Final patho-HCVD
Final patho-HCVD
Download as docx, pdf, or txt
You might also like
- Defibrillation ChecklistDocument4 pagesDefibrillation ChecklistCzarina100% (2)
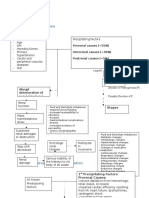
- Pathophysiology of Congestive Heart Failure: Predisposing Factors Precipitating/Aggravating FactorsDocument1 pagePathophysiology of Congestive Heart Failure: Predisposing Factors Precipitating/Aggravating Factorsguillermojerry100% (2)
- Bowel Obstruction PathophysiologyDocument4 pagesBowel Obstruction PathophysiologyAya BolinasNo ratings yet
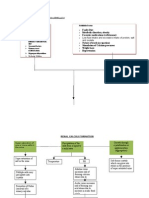
- Pathophysiology of Nephrolithiasis, Struvites Stone (Staghorn Calculi)Document2 pagesPathophysiology of Nephrolithiasis, Struvites Stone (Staghorn Calculi)Floyd100% (2)
- Pathophysiology of HCVD DM2 CVD Left Basal GangliaDocument1 pagePathophysiology of HCVD DM2 CVD Left Basal GangliaJake Caballo100% (1)
- Pathophysiology of DMDocument4 pagesPathophysiology of DMNicole Louise N. VillanuevaNo ratings yet
- Hypertension PathophysiologyDocument1 pageHypertension PathophysiologyZaida Eunice EstabayaNo ratings yet
- Pathophysiology Acute Pyelonephritis: Precipitating FactorsDocument2 pagesPathophysiology Acute Pyelonephritis: Precipitating Factorsgodwinkent888No ratings yet
- Final Lung Cancer Concept MapDocument3 pagesFinal Lung Cancer Concept MapKaycee TolingNo ratings yet
- Qtsoi Concept MapDocument5 pagesQtsoi Concept MapGenella BabantoNo ratings yet
- Patho UGIBDocument3 pagesPatho UGIBKristineBungcagNo ratings yet
- Etiology: Predisposing Factors: Precipitating FactorsDocument5 pagesEtiology: Predisposing Factors: Precipitating FactorsJanelle NarcisoNo ratings yet
- Angina Pectoris PathophysiologyDocument2 pagesAngina Pectoris Pathophysiologydana88% (8)
- HypertensionDocument13 pagesHypertensionkennedy1434450% (4)
- Cpms College of Nursing: Assignment ON Electrocardiogram (ECG)Document6 pagesCpms College of Nursing: Assignment ON Electrocardiogram (ECG)Amy Lalringhluani Chhakchhuak100% (3)
- Comparison of Myocardial Ischemia During Intense Mental Stress Using Flight SimulationDocument7 pagesComparison of Myocardial Ischemia During Intense Mental Stress Using Flight Simulationluis11256No ratings yet
- Pathophysiology CHF MineDocument2 pagesPathophysiology CHF MineCalimlim KimNo ratings yet
- Renal Diseases PathophysiologyDocument6 pagesRenal Diseases PathophysiologyBilly Gayados100% (1)
- Pathophysiology of HCVD, DM2, CVD (Left Basal Ganglia)Document1 pagePathophysiology of HCVD, DM2, CVD (Left Basal Ganglia)rexale ria100% (1)
- Pathophysiology Sickle Cell AnemiaDocument1 pagePathophysiology Sickle Cell AnemiaTine GuibaoNo ratings yet
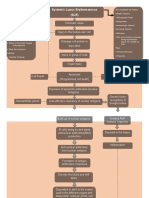
- Systemic Lupus Erythematosus (SLE) : Genetic Factors Environmental FactorsDocument5 pagesSystemic Lupus Erythematosus (SLE) : Genetic Factors Environmental Factorsjoyrena ochondraNo ratings yet
- Cva Concept MapDocument1 pageCva Concept MapAnn Justine OrbetaNo ratings yet
- Pathophysiology of Inflammatory ResponseDocument1 pagePathophysiology of Inflammatory ResponseDeo FactuarNo ratings yet
- Pathophysiology Diagram of Congestive Heart FailureDocument3 pagesPathophysiology Diagram of Congestive Heart Failurea_samiane64% (11)
- Stroke PathoDocument15 pagesStroke PathoWiljohn de la CruzNo ratings yet
- Pathophysio Chronic GlomerulonephritisDocument1 pagePathophysio Chronic GlomerulonephritisRan Ma100% (1)
- CeVD, MI, HCVD & Atrial Fibrillation PathophysiologyDocument3 pagesCeVD, MI, HCVD & Atrial Fibrillation PathophysiologyJjessmar Bolivar FamaNo ratings yet
- APPENDICITISDocument2 pagesAPPENDICITISRay Dan Aro CelerianNo ratings yet
- PathoPhysiology of Renal Failure OverviewDocument7 pagesPathoPhysiology of Renal Failure Overviewnursing concept maps100% (1)
- Pathophysiology-Kni Ns PLZZZDocument8 pagesPathophysiology-Kni Ns PLZZZAnna Lira Manluyang MungcalNo ratings yet
- DiverticulitisDocument2 pagesDiverticulitisyapyapvinx50% (2)
- V. Pathophysiology Modifiable: Non - ModifiableDocument2 pagesV. Pathophysiology Modifiable: Non - ModifiableMary Grace BanezNo ratings yet
- IV. The PATIENTS ILLNESS (Nephrolithiasis) Pathophysiology (Book-Based)Document3 pagesIV. The PATIENTS ILLNESS (Nephrolithiasis) Pathophysiology (Book-Based)wapakalypseNo ratings yet
- PathoDocument7 pagesPathoAnonymous 87fNoO2fhVNo ratings yet
- Pathophysiology of Gastrointestinal Bleeding Secondary To Bleeding PolypsDocument1 pagePathophysiology of Gastrointestinal Bleeding Secondary To Bleeding PolypsGinoTevesNo ratings yet
- HCVD Cad Cva InfarctionDocument2 pagesHCVD Cad Cva InfarctionMiguel Carlos Tacderan100% (1)
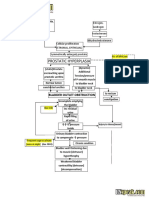
- Benign Prostatic Hyperplasia BPH Pathophysiology Schematic Diagram PDFDocument2 pagesBenign Prostatic Hyperplasia BPH Pathophysiology Schematic Diagram PDFgailNo ratings yet
- Pathophysiology of CHFDocument1 pagePathophysiology of CHFLance MarquezNo ratings yet
- Patof DMDocument1 pagePatof DMxerwaneNo ratings yet
- Urinary Tract Infection pATho SHEENADocument2 pagesUrinary Tract Infection pATho SHEENASheena Arnoco ToraynoNo ratings yet
- Pathophysiology of Severe AnemiaDocument3 pagesPathophysiology of Severe AnemiaChrizley Shawn DeroniaNo ratings yet
- Pathophysiology of AppendicitisDocument2 pagesPathophysiology of AppendicitisSherry Mae Rizza GonzalesNo ratings yet
- COPD PathophysioDocument1 pageCOPD Pathophysionanette flores dela cruzNo ratings yet
- Pathophysiology of Hypertension, Diabetes, Ubm, BPHDocument3 pagesPathophysiology of Hypertension, Diabetes, Ubm, BPHCarly Beth Caparida LangerasNo ratings yet
- Coronary Artery Disease PathophysiologyDocument3 pagesCoronary Artery Disease PathophysiologyElmer Balgos Alinsog60% (5)
- Pathophysiolgoy Coronary Artery DiseaseDocument3 pagesPathophysiolgoy Coronary Artery DiseaseNursesLabs.comNo ratings yet
- Pathophysiology of AMLDocument1 pagePathophysiology of AMLjake251996100% (1)
- Pathophysiology of Cervical Cancer: High Risk HPV (16, 18, 31)Document2 pagesPathophysiology of Cervical Cancer: High Risk HPV (16, 18, 31)Moses Gabriel ValledorNo ratings yet
- Age Greater Than 60 Y/o Hereditary Precipitating Factors: Hypertension Increase Protein and Fat IntakeDocument3 pagesAge Greater Than 60 Y/o Hereditary Precipitating Factors: Hypertension Increase Protein and Fat Intakenursing concept mapsNo ratings yet
- Pathophysiology Sickle Cell Anemia PDFDocument1 pagePathophysiology Sickle Cell Anemia PDFTine GuibaoNo ratings yet
- Dengue Hemorrhagic Fever Pathophysiology DiagramDocument4 pagesDengue Hemorrhagic Fever Pathophysiology DiagramAni MarlinaNo ratings yet
- Pathophysiology PDFDocument3 pagesPathophysiology PDFJenievieve MerzaNo ratings yet
- Pathophysiology Diagram of Congestive Heart FailureDocument3 pagesPathophysiology Diagram of Congestive Heart FailureLeng Royo BrionesNo ratings yet
- Pathophysiology of Benign Prostatic HyperplasiaDocument1 pagePathophysiology of Benign Prostatic HyperplasiaKevin Jade Herrera0% (2)
- Pathophysiology of Congestive Heart FailureDocument2 pagesPathophysiology of Congestive Heart FailureAnonymous XvwKtnSrMR100% (10)
- Pathophysiology (Client Base) :: Predisposing Factors: Precipitating FactorsDocument1 pagePathophysiology (Client Base) :: Predisposing Factors: Precipitating Factorsleslie_macasaetNo ratings yet
- Patho Pleural EffusionDocument2 pagesPatho Pleural EffusionJess Prodigo50% (2)
- Pathophysiology Hemor CVADocument4 pagesPathophysiology Hemor CVAMatthew Emmanuel M. Martinez100% (2)
- ShocksDocument1 pageShocksmadelinexundae.cabucoNo ratings yet
- Pathophysiology of Congestive Heart FailureDocument3 pagesPathophysiology of Congestive Heart FailureMel Izhra N. MargateNo ratings yet
- Biology 1 EditedDocument336 pagesBiology 1 EditedEmperor GooseNo ratings yet
- Pre Gestational 1Document12 pagesPre Gestational 1Fatima TañedoNo ratings yet
- Pathophysiology of Congestive Heart FailureDocument3 pagesPathophysiology of Congestive Heart Failuretinayko100% (1)
- PathophysiologyDocument34 pagesPathophysiologyeunams_1195% (20)
- Prometric Sample For DentistryDocument43 pagesPrometric Sample For DentistryAlvin RamirezNo ratings yet
- Copd PathoDocument2 pagesCopd PathoAlvin RamirezNo ratings yet
- Nbs 3Document17 pagesNbs 3Alvin RamirezNo ratings yet
- Generic Name: Brand Name: Zurenix Classification: Doctor's Order: 750 Date Started: Nursing ConsiderationsDocument3 pagesGeneric Name: Brand Name: Zurenix Classification: Doctor's Order: 750 Date Started: Nursing ConsiderationsAlvin RamirezNo ratings yet
- HypertensionDocument1 pageHypertensionAlvin RamirezNo ratings yet
- Toto Na DawDocument30 pagesToto Na DawAlvin RamirezNo ratings yet
- Cardiac AssessmentDocument48 pagesCardiac AssessmentRatheesh NathNo ratings yet
- TOAST MASTER Hypertention NewDocument15 pagesTOAST MASTER Hypertention Newdiahpurnama dewiNo ratings yet
- Anti Anginal DrugsDocument26 pagesAnti Anginal DrugsAtharva PuranikNo ratings yet
- DPP - Body Fluids & Its Circulation PDFDocument6 pagesDPP - Body Fluids & Its Circulation PDFKisna guptaNo ratings yet
- Physiology of The HeartDocument27 pagesPhysiology of The HeartNavadeep KalluriNo ratings yet
- Ikram 2021 IOP Conf. Ser. Mater. Sci. Eng. 1084 012129Document7 pagesIkram 2021 IOP Conf. Ser. Mater. Sci. Eng. 1084 012129Anagha PradeepNo ratings yet
- Cardiovascular DisordersDocument10 pagesCardiovascular DisordersAngel Joy CatalanNo ratings yet
- Neurovascular DisordersDocument42 pagesNeurovascular DisordersAlexandra Nedelcoff-GhiranlieffNo ratings yet
- Blood VesselsDocument4 pagesBlood VesselsNeel GamiNo ratings yet
- Complication of Hemodialysis and Their ManagementDocument52 pagesComplication of Hemodialysis and Their ManagementRetno SumaraNo ratings yet
- #7assess CV Function Physical ExamDocument27 pages#7assess CV Function Physical Exam2A - Nicole Marrie HonradoNo ratings yet
- Lifedop Abi Calculation ChartDocument1 pageLifedop Abi Calculation ChartRetno SumaraNo ratings yet
- BJAS-Volume 3-Issue 1 - Page 11-16Document6 pagesBJAS-Volume 3-Issue 1 - Page 11-16rakaNo ratings yet
- Rundown WORKSHOP BKCU 2023-REVISI UPDATEDocument8 pagesRundown WORKSHOP BKCU 2023-REVISI UPDATEacengNo ratings yet
- Angio Tens in Ren in Al DostDocument18 pagesAngio Tens in Ren in Al Dostatik mayasariNo ratings yet
- PHARMACOTHERAPY ON HypertensionDocument95 pagesPHARMACOTHERAPY ON Hypertensiondiwakar4123sawNo ratings yet
- Chapter 1 - The Cardiovascular SystemDocument22 pagesChapter 1 - The Cardiovascular SystemHoa LoNo ratings yet
- Smoking Inactivity: Hypertension (High Blood Pressure)Document1 pageSmoking Inactivity: Hypertension (High Blood Pressure)Belal AymanNo ratings yet
- Cardiac Cycle Electrical Mechanical EventsDocument49 pagesCardiac Cycle Electrical Mechanical EventsJardee Datsima100% (1)
- Cardiovascular: The Least Likely To Cause Postural Hypotension?Document8 pagesCardiovascular: The Least Likely To Cause Postural Hypotension?Sandeep KannegantiNo ratings yet
- Physiology Seminar: ElectrocardiographyDocument42 pagesPhysiology Seminar: ElectrocardiographyRajesh SharmaNo ratings yet
- Bio 20Document43 pagesBio 20Samantha WalkerNo ratings yet
- Intervensi Pada Pembuluh Darah (Embolisasi)Document10 pagesIntervensi Pada Pembuluh Darah (Embolisasi)Akram BatjoNo ratings yet
- Blood Flow Mechanics (Medicalstudyzone - Com)Document31 pagesBlood Flow Mechanics (Medicalstudyzone - Com)Lordoc DoctorsaabNo ratings yet
- Advance Trauma & Cardiovascular Life Support: Siswa Susdokbangan A-18Document86 pagesAdvance Trauma & Cardiovascular Life Support: Siswa Susdokbangan A-18sahidakn100% (1)
- Checklist Adult CPR OLFU 2022Document2 pagesChecklist Adult CPR OLFU 2022ANGELICA MACASO100% (1)