.1
2.18
0.86-5.51
Right
7
30.4
111
48.9
1
Ref.
0.09
Stage
I
1
4.3
21
9.3
0.47
0.05-3.88
0.48
II
4
17.4
45
19.8
0.88
0.26-2.93
0.84
III
7
30.4
51
22.5
1.37
0.50-3.74
0.53
IV
11
47.8
110
48.5
1
Ref.
Yes
12
52.2
110
48.5
1.16
0.49-2.73
No
11
47.8
117
51.5
1
Ref.
Yes
8
34.8
141
62.1
0.32
0.13-0.79
No
15
65.2
86
37.9
1
Ref.
Yes
19
82.6
171
75.3
1.55
0.50-4.76
No
4
17.4
56
24.7
1
Ref.
Yes
7
30.4
66
29.1
1.06
0.42-2.71
No
16
69.6
161
70.9
1
Ref.
Smoking
0.73
Pan masala
0.01*
Tobacco
0.43
Alcohal
Multiple habit
7080
Asian Pacific Journal of Cancer Prevention, Vol 16, 2015
0.89
�DOI:http://dx.doi.org/10.7314/APJCP.2015.16.16.7077
Do Human Papilloma Viruses Play Any Role in Oral Squamous Cell Carcinoma in North Indians?
Present
3
13
30
13.2
0.98
0.27-3.51
Absent
20
87
197
86.8
1
Ref.
Any habit
21
91.3
212
93.4
0.74
0.15-3.47
No habit
2
8.7
15
6.6
1
Ref.
0.98
No habit
0.7
Treatment
ABS
0
0
3
1.3
-
CT
9
39.1
62
27.3
1.52
0.30-7.62
0.6
CT/RT
3
13
34
15
0.92
0.14-6.01
0.93
CT/SX/RT
2
8.7
31
13.7
0.67
0.08-5.19
0.7
SX
7
30.4
76
33.5
0.96
0.18-5.01
0.96
SX/RT
2
8.7
21
9.3
1
Ref.
WD
14
60.9
129
56.8
0.65
0.07-5.80
0.7
MD
8
34.8
92
40.5
0.52
0.05-4.88
0.56
PD
1
4.3
6
2.6
1
Ref.
Large
22
95.7
226
99.6
0.09
0.01-1.61
Basaloid
1
4.3
1
0.4
1
Ref.
Present
15
65.2
132
58.1
1.34
0.55-3.31
Absent
8
34.8
95
41.9
1
Ref.
Recurrence
1
9.1
9
7
1.33
0.15-11.61
No recurrence
10
90.9
120
93
1
Ref.
Dead
7
30.4
58
25.6
1.27
0.49-3.25
Alive
16
69.6
169
74.4
1
Ref.
Positive
9
39.1
7
30.4
1.46
0.43-4.9
Negative
14
60.9
16
69.6
1
Ref.
Differentiation
Cellular morphology
0.1
Node
0.51
Recurrence (n=140)
0.79
Survival
0.61
p16 Protein expression (n=23)
0.54
1 p value <0.05 by Binary logistic regression method.; Abbreviations: HPV- Human Papilloma Virus, OR-Odds Ratio, BM-Buccal Mucosa, FMfloor of Mouth, LA-Lower Alveolus, RMT-Retro Moral trigone, SX = Surgery, CT=Chemotherapy, CT/RT=Chemotherapy and Radiotherapy
both, SX/RT=Surgery and Radiotherapy both, CT/SX/RT=Chemotherapy, Surgery and Radiotherapy, WD- Well Differentiated, MD- Moderately
Differentiated, PD- Poorly Differentiated
Table 2. HPV Subtypes in OSCC Patients
HPV Result
HPV positive cases
HPV negative cases
HPV Types
HPV16 only
HPV18 only
HPV16 and 18 co-infection
Negative for HPV 16 /18 or suspected subtypes other than 16/18
No. of Patient
%
23
227
9.2
90.8
7
4
6
6
30.4
17.4
26.1
26.1
Abbreviation: HPV- Human Papilloma Virus
DNA of both HPV 16 and 18 subtypes and 26.1% cases
were negative for both 16 and 18 or supposed to had HPV
subtypes other than 16/18 (Table 2, Figure 1C& D).
Correlation of HPV 16 and 18 with clinicopathological
variables
Association of HPV type 16 & 18 with all clinical,
demographic & behavioral profile of patients were
evaluated but it was found to be shown no association
with any of these (data not shown).
Correlation of HPV with Survival of Patients
Asian Pacific Journal of Cancer Prevention, Vol 16, 2015
7081
�Vineeta Singh et al
Table 3. Association of Survival of Patients with HPV
Presence and Its Subtypes.
HPV Status
HPVa
Positive
Negative
Total cases
HPV16b
Positive
Negative
HPV18c
Positive
Negative
Median Survival in Month
16.5
12.9
15.6
14
12
13
14
Log Rank test ap=0.62, bp=0.68, cp=0.72 (Insignificant); Abbreviation:
HPV- Human Papilloma Virus
According to Log rank test median survival of HPV
positive patients was better (16.5) compared to HPV
negative patients (12.9) but the difference was not
significant (p=0.62) (Figure 3A, B & C). The survival
status of patients in the study is shown in Table 3.
Correlation of HPV with p16 protein expression
p16 expression was evaluated in all HPV positive
cases and equal number of HPV negative cases (n=23)
that were selected randomly. Diffuse nuclear staining with
some cytoplasmic positivity for p16 protein was seen in
39.13% HPV positive patients and 30.43% HPV negative
patients (Table 1, Figure 2B). p16 over expression was not
associated with the presence of HPV ( p=0.54).
Discussion
HPV has been identified as a prime suspect in the
etiology of HNSCC due to their morphological similarities
with genital epithelia and their ability to transform and
immortalize oral keratinocytes (Termine et al., 2008).
Speculation on the role of HPV in the etio-pathogenesis
of oral carcinoma has been voiced worldwide.We have
explored the frequency and major genotypes of HPV in
250 histologically confirmed cases of OSCC in NorthIndian population.
The overall prevalence of HPV associated OSCC at
worldwide level varies from 0-30%.In North America
5.9% positivity was reported by Mark W. Lingen., 2013,
in Canada 4% by Jarry Machado et al., 2010, 27.5% in
China by Li-Li Gan et al., 2014 and only 3% in Bangladesh
by Mahmuda Akhter et al., 2013.
Most Indian studies have reported prevalence of
HPV associated OSCC between 15-37.9% (Priya et al.,
2005; Alok et al., 2006; Chaudhary et al., 2013) with an
exception in southern India where higher prevalence of
HPV (70.6%) was reported (Kulkarni et al., 2011). Our
study is in concordance with previous studies and shows
that HPV was associated in 9.2% of OSCC cases with
HPV 16 showing higher (30.4%) prevalence than HPV 18
(17.47%). In one fourth of the cases it is not single subtype
which was present, but the co-infection of 16/18. Tobacco
and betel nut chewing habits were the major etiological
factors involved in our study population.
7082
Asian Pacific Journal of Cancer Prevention, Vol 16, 2015
In contrast to oropharyngeal cancer, oral cancer and
other HNSCC occasionally harbor HPV (Dayyani et al.,
2010; Machado et al., 2010). Its presence is strongly
associated with oropharynx, most notably in tonsils and
base of tongue (El-Mofty, 2003; Gillison et al., 2004).
This might be due to the fact that these tumors may
constitute an etiologically different subgroup within head
and neck tumors. HPV might play a role in progression of
premalignant lesions to advanced cancer form (Miller et
al., 2001) but evidences in this direction are not sufficient.
Low prevalence of HPV in oral cavity carcinoma was
reported by Jerry Machado et al., 2010. Luca Scapoli et
al., 2008 also found a very low prevalence of HPV in oral
cavity (2%) and demonstrated no significant correlation
of HPV in OSCC.
Association of HPV with other factors is also
controversial worldwide, for instance Luciano MarquesSilva et al., 2012 reported no association of HPV positivity
with age. To the contrary Abdul Samad Gichki et al., 2012
reported higher HPV incidence between 20-59 years of
age. Jerry Machado et al., 2010 found no significant
association between HPV presence and smoking, alcohol
status, tumor differentiation, stage and survival. Our study
is in concordance with previous reports of no significant
association of HPV positivity with age, marital status,
demographic profile, tumor stage, grade and site of tumor.
HPV in our case series was significantly associated with
male gender (p=0.02) this is might be due to the fact that
HNSCC is more common in males compared to females
because of the presence of traditional risk factors here.
Earlier studies report that majority of HPV related
carcinomas of the oropharynx are nonkeratinizing
squamous cell carcinoma (NKSCC) with a characteristic
basaloid cellular morphology and these tumors were found
to be more responsive to treatment with a favorable patient
outcome and good prognosis. But HPV positive OSCC,
unlike oropharynx, do not exhibit distinct morphology and
have poor prognosis (El-Mofty et al., 2014). Our study is
in agreement with studies where HPV positive cases did
not demonstrate basaloid morphology (p=0.10) and we
also found no significant differences in survival outcome
(p=0.62) between HPV positive and negative cases.
It is assumed that carcinogenic potential of HPV
increases with viral integration to host genome (Spence
et al., 2005). Smoking induces DNA damage which may
favor the integration of HPV to human genome at these
sites (Luo et al., 2005) thus enhancing the oncogenic
potential of virus. In our study majority of HPV positive
cases (91.3%) had one or multiple of the tobacco related
habits like tobacco and pan masala chewing/smoking.
We have observed significant relationship of HPV with
pan masala chewing (0.01), a habit peculiar to the Indian
subcontinent. The possibility of this may be the local
injury caused to buccal mucosa during tobacco/pan masala
chewing creates atmosphere for virus to infect easily.
The limitation of the present study was that we were
unable to evaluate the oncogenic expressions of HPV
E6/E7 in our case series due to scarce sample amount.
Furthermore, due to lack of relevant information regarding
behavioral history of patients, the route of transmission
of virus is not recognized here. The FDA approved
�DOI:http://dx.doi.org/10.7314/APJCP.2015.16.16.7077
Do Human Papilloma Viruses Play Any Role in Oral Squamous Cell Carcinoma in North Indians?
by p16INK4a immunostaining. Asian Pac J Cancer Prev,
hybrid capture method was not implemented in our cases.
13,
6083-6.
However we have utilized both in-house conventional
AK
Chaudhary,
S Pandya, M Singh, et al (2013). Identification
PCR assay and a kit based real time PCR analysis to
of
high-risk
human papillomavirus-16 and -18 infections
confirm HPV presence. Further sub typing for 16 and
by multiplex PCR and their expression in oral submucous
18 also show independent positive results. Hence we
fibrosis and oral squamous cell carcinoma. Head Neck
feel confident about the presence of HPV in our cases.
Oncol, 5, 4.
Despite of some limitations our data is contributing
Alok Mishra, Alok C Bharti, Prishla Varghese, et al (2006).
needful information regarding HPV presence in OSCC of
Differential expression and activation of NF-jB family
North Indian population that will be useful for the future
proteins during oral carcinogenesis: Role oh high risk human
papilloma infection. Int J Cancer, 119, 2840-50.
treatment implications.
Anil
K Chaturvedi, Eric A Engels, William F Anderson, et al
HPV positive cancers usually show over-expression
(2008).
Incidence trends for human papillomavirus -related
of p16, while the loss of the p16 expression by deletion,
and
-unrelated
oral squamous cell carcinomas in the united
hypermethylation or mutation is common in tobacco
states. J Clin Oncol, 26, 612-19.
related cancers. Therefore, p16 up regulation is an
Balaram P, Nalinakumari KR, Abraham E, et al (1995). Human
indication of expression of viral oncogenes and we can
papilloma virus in 91 oral Indian betel quid chewers: High
expect the presence of HPV (Tran et al., 2007; Vidal et al.,
prevalence and multiplicity of infections. Int J Cancer, 61,
2008; Klussmann et al., 2009; Ahmed et al., 2012), but its
450-4.
relevance for the site of HNSCC other than oropharynx
Byakodi R, Byakodi S, Hiremath S, et al (2012). Oral cancer in
India: an epidemiologic and clinical review. J Community
is ambiguous. In our cases presence of HPV was not
Health, 37, 316-9.
significantly associated with p16 expression and all p16
Dayyani
F, Etzel CJ, Liu M, et al (2010). Meta- analysis of the
positive cases had history of tobacco consumption. It
impact
of human papillomavirus (HPV) on cancer risk and
is possible that tobacco related oncogenic pathway cooverall survival in head and neck squamous cell carcinomas
existed with HPV related events in our cases. Hence,
(HNSCC). Head Neck Oncol, 2, 15.
p16 expression was not found to be a reliable marker
D’Costa J, Saranath D, Dedhia P, et al (1998). Detection of HPVfor HPV presence in our population. Our findings are
16 genome in human oral cancers and potentially malignant
in concordance with Pradit Rushatamukayanunt et al.,
lesions from India. Oral Oncol, 34, 413-20.
2014 who also could not relate p16 expression for HPV
D’Souza, A R Kreimer, R Viscidi, et al (2007). Case-control
study of human papillomavirus and oropharyngeal cancer.
infection in OSCC.
New Engl J Med, 356, 1944-56.
In conclusion, our findings illustrate that 9.2% OSCC
El-Mofty
SK, Lu DW (2003). Prevalence of human papillomavirus
cases harbor HPV in North Indian population which
type
16
DNA in squamous cell carcinoma of the palatine
is slightly lower than that observed in previous Indian
tonsil, and not the oral cavity, in young patients: A distinct
studies and we report tobacco as a major risk factor in
clinicopathologic and molecular disease entity. Am J Surg
both HPV negative as well as positive cases. Therefore the
Pathol, 27, 1463-70.
independent role of HPV in the causation of oral cancer
Elaine M Smith, Justine M Ritchie, Kurt F Summersgill, et al
is difficult to evaluate in our case series due to the strong
(2004). Age, sexual behavior and human papillomavirus
confounding influence of tobacco. We also find that p16
infection in oral cavity and oropharyngeal cancers. Int
J.Cancer, 108, 766-72.
expression is not a reliable marker in the oral cavity to
Freddie
Bray, Jian-Song Ren, Eric Masuyer, et al (2013). Global
assess the potential etiologic role of HPV. Further studies
estimates
of cancer prevalence for 27 sites in the adult
on larger and well defined population are needed to
population
in 2008. Int J Cancer, 132, 1133-45.
elucidate the role of HPV induced oral oncogenesis and
Gillison ML (2004). Human papillomavirus-associated head
co-carcinogenesis pathways need to be explored.
and neck cancer is a distinct epidemiologic, clinical, and
molecular entity. Semin Oncol, 31, 744-54.
Acknowledgements
Hafkamp HC, Manni JJ, Haesevoets A, et al (2008). Marked
Differences in Survival Rate between Smokers and
The authors wish to thank all those who have
Nonsmokers with HPV 16-Associated Tonsillar Carcinomas.
Int J Cancer, 122, 2656-64.
cooperated in the study. Present work was funded by the
JC
De
Vicente, LMJ Gutierrez, AH Zapatero, et al (2004).
Institutional Research Grant, Dr. Ram Manohar Lohia
Prognostic
significance of p53 expression in oral squamous
Institute of Medical Sciences, Lucknow and Rajiv Gandhi
cell
carcinoma
without neck node metastases. Head Neck,
National Fellowship, University Grant Commission
26, 22-30.
(UGC), New Delhi, India (Vineeta Singh; F1-17.1/2011Jerry Machado, Patricia P Reis, Tong Zhang, et al (2010).
12/RGNF-SC-UTT-2841).
Low prevalence of Human Papilloma virus in oral cavity
carcinoma. Head Neck Oncol, 2, 6.
Judit A. Nemes, Levente Deli, ZoltánNemes, et al (2006).
References
Expression of p16 (INK4A), p53, and Rb proteins are
Abdul Samad Gichki, Waranun Buajeeb, Sombhun
independent from the presence of human papillomavirus
Doungudomdacha, et al (2012). Detection of human
genes in oral squamous cell carcinoma. Oral Surg Oral Med
papillomavirus in normal oral cavity in a group of pakistani
Oral Pathol Oral Radiol Endod, 102, 344-52.
subjects using real-time PCR. Asian Pac J Cancer Prev, 13,
Klussmann JP, Mooren JJ, Lehnen M, et al (2009). Genetic
2299-2304.
signatures of HPV-related and unrelated oropharyngeal
Ahmed HG, Mustafa S, Warille E (2012). Human papilloma
carcinoma and their prognostic implications. Clin Cancer
virus attributable head and neck cancer in the Sudan assessed
Res, 15, 1779-86.
Asian Pacific Journal of Cancer Prevention, Vol 16, 2015
7083
�Vineeta Singh et al
Lassen P, Eriksen JG, Hamilton-Dutoit S, et al (2009). Effect
of HPV-associated p16INK4A expression on response to
radiotherapy and survival in squamous cell carcinoma of
the head and neck. J Clin Oncol, 27, 1992-98.
Li-Li Gan, Hao Zhang, Ji-HuaGuo, et al (2014). Prevalence
of human papillomavirus infection in oral squamous cell
carcinoma: a case-control study in Wuhan, China. Asian
Pac J Cancer Prev, 15, 5861-65.
Luo LZ, Werner KM, Gollin SM, et al (2004). Cigarette smoke
induces anaphase bridges and genomic imbalances in normal
cells. Mutat Res, 554, 375-85.
Luca Scapoli, Annalisa Palmieri, Corrado Rubini, et al (2009).
Low prevalence of human papillomavirus in squamous- cell
carcinoma limited to oral cavity proper. Modern Pathol,
22, 366-72.
Luciano Marques-Silva, Lucyana Conceição Farias, Carlos
Alberto De Carvalho Fraga, et al (2012). HPV-16/18
detection does not affect the prognosis of head and neck
squamous cell carcinoma in younger and older patients.
Oncol Letters, 3, 945-49.
Maura L Gillison, Wayne M Koch, Randolph B. Capone, et al
(2000). Evidence for a causal association between human
papillomavirus and a subset of head and neck cancers. J
National Cancer Inst, 92, 9.
Marur S, D’Souza G, Westra WH, et al (2010). HPV-associated
head and neck cancer: a virus-related cancer epidemic.
Lancet Oncol, 11, 781-9.
MahmudaAkhter, Liaquat Ali, Zahid Hassan, et al (2013).
Association of human papilloma virus infection and oral
squamous cell carcinoma in bangladesh. J Health Popul
Nutr, 31, 65-9
Mark W. Lingen, Weihong Xiao, Alessandra Schmitt (2013).
Low etiologic fraction for high-risk human papillomavirus
in oral cavity squamous cell carcinomas.Oral Oncol, 49, 1-8.
Miller CS, Johnstone BM (2001). Human papillomavirus as a
risk factor for oral squamous cell carcinoma: a meta-analysis,
1982-1997. Oral Surg Oral Med Oral Pathol Oral Radiol
Endod, 91, 622-35
Mia Hashibe, Paul Brennan, Shu-chun Chuang, et al (2009).
Interaction between tobacco and alcohol use and the risk
of head and neck cancer: pooled analysis in the inhance
consortium. Cancer Epidemiol Biomarkers Prev, 18, 541-50.
M Rani, S Bonu, P Jha, et al (2003). Tobacco use in India:
prevalence and predictors of smoking and chewing in a
national cross sectional household survey. Tob Control, 12, 4.
P.E.Gravitt,C.L.Peyton, T.Q.Alessi, et al (2000). Improved
amplification of genital human papillomaviruses. J Clin
Microbiol, 38, 357-61.
Priya Koppikar, Ethel-Michele deVilliers, Rita Mulherkar
(2005). Identification of human papillomaviruses in tumors
of the oral cavity in an Indian community. Int J Cancer,
113, 946-50.
Pradit Rushatamukayanunt, Kei-ichi Morita, Sho Matsukawa,
et al (2014). Lack of association between high-risk human
papillomaviruses and oral squamous cell carcinoma in Young
Japanese Patients. Asian Pac J Cancer Prev, 15, 4135-41.
Samir K El-Mofty (2014). Histopathologic risk factors in oral
and oropharyngeal squamous cell carcinoma variants: An
update with special reference to HPV-related carcinomas.
Med Oral Patol Oral Cir Bucal, 19, 377-85.
Sharma H, Singh A, Sharma C, et al (2005). Mutations in the
mitochondrial DNA D-loop region are frequent in cervical
cancer. Cancer Cell Int, 5, 34.
Spence AR, Franco EL, Ferenczy A (2005). The role of human
papillomavirus in cancer. Am J Cancer, 4, 49-64.
Suyamindra S Kulkarni, Sujayendra S Kulkarni, Priyanka P
Vastrad, et al (2011). Prevalence and distribution of high
7084
Asian Pacific Journal of Cancer Prevention, Vol 16, 2015
risk human papillomavirus (HPV) types 16 and 18 in
carcinoma of cervix, saliva of patients with oral squamous
cell carcinoma and in the general population in Karnataka,
India. Asian Pac J Cancer Prev, 12, 645-48.
Termine N, Panzarella V, Falaschini S, et al (2008). HPV in
oral squamous cell carcinoma vs head and neck squamous
cell carcinoma biopsies: a meta-analysis (1988-2007). Ann
Oncol, 19, 1681-90.
Tran N, Rose BR, O’Brien CJ (2007). Role of human
papillomavirus in the etiology of head and neck cancer.
Head Neck, 29, 64-70.
Vidal L, Gillison ML (2008). Human papillomavirus in HNSCC:
recognition of a distinct disease type. Hematol Oncol Clin
North Am, 22, 1125-42.
�
 Shikha Tewari
Shikha Tewari