Tropical Medicine and International Health
doi:10.1111/j.1365-3156.2008.02038.x
volume 13 no 2 pp 286–290 february 2008
Desiccated vector mosquitoes used for the surveillance of
Japanese encephalitis virus activity in endemic southern India
S. C. Tewari, V. Thenmozhi, N. Arunachalam, P. Philip Samuel and B. K. Tyagi
Centre for Research in Medical Entomology, Madurai, India
Summary
To monitor Japanese encephalitis virus (JEV) activity in endemic areas of Tamil Nadu, southern India,
desiccated vector mosquitoes were screened for JEV antigen using ELISA, from 1996. A total of 133 233
specimens from eight index villages comprising 2816 pools (mainly Culex vishnui subgroup) were tested.
Of these, 59 pools (2.1%) were positive for JEV antigen. Control measures were undertaken in positive
villages accordingly. The average annual minimum infection rate was 0.8 at the beginning of the study
and remained lower for nearly 8 years. A declining trend in JE cases was recorded.
keywords desiccated mosquitoes, Culex vishnui subgroup, surveillance, Japanese encephalitis virus
Introduction
Japanese encephalitis (JE) is a mosquito-transmitted
arboviral disease mainly affecting children <15 years of
age. It is a major public health problem worldwide because
of its high mortality and morbidity coupled with neurological sequelae during epidemics (Solomon 1997; Gajanana 1998). The epidemiology of JE is complex due to
involvement of several vertebrate and invertebrate hosts.
JE virus (JEV) is transmitted naturally between ardeid birds
and pigs by mosquito species belonging to the Culex
vishnui subgroup, comprising Culex tritaeniorhynchus,
Culex vishnui and Culex pseudovishnui, in India (Reuben
et al. 1994). Domestic pigs are considered as amplifying,
humans as accidental and cattle as dead end hosts (Reuben
et al. 1992; Solomon et al. 2000).
A sound surveillance system is an integral part of
arboviral disease control programmes. At present, surveillance of JE in endemic areas is mainly based on clinical case
reporting and monitoring abundance of vector mosquitoes.
JEV activity has been monitored using pigs (Thenmozhi
et al.1991), donkeys (Mani et al. 1991) and goats (Rajendran et al. 2003) as sentinel animals. As the pig is an
amplifying host for JEV, the introduction of non-immune
animals to endemic areas as sentinels is unethical. Further,
the pig may serve as a sensitive indicator of JEV activity in
a given area, but may not be a good predictor of the risk to
humans (Peiris et al. 1993). Donkeys are rarely available in
the villages and may die of JEV infection.
Vector infection and abundance were found to be good
indicators of JE occurrence in surveillance studies con286
ducted in South India (Gajanana et al. 1997). The antigencapture enzyme-linked immunosorbent assay (ELISA) is a
rapid and sensitive method for the detection of JEV
infection in wild-caught vector mosquitoes. The assay was
validated in large-scale field trials in southern India
(Gajanana et al. 1997). Hence, it was considered useful for
surveillance of JEV activity in endemic areas, but transportation of field-collected live specimens under cold-chain
conditions to the central laboratory was a major limitation.
Peiris et al. (1993) found JEV antigen in dead mosquitoes
by ELISA. Tewari et al. (1999) applied this observation to
develop an improved surveillance system in nine districts of
Tamil Nadu from March 1996 to February 1999 (Tewari
et al. 1999). The study was extended for 5 years and the
consolidated results of the study from March 1996 until
December 2004 are presented in this paper.
Materials and methods
The details of the study area and the methods employed are
described elsewhere (Tewari et al. 1999). Briefly, the
(CRME) formed a JE surveillance network with the Zonal
Entomological Team (ZET) of the Department of Public
Health & Preventive Medicine, Goverment of Tamil Nadu,
of nine districts for JE. Of these, eight districts namely
Tiruchirapalli, Virudhunagar, Dindigul, Thirunelvelli,
Cuddalore, Vellore, Coimbatore and Salem are endemic,
whereas one district namely Thanjavur is non-endemic.
The endemic districts had reported JE human cases at least
once in 3 years; the non-endemic district had reported none
in the past 10 years. One village with at least one case or
ª 2008 Blackwell Publishing Ltd
�Tropical Medicine and International Health
volume 13 no 2 pp 286–290 february 2008
S. C. Tewari et al. JEV surveillance in southern India
death due to JE in the past 3 years in each district was
selected as the index village. Every 3 years, the allocation
of index villages was reviewed and if no case ⁄ death was
reported consecutively for 3 years, the index villages used
to be shifted to another nearby one where cases occurred
recently. Specimens were received throughout the year as
ZET visits each index village monthly for the longitudinal
study to collect specimens.
Field staff of the ZETs collected the mosquitoes at dusk
and after identification, desiccation and pooling by species
(7–50 ⁄ pool), put them in polythene packets and posted
them to the laboratory in CRME, Madurai. In CRME, the
vectors were re-identified. Mutilated specimens which
could not be identified to species level were pooled and
classified as Cx. vishnui subgroup. Subsequently each
mosquito pool was screened by antigen-capture ELISA
(Gajanana et al. 1995), and JEV identified by inhibition
ELISA (Tsai et al.1987). Results of positive pools were
communicated to the health authorities within a fortnight
of receipt of the mosquito vector samples. The infection in
vector was recorded as the minimum infection rate (MIR;
MIR = [No. of positive pools ⁄ Total no. of specimens
tested] · 1000). Statistical analysis was carried out using
SPSS 11.5.
Results
From March 1996 to December 2004, a total of 2816
pools (133 233 mosquito specimens) were received from
nine ZETs. A total of 429 pools (21 005 specimen) were
Cx. tritaeniorhynchus, 61 pools (2787 specimen) were
Cx. vishnui, three pools (120 specimen) were Cx. pseudovishnui, 2142 pools (101 707 mutilated specimens) were
Cx. vishnui subgroup, 177 pools (7485 specimen) were
Culex gelidus, three pools (104 specimen) were Culex
fuscocephala and one pool (25 specimen) was Culex
bitaeniorhynchus. Fifty-nine pools (Cx. tritaeniorhynchus
13, Cx. vishnui 1, Cx. vishnui subgroup 41 and Cx. gelidus
4) tested positive for JEV antigen by ELISA (Table 1).
Among the 41 positive pools of Cx. vishnui subgroup, the
probability would be maximum number of Cx. tritaeniorhynchus pools, although the number of pools was
lower in the beginning of the study as implementation of
the programme took time to gear up the peripheral
health workers. Most of the positive pools were recorded
during JE transmission season, and at least one positive
pool was recorded each year (except 1998) with the highest
number of positive pools (27) in 2004. The annual MIR
was 0.8 at the beginning of the study (1996) and remained
lower than this value for nearly 8 years (up to 2004).
There was no correlation between MIR and JE cases during
the study period (Table 1). In 2003 (v2 11.42, P < 0.001),
ª 2008 Blackwell Publishing Ltd
Table 1 Japanese encephalitis virus antigen detected in desiccated
vector mosquitoes and human JE cases recorded in Tamil Nadu
state, 1996–2004
Year
1996
1997
1998
1999
2000
2001
2002
2003
2004
Total
No. pools tested
(mosquitoes
specimens)
25
145
79
202
399
410
316
464
776
(1250)
(6880)
(3784)
(9656)
(18391)
(18515)
(14363)
(21711)
(38683)
2816 (1,33,233)
No. positive
pools ⁄ minimum
infection rate (MIR)
No. of
cases
(death)*
1 ⁄ 0.8
2 ⁄ 0.29
0⁄0
5 ⁄ 0.52
2 ⁄ 0.11
11 ⁄ 0.59
2 ⁄ 0.14
9 ⁄ 0.41
27 ⁄ 0.70
111
89
25
14
4
0
0
163
19
59 ⁄ 0.44
425 (132)
(53)
(42)
(14)
(5)
(0)
(9)
(9)
*Courtesy of Annual Report Min. Hlth. Govt. of India.
there was a sudden rise in MIR (1.3) in the non-endemic
zone Thanjavur, indicating an increase in the circulation of
JEV (Table 2). However, no human case was reported in
this area during the study period, and there was no
significant difference (v2 = 0.05 P = 0.94 using Fisher’s
exact test) in overall infection rate (MIR) between nonendemic and endemic areas between 2000 and 2004.
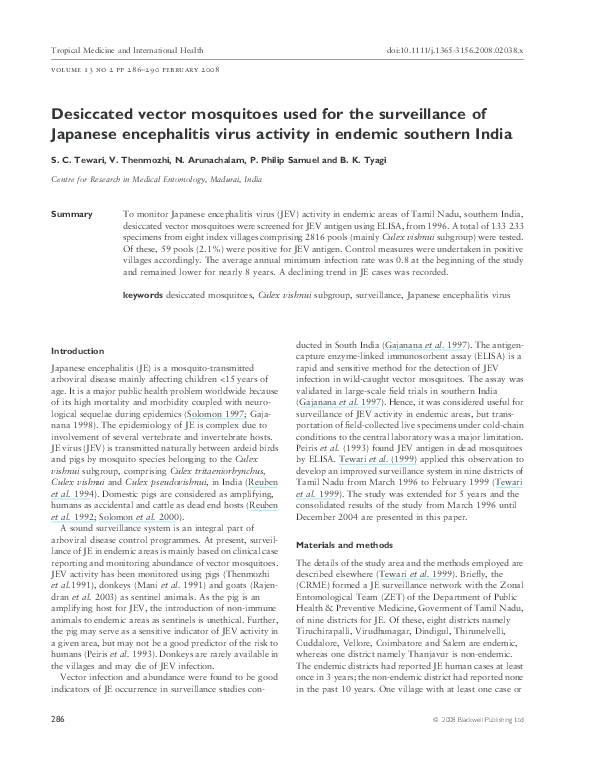
Among the endemic zones, two zones, Tiruchirapalli and
Cuddalore, were relatively more viraemic than the other
endemic zones, as 90.24% (37 ⁄ 41) of positives were
recorded from these two areas (Figure 1).
Discussion
This study indicated that the existing infrastructure with
the health department could be effectively used for
surveillance of JEV activity in endemic areas. ELISA is
particularly useful for mass screening of mosquitoes
quickly and communicating results to field staff. JEV
antigen was detected in 59 pools of vector mosquitoes.
Of these, 55 belonged to Cx. vishnui subgroup in which
Cx. tritaeniorhynchus is a dominant species. Field-collected
adults of Cx. vishnui subgroup are difficult to identify;
nearly 88% could be identified up to species status (Reuben
1969). In this study, we received for analysis, species which
had been transported via surface mail, which increases
the mutilation of specimens. Hence, prior to ELISA test
while re-identification most of the specimens were pooled
as Cx. vishnui subgroup (mixed specimens of Cx. tritaeniorhynchus, Cx. vishnui and Cx. pseudovishnui). In
these mixed pools of Vishnui subgroup, Cx. tritaeniorhynchus would be dominant, as studies in southern
India already demonstrated that Cx. tritaeniorhynchus is
a dominant species in rural environment of paddy
287
�Tropical Medicine and International Health
volume 13 no 2 pp 286–290 february 2008
S. C. Tewari et al. JEV surveillance in southern India
Table 2 Comparison of JEV activity in non-endemic and endemic study areas (2000–2004)
Places ⁄ year
Non-endemic zone (1)
Mosquitoes specimens ⁄ no.
pools tested
Positive pools
MIR
Endemic zones (8)
Mosquitoes specimens ⁄ no.
pools tested
Positive pools
MIR
2000
2001
2002
2003
2004
Total
3813 ⁄ 83
4125 ⁄ 90
4879 ⁄ 100
5400 ⁄ 113
6005 ⁄ 123
24222 ⁄ 509
0
0
0
0
0
0
7
1.3
3
0.5
10
0.41
14578 ⁄ 316
14545 ⁄ 319
6484 ⁄ 216
16251 ⁄ 351
32678 ⁄ 653
84536 ⁄ 1855
2
0.14
11
0.76
2
0.31
2
0.12
24
0.73
41
0.49
MIR, minimum infection rate; JEV, Japanese encephalitis virus.
ecosystem where it was found ranging between 55 and
78% (Reuben 1971; Mani et al. 1991; Gajanana et al.
1997; Sunish & Reuben 2001). The JEV-antigen detection
in desiccated vector pools in this study confirms that
Cx. tritaeniorhynchus is the main vector of JEV in the
study areas (Gajanana et al. 1997). However, in south
India, all the three species had been identified as vectors of
JE (Reuben et al. 1988, 1994).
There was no significant difference (v2 = 0.05 p 0.94,
Fisher’s exact test) in overall infection rate (MIR) between
non-endemic and endemic areas, indicating occurrence of
silent JEV transmission in the non-endemic Thanjavur
zone. This phenomenon was also recorded earlier in a
serological investigation of children, 1991–1993 (Vijayarani & Gajanana 2000). Hence, it confirms that the rural
population of the non-endemic zone is getting sublethal
doses of JEV.
There has been a decline in deaths ⁄ cases due to JE in
Tamil Nadu since 1999 onwards. However, JEV activity
continued, although no case was reported in 2001 and
2002. This may be because of underreporting as laboratory
diagnostic facilities are inadequate in the existing health
system. In hospital-based studies in south India, 50% of
suspected encephalitis cases were confirmed as JE
(Gajanana et al. 1996; Kabilan et al. 2004). Another
possibility is that the natural immunity level of the endemic
population has increased due exposure to infective bites of
JE vectors, which was estimated to be 0.53 from Cuddalore
district (Gajanana et al. 1997). The JEV antigen was
mainly detected from the collections made between August
and January, which is the JE transmission season in
southern India (Gajanana et al. 1997). Cuddalore and
Tiruchirapalli, situated close to each other (Figure 1), were
found to be the epicentre of JE in Tamil Nadu.
There was a significant rise in MIR (1.3) in the hitherto
non-endemic area, viz. Thanjavur district, which remains
free of human JE cases (Vijayarani & Gajanana 2000). The
288
reasons would be (i) the characteristic of zoonotic diseases
which do not spill over to humans, although JEV circulation in nature continued in vector and hosts; ii) a classical
longitudinal study from 1991 to 1993 in Thanjavur area
showed that the ratio of pig (amplifying host) to cattle
(dumping host) was 1:400, whereas in the neighbouring JE
endemic area it was 1:4 (Vijayarani & Gajanana 2000).
Species of Cx. vishnui subgroup are zoophilic and JEV does
not multiply in cattle. Hence JEV did not spill over to
humans (Ilkal et al. 1988).
The ELISA technology has many advantages over the
conventional sentinel animal method to monitor JEV
activity. It does not require a cold-chain for the preservation and transportation of vector mosquitoes from
peripheral rural health centres to the central laboratory.
Screening vector mosquito pools for JEV infection by using
JE-antigen capture ELISA was the most rapid system
compared to other highly sensitive systems such as insect
bioassay (Toxo-IFA system) or IIF, which are cumbersome,
time-consuming (Gajanana et al. 1995) and thus unsuitable for routine surveillance programmes where results
must be disseminated to operational organizations within a
week. This improved surveillance networking system was
effective in identifying high-risk areas to initiate appropriate control measures and could be implemented elsewhere in JE prone areas in the country to avoid impending
outbreaks.
Acknowledgements
We thank the Director General of the Indian Council of
Medical Research for providing the required facilities and
for his consistent encouragement. We also gratefully
acknowledge the cooperation by the Director, Department
of Public Health & Preventive Medicine (DPH&PM),
Tamil Nadu. We are deeply grateful to Dr. N.C
Appavoo (former Director DPH&PM, Tamil Nadu) and
ª 2008 Blackwell Publishing Ltd
�Tropical Medicine and International Health
volume 13 no 2 pp 286–290 february 2008
S. C. Tewari et al. JEV surveillance in southern India
N
INDIA
H
ADES
A PR
R
ANDH
Vellore
A
KARNATAK
24
Salem
2
Cuddalore
im
Co
re
to
ba
li
13 pal
a
r
11
i
h
uc
Thanjavur
r
i
T
ALA
KER
1
Dindigul
2
Virudhunagar
Number of positive pools
6
Tirunelveli
Figure 1 Japanese encephalitis virus activity in the different entomological zones of Tamil Nadu, India.
Dr. A. Gajanana (Former Officer in-Charge, CRME) who
initially formulated and implemented this surveillance
network programme, and also critically reviewed the
ª 2008 Blackwell Publishing Ltd
manuscript. We thank the Centre for Disease Control, Fort
Collins, USA for providing JEV monoclonal antibodies. We
appreciate the excellent technical assistance rendered by
289
�Tropical Medicine and International Health
volume 13 no 2 pp 286–290 february 2008
S. C. Tewari et al. JEV surveillance in southern India
staff members of CRME, Madurai Culex ecology and
Serology sections and Mr. A. Venkatesh for desktop
publishing and illustration.
References
Gajanana A (1998) Epidemiology and surveillance of Japanese
encephalitis in Tamil Nadu. ICMR Bulletin 28, 33–37.
Gajanana A, Rajendran R, Thenmozhi V, Samuel PP, Tsai TF &
Reuben R (1995) Comparative evaluation of bioassay and
ELISA for detection of Japanese encephalitis virus in field collected mosquitoes. Southeast Asian Journal of Tropical Medicine and Public Health 26, 91–97.
Gajanana A, Philip Samuel P, Thenmozhi V & Rajendran R
(1996) An appraisal of some recent diagnostic assays for Japanese encephalitis. Southeast Asian Journal of Tropical Medicine
and Public Health 27, 673–679.
Gajanana A, Rajendran R, Philip Samuel P et al. (1997) Japanese
encephalitis in South Arcot district, Tamil Nadu: A three-year
longitudinal study of vector abundance and infection frequency.
Journal of Medical Entomology 34, 651–659.
Ilkal MA, Dhanda V, Rao BU et al. (1988) Absence of viraemia in
cattle after experimental infection with Japanese encephalitis
virus. Transactions of the Royal Society of Tropical Medicine
and Hygiene 82, 628–631.
Kabilan L, Vrati S, Ramesh S et al. (2004) Japanese encephalitis
virus (JEV) is an important cause of encephalitis among children
in Cuddalore district, Tamil Nadu, India. Journal of Clinical
Virology 31, 153–159.
Mani TR, Mohan Rao CVR, Rajendran R et al. (1991) Surveillance for Japanese encephalitis in villages near Madurai, Tamil
Nadu, India. Transactions of the Royal Society of Tropical
Medicine and Hygiene 85, 287–291.
Peiris JSM, Amerasinghe FP, Arunagiri CK et al. (1993)
Japanese encephalitis in Sri Lanka: comparison of vector
and virus ecology in different agro-climatic areas. Transactions of the Royal Society of Tropical Medicine and Hygiene
87, 541–548.
Rajendran R, Thenmozhi V, Tewari SC et al. (2003) Longitudinal
studies in south Indian villages on Japanese encephalitis virus
infection in mosquitoes and seroconversion in goats. Tropical
Medicine and International Health 8, 174–181.
Reuben R (1969) A redescription of Culex vishnui Colles and
Culex tritaeniorhynchus Giles, from southern India. Bulletin of
Entomological Research 58, 643–652.
Reuben R (1971) Studies on the mosquitoes of North Arcot District, Madras state, India. Part 5. Breeding places of the Culex
vishnui group of species. Journal of Medical Entomology 8,
363–366.
Reuben R, Kaul H & Soman RS (1988) Mosquitoes of arboviral
importance in India. Mosquito Borne Diseases Bulletin 5, 48–54.
Reuben R, Thenmozhi V, Samuel PP, Gajanana A & Mani TR
(1992) Mosquito blood feeding patterns as a factor in the epidemiology of Japanese encephalitis in southern India. American
Journal of Tropical Medicine & Hygiene 46, 654–663.
Reuben R, Tewari SC, Hiriyan J & Akiyama J (1994) Illustrated
keys to species of Culex (Culex) associated with Japanese
encephalitis in Southeast Asia (Diptera: Culicidae). Mosquito
Systematics 26, 75–96.
Solomon T (1997) Viral encephalitis in southeast Asia. Neurological Infections and Epidemiology 2, 191–199.
Solomon T, Dung NM, Keen R, Gainsborough M, Wvaughn D &
Khanh VT (2000) Japanese encephalitis. Journal of Neurosurgery and Psychiatry 68, 405–415.
Sunish IP & Reuben R (2001) Factors influencing the abundance
of Japanese encephalitis vector in rice fields in India- 1 Abiotic.
Medical Veterinary Entomology 15, 381–392.
Tewari SC, Thenmozhi V, Rajendran R, Appavoo NC & Gajanana A (1999) Detection of Japanese encephalitis virus antigen
in desiccated mosquitoes: an improved surveillance system.
Transactions of the Royal Society of Tropical Medicine and
Hygiene 93, 525–526.
Thenmozhi V, Samuel PP, Gajanana A & Reuben R (1991)
Temporal relationship of swine infection of Japanese encephalitis virus to human cases in a Japanese encephalitis endemic
area of Tamil Nadu. Virus Information Exchange Newsletter 8,
64.
Tsai TF, Bolin RA, Montoya M et al. (1987) Detection of St Louis
encephalitis virus antigen in mosquitoes by capture enzyme
immunoassay. Journal of Clinical Microbiology 25, 370–376.
Vijayarani H & Gajanana A (2000) Low rate of Japanese
encephalitis infection in rural children in Thanjavur district
(Tamil Nadu), an area with extensive paddy cultivation. Indian
Journal of Medical Research 111, 212–214.
Corresponding Author S.C. Tewari, Centre for Research in Medical Entomology (Indian Council of Medical Research), 4 Sarojini
Street, Chinna Chokkikulam, Madurai 625 002, Tamil Nadu, India. Tel.: 91 452 2531430; Fax: 91 452 2530660;
E-mail: crmeicmr@icmr.org.in
290
ª 2008 Blackwell Publishing Ltd
�
 Samuel Kishore
Samuel Kishore