C 2007)
Journal of Clinical Immunology, Vol. 27, No. 4, July 2007 (�
DOI: 10.1007/s10875-007-9084-0
Host Innate Immune Response to Mycobacterium tuberculosis
KAMLESH BHATT1 and PADMINI SALGAME1,2
the prevalence of HIV infection is high (4). The situation
is further complicated by a worldwide increase in drug
resistant and MDR-TB, and the recent reports of XDR
TB (5). Thus, the resurgence of TB truly constitutes a
global health crisis (6).
Tuberculosis begins with the inhalation of Mtbcontaining aerosols into the pulmonary alveoli. Here, the
bacteria bind to phagocytic receptors and enter resident
alveolar macrophages, dendritic cells, and monocytes recruited from the bloodstream. Besides expressing phagocytic receptors, macrophages and dendritic cells also express Toll-like receptors (TLRs) that recognize conserved
molecular patterns expressed on pathogens (7–9). Ligation of TLRs by these pathogen-specific ligands initiates
a signal transduction pathway in the host cell that culminates in the activation of NFκb and the induction of
cytokines and chemokines (10) that are crucial to eliciting the adaptive immune response against the pathogen.
Consequently, activation of TLR is an important link between innate cellular response and the subsequent activation of adaptive immune defense against microbial
pathogens.
As depicted in Fig. 1, a small percentage of individuals,
despite exposure to Mtb, remain uninfected, most likely
due to the expression of high innate immunity. However,
in the majority of individuals who are exposed to Mtb,
the innate response cannot protect from infection, and
effector Th1 cytokines of the adaptive immune response
are necessary to restrict bacterial growth and mediate protection. The adaptive immunity generated in these people,
although protective, nonetheless does not induce sterilizing immunity. These individuals therefore remain latently
infected, and are vulnerable to disease reactivation when
their immune surveillance weakens or when their immune
response is compromised. Reactivation tuberculosis contributes significantly to the morbidity and mortality associated with the disease (11, 12), and is believed to account
for a substantial portion of TB cases in HIV-infected individuals (13). In another small proportion of individuals,
infection leads directly to primary tuberculosis due to a
Received February 9, 2007; accepted February 14, 2007
Published online: 16 March 2007
This review focuses on recent progress in our understanding
of Mycobacterium tuberculosis survival in macrophages, the
interaction of M. tuberculosis with Toll-like receptors (TLRs)
and the establishment of the link between innate and adaptive
immunity, and TLRs and interferon-γ -mediated antimicrobial
pathways in macrophages. We also propose a paradigm that
TLR2 signaling regulates the magnitude of the host Th1 response
leading to either M. tuberculosis persistence and latent infection
or replication and disease.
KEY WORDS: Mycobaterium tuberculosis; innate immunity; TLR2;
dendritic cells; macrophages.
INTRODUCTION
The naissance of innate immunity was the description of
macrophage phagocytosis by Metchnikoff (1). Today, the
science of innate immunity is more than just phagocytosis.
The innate immune response comprises several different
cell types, has its own receptor system to recognize the
presence of pathogens, and is a key to the initiation of
an adaptive immune response in the host. No wonder,
successful pathogens have evolved ways to evade innate
immune killing in order to find a niche in the host. In this
review, we will discuss host innate immunity generated
in response to the pathogen, Mycobacterium tuberculosis
(Mtb).
Mtb infects approximately one-third of the world’s population (2). Close to eight million new cases of tuberculosis occur each year, accounting for approximately 7%
of all deaths and 26% of all avoidable adult deaths in
developing countries (3). Despite the implementation of
TB control programs, case rates continue to soar where
1 Department
of Medicine, Centre for Emerging Pathogens, UMDNJNew Jersey Medical School, MSB A902, 185 South Orange Avenue,
Newark, New Jersey, 07101.
2 To whom correspondence should be addressed to; e-mail:
salgampa@umdnj.edu.
347
C 2007 Springer Science+Business Media, LLC
0271-9142/07/0700-0347/0 �
�348
BHATT AND SALGAME
High innate immunity
Innate immunity
Mtb clearance
No infection
Defective adaptive immunity
Disease <10%
Containment > 90%
Innate immunity
Adaptive immunity
Latent Infection
Immunosuppression
Disease
Reactivation < 10%
Fig. 1. Three possible outcomes of Mtb exposure. In some individuals, Mtb is eliminated by the host immediately upon
inhalation. The frequency and the cause of such spontaneous healing are not certain. In the second and the largest group of
individuals, infection is contained as a result of successful granuloma formation, a function of strong innate and adaptive
immune response by the host, which results in latent infection. In this group, reactivation of latent infection can occur due
to factors such as aging or the immunocompromised status of the host. In a small number of infected individuals, adaptive
immunity fails and they develop primary tuberculosis.
failure of their adaptive immune response to control the
initial bacterial replication.
In the last several years, we have gained a better appreciation regarding host innate immune response to Mtb,
although much needs to be learned regarding the nature of
the innate response that prevents establishment of Mtb infection. This review focuses on our current understanding
of the regulation of host innate immune response to Mtb
and how it interfaces with the adaptive immune response.
The review is not all-inclusive, and only areas where substantial progress has been made will be addressed. Specifically, we will discuss (i) Mtb entry and subsequent survival inside macrophages; (ii) Mtb interaction with innate
receptors, specifically TLRs; (iii) Mtb-induced cytokine
and chemokine induction in macrophages and dendritic
cells; (iv) maturation and migration of dendritic cells—a
key step that links innate and adaptive anti-Mtb immunity; (v) modulation of innate immunity by effectors of the
adaptive immune response. Finally, in closing, we will explore the evolving paradigm that innate immune response
generated in the host in response to Mtb infection is not
only important for initiating anti-Mtb immunity, but the
innate response concomitantly also activates regulatory
pathways in the host. Whether the regulatory mechanisms
activated are important for controlling the magnitude of
the host immune response to prevent immunopathology,
or whether this is a virulence strategy for the TB bacillus
to persist in the host will be discussed.
MTB PHAGOCYTOSIS AND SURVIVAL INSIDE
MACROPHAGE
Macrophages lining the alveolar spaces of the lungs
represent the first line of defense upon aerosol infection of
the host with Mtb. In vitro studies have implicated comple-
ment receptor (CR)3 as a major receptor on macrophages
for phagocytosis of Mtb (14). Nonetheless, several other
macrophage surface receptors, such as CR1, CR4, Mannose receptor, CD14, and Scavenger receptors can also
recognize and bind Mtb in vitro (15). Pulmonary surfactant protein A (Sp-A) too enhances Mtb uptake by human
macrophages (16, 17). In this context, it is worth noting
that although CR3 was determined as the primary mode
of macrophage entry for Mtb in vitro, mice lacking CR3
exhibited similar bacterial burden and host response to
that of CR3-sufficient mice (18). Cholesterol accumulates
at the site of Mtb entry into macrophages, and depleting
cells of cholesterol prevent Mtb internalization (19). This
indicates that perhaps cholesterol accumulation around
phagocytic receptors rather than the nature of the receptor itself dictates Mtb uptake. Whether in vivo a similar
relocation of cholesterol occurs at sites of Mtb entry into
macrophages and whether it provides a distinct advantage
to the TB bacillus remains to be determined.
Once inside the host cell, Mtb successfully evades
destruction by the innate microbicidal machinery. Armstrong and Hart in papers published in the early 1970s (20,
21) shaped our understanding of how Mtb might persist
in the host. Their work showed that Mtb vacuoles did not
fuse with the lysosomal compartment. Substantive work
from several laboratories has built on this seminal observation to provide a detailed insight into the molecular
events that arrest the maturation of the Mtb phagosome
and prevent its further biogenesis and acquisition of lysosomal components. The early trafficking pattern of the
Mtb phagosome is normal and exhibits fusion with certain early endosomal compartments, since both iron (22,
23) and glycosphingolipids (24) are found associated with
the Mtb phagosome. The arrested phagosome, however,
lacks the vacuolar ATPase and lysosomal hydrolases (25).
Subsequent studies that monitored the trafficking pattern
Journal of Clinical Immunology, Vol. 27, No. 4, 2007
�HOST INNATE IMMUNE RESPONSE TO
349
m. tuberculosis
of the Mtb phagosome showed that the arrest occurs between the acquisition of the endocytic vesicles Rab5 and
Rab7. The Mtb phagosome is associated with Rab5 (26),
but not Rab7 (27), and furthermore exhibits reduced recruitment of the early endosomal autoantigen 1 (EEA1)
(28), an effector molecule of Rab5 required for organelle
tethering and delivery of lysosomal hydrolases, cathepsins, and vacuolar ATPases from the trans golgi network
to the phagosome. The Mtb phagosome also lacks a specific type III phosphatidylinositol 3-kinase, hVPs34 (29)
whose activation product phospatidylinositol 3-phosphate
aids the retention of EEA1 to the endosomal membrane
(29).
How and what components of Mtb block the Mtb
phagosome from undergoing the typical phagosome biogenesis? The arrest of the Mtb phagosome at the Rab 5
stage and its inability to proceed through the maturation
pathway, at least partly, results from Mtb-induced inhibition of sphingosine kinase activity and subsequent Ca2+
signaling pathway in the cell, a step necessary for recruitment of hVPs35 to membranes of organelles (30). Another
study reported that maturation of the Mtb phagosome is
impeded because Mtb suppresses phagosomal actin assembly (31). Yet another study determined that the Mtb
phagosome arrest was dependent on its initial fusion with
early endosomes and acquisition of iron (32). Manosylated lipoarabinamannan (ManLAM), the Mtb analog of
host phophatidylinositol-3 phosphate is responsible for
actively inhibiting Mtb phagosome from fully maturing
and acquiring lysosomal hydrolases (33, 34). Indeed, it
has been shown that phagocytosis of Mtb via binding of
its cell surface LAM to the mannose receptor on human
macrophages led to the non-fusogenic phenotype of the
Mtb phagosome (35). Interestingly, other Mtb lipids such
as PIMs enhance Mtb phagosome fusion with early endosomes, possibly providing the phagosome access to host
nutrients (36). Besides lipids, a protein from Mtb, protein
kinase G (PknG) has also been implicated in interfering
with the transfer of Mtb phagosome to the lysosomal compartment (37).
Our understanding of Mtb phagocytosis, the biogenesis of Mtb phagosome, and intracellular growth of Mtb is
almost entirely derived from studies examining interaction of Mtb with macrophages. However, it is necessary
to also understand the handling of Mtb inside dendritic
cells, since in response to an aerosol challenge with Mtb,
dendritic cells take up Mtb, and as will be discussed later,
are crucial to linking the innate and adaptive immune
responses. Besides the expression of CR3 and mannose
receptor, dendritic cells are endowed with an additional
phagocytic receptor for binding Mtb. Dendritic cells express the C-type lectin, DC-SIGN (DC-specific intercel-
Journal of Clinical Immunology, Vol. 27, No. 4, 2007
lular adhesion molecule-grabbing nonintegrin), and Mtb
can bind DC-SIGN through manLAM expressed on their
surface. A comparative analysis of Mtb survival within human macrophages and dendritic cells revealed that unlike
macrophages, dendritic cells did not support intracellular
growth of Mtb (38, 39). Despite being a key player in the
innate response to Mtb, we know very little regarding the
trafficking of Mtb vacuole inside dendritic cells; except
for a study that reported that endosomal trafficking is significantly reduced compared to that in macrophages (39).
Clearly, more detailed studies examining the intracellular
fate of Mtb inside dendritic cells are needed.
It must be emphasized that Mtb replication in the
macrophage is also controlled at the level of host factors.
Expression of a candidate gene IntracellularPathogenResistance (lpr1) within the sst1 locus limits Mtb multiplication in the host (40). Variants in the human equivalent of the lpr1 gene SP110 were shown to be associated
with genetic susceptibility to TB in a study of families
in West Africa (41). Another association study in human
TB, also in West Africa, however, found no association of
human pulmonary TB with SP110 variants (42). Undoubtedly, more studies in genetically different populations are
needed to equivocally determine the role of SP100 and
other potential candidate genes in susceptibility to TB.
MTB INTERACTION WITH TLRS
Engagement of TLR by Mtb ligands is an early event
in the interaction of Mtb with its host cell. Accumulating data indicate that Mtb expresses a large repertoire
of TLR2 ligands. The 19-kDa lipoprotein (LpqH), a secreted antigen of Mtb, was the first Mtb ligand shown
to interact specifically with TLR2 to induce TNFα and
nitric oxide production from both murine and human
macrophages (43). In addition, the 19-kDa lipoprotein
is a major inducer of interleukin (IL)-12 production in
human monocytes (43). LprA (Rv1270) (44) and LprG
(Rv1411c) (45) are two other mycobacterial lipoproteins
that are TLR2 agonists. In addition to lipoproteins, lipomannan (46) and phosphatidyl-myo-inositol mannoside
(PIM) (47, 48) also interact with TLR2 to initiate cellular activation (48). However, with regards to PIMs,
Abel et al. (49) demonstrated that PIM structures can
also elicit cellular activation via TLR4. They showed
that PIM was able to induce NFκB activation in a dosedependent manner in stable TLR4 and MD-2 Ba-F3 transformants. A systematic biochemical characterization of
four acyl forms of lipomannan (LM) from M. bovis BCG
that differed in their degree of acylation, indicated that
only the triacylated LM was a potent TLR2 agonist (50).
�350
Interestingly, ManLAM derived from virulent Mtb fails
to activate either TLR2 or TLR4-transfected cells (51). In
contrast, AraLAM purified from fast-growing mycobacteria is capable of TLR2-mediated cellular activation
(51).
Studies aimed at determining the requirement of TLR4
in controlling Mtb infection following an aerosol challenge showed that lack of TLR4 did not compromise host
resistance to TB (52, 53). However, a high dose of Mtb
infection did lead to enhanced susceptibility in the absence of TLR4 signaling (49). It is interesting that despite
a large collection of TLR2 agonists on the TB bacillus,
murine studies indicate that TLR2 is not essential for host
resistance against tuberculosis. In a model of low-dose
aerosol infection, TLR2 (53, 54) deficiency did not affect
host defense against Mtb infection. However, in one of
the two studies (53) with high-dose aerosol infection, a
role for TLR2 in host resistance was revealed. The TLR2deficient mice were not compromised in their ability to
induce Th1 immunity, but on the contrary, exhibited exaggerated immunopathology. In vitro studies have shown
that engagement of TLR2 with Mtb ligands induces inhibition of macrophage MHC class II antigen presentation (55) and also blocks macrophage responsiveness to
IFNγ (56, 57). Together with the in vivo studies, these in
vitro findings that TLR2 signaling negatively modulates
macrophage functions point to the need for future studies
designed to examine whether the negative signaling from
TLR2 curtails Th1 activation, and whether this is important for balancing protection and immunopathology in the
host.
Our studies examining the in vitro interaction of TLR
with live Mtb reported that in response to Mtb, dendritic
cells secreted copious amount of IL-12, while the secretion was limited in infected macrophages. The study
also reported that Mtb induced rapid and significantly
higher remodeling at the IL-12p40 promoter in dendritic
cells in comparison to macrophages. The mechanism
behind the differential remodeling at the IL-12p40 promoter and subsequent IL-12 release was shown to be due
to differences in TLR usage by macrophages and dendritic cells. Mtb induced IL-12 secretion from dendritic
cells in a TLR9-dependent manner while in macrophages
it was TLR2-dependent (58). Consistent with this, the
greatest effect on the progression of tuberculosis disease
was seen in mice doubly deficient in TLR2 and TLR9
(59).
Although IFNγ is undoubtedly necessary for resistance
against Mtb infection (60), it is of interest that there exist
antimycobacterial pathways that are independent of IFNγ
and are induced by TLR in human macrophages. For example, it has been known for some time that activation
BHATT AND SALGAME
of the Vitamin D3 pathway controls Mtb replication in
human macrophages (61). Also, it had been documented
that Vitamin D deficiency is a risk factor for tuberculosis
(62). Only recently, however, Modlin and colleagues deciphered the mechanism for Vitamin-D3-mediated antimicrobial pathway. They demonstrated that TLR2-mediated
activation of macrophages upregulated the expression of
Vitamin D receptor and Vitamin-D-1-hydroxylase genes,
leading to the induction of the antimicrobial peptide,
cathelicidin (63). The study from Modlin’s group also
showed that African American individuals who are more
susceptible to Mtb infection and disease were not efficient in inducing the antimicrobial peptide, cathelicidin.
The TLR2-mediated innate mechanism of mycobacterial
killing provides a scientific basis for tuberculosis treatment of a century ago: exposure to sunlight. Other TLRinduced killing mechanisms may also participate in the
innate response. For instance, CpG, an activator of the
TLR9-pathway, also induces rapid antimycobacterial responses in macrophages, in a phospholipase D-dependent
manner (64). These innate mechanisms for killing Mtb
provoke future investigations of whether individuals who
never become infected with Mtb have the capacity to activate these pathways and overpower the Mtb-induced block
in phagosome maturation.
MTB-INDUCED UPSURGE OF CYTOKINE
AND CHEMOKINE SECRETION
A major consequence of Mtb interaction with the TLRs
on macrophages and dendritic cells is the burst in cytokine
and chemokine secretion. The induction of these effector
molecules regulates the formation of the granuloma and is
responsible for initiating and shaping the adaptive immune
response to Mtb. The contribution of adaptive immunity
to the evolving tubercle granuloma in the lung will not be
elaborated in this review. The reader is referred to other
reviews on the topic (65–67).
Cytokines Important for Induction of Th1 Immunity
Clearly, induction of cellular Th1 immunity is critical for protection against tuberculosis as evidenced by
enhanced disease in the HIV-infected (68) and from experiments of nature where individuals carrying defective
genes for IFNγ R and IL-12R (69) are exquisitely susceptible to intracellular pathogens, including mycobacteria. Currently, there are three well-defined cytokines that
steer naı̈ve T cells toward Th1 commitment (70). IL-12
was the first cytokine to be described with potent Th1
promoting attributes, followed by the discovery of IL-23
Journal of Clinical Immunology, Vol. 27, No. 4, 2007
�HOST INNATE IMMUNE RESPONSE TO
m. tuberculosis
(shares the p40 component with IL-12) and the recent
addition of IL-27 to this list. Work from several laboratories has revealed that the three cytokines together orchestrate Th1 responses, with IL-12 being the prototypic
and dominant cytokine that affects both the induction and
maintenance of Th1 immunity. IL-23, on the other hand,
has activities on memory T cells and IL-27, secreted prior
to IL-12 by antigen-presenting cells, is involved in Th1
initiation.
In patients with tuberculosis pleuritis, a clinical form
of disease that is mostly self-healing, high IL-12 levels
were found in the pleural fluid (71). Two studies comparing murine macrophages and dendritic cells demonstrated
that dendritic cells release significantly higher IL-12 than
did macrophages in response to live Mtb (72, 73). In
vitro, Mtb-infected dendritic cells also primed naı̈ve T
cells toward Th1 development, while macrophages did
not; though, IL-23-secreting macrophages were capable
of inducing Mtb-specific Th1 response (74).
Early studies in the murine model of tuberculosis
clearly demonstrated that the cytokine IL-12 that is necessary to drive Th1 responses and IFNγ —the effector
molecule of the Th1 response—were both necessary for
protection against Mtb infection. Mice deficient in the p40
component of IL-12 or in IFNγ (GKO) were both highly
susceptible to Mtb infection. Exogenous supplementation
of IL-12 at the onset of disease led to reduction in bacterial
burden and delayed the lung pathology in the relatively
susceptible Balb/C strain of mice (75). However, IL-12
supplementation did not lead to enhanced protection in
GKO mice indicating that IFNγ is downstream of IL-12
and is the effector molecule mediating protection in the
host. In another study (76), the role of endogenous IL-12
was studied by neutralization with anti-IL-12 antibodies.
It was found that in Balb/C mice neutralization of IL-12
at the onset of infection led to disruption in the ability
of the host to contain infection; however, neutralization
of the cytokine after the onset of infection (third week)
did not affect bacterial replication. This suggests that the
presence of IL-12 is more critical during early infection
when anti-Mtb adaptive immunity is being shaped toward
Th1-type. However, in later studies, reconstitution of IL12-p40 gene-deficient mice with recombinant IL-12 only
during the early phase of infection was determined not
to be sufficient to provide long-term immunity, despite
early control of bacterial growth. Transfer of immune
CD4 T cells from Mtb-infected wild-type mice to Rag
−/− provided immunity against infection. However, similar reconstitution of immune CD4 T cells into Rag−/−
mice that were also deficient in IL-12-p40 failed to induce protection. This provides experimental evidence that
sustained production of IL-12 throughout the course of
Journal of Clinical Immunology, Vol. 27, No. 4, 2007
351
infection is necessary to maintain antibacterial immunity
in the host (77). A reason why this study differed from
the previous where IL-12 was shown not to be necessary for long-term immunity may probably be due to the
presence of residual IL-12 activity in the neutralization
experiments.
To further characterize whether susceptibility to Mtb
infection in the absence of p40 is due to the lack of biologically active IL-12 or is a consequence of defective IL-23
production, mice deficient in the specific components of
IL-12 and IL-23, p35 and p19, respectively, were studied.
Mice lacking p19 were able to control Mtb infection as
well as the wild-type mice (78, 79). Mice lacking p35
were able to control bacterial replication slightly better
than the p40-deficient mice (79, 80), but in comparison to
the p19 knockout mice exhibited significantly higher bacterial burden. Mice doubly deficient in p35 and p19 genes
were as susceptible as the p40-gene-deficient mice (79).
Exogenous delivery into the lung of IL-23 via adenoviral
vectors enhanced anti-Mtb immunity, upregulated IL-17
expression, and reduced bacterial burden in the lungs of
Mtb-infected mice (81). Together, these data indicate that
IL-23 is less critical for protection against Mtb, and only
provides a moderate level of protection to the host in the
absence of biologically active IL-12. On the other hand,
IL-12 has a far more vital role in the generation of protective anti-Mtb immunity.
IL-27 is also an IL-12-related cytokine and WSX-1
is a component of the IL-27R complex (82). IL-27/IL27R signaling, interestingly, exhibits both pro- and antiinflammatory properties. Infection of WSX-1−/− mice
with Mtb revealed that, in the absence of IL-27R signaling, there was a reduced bacterial burden accompanied
by enhanced CD4 infiltration into the lungs (83). Another
group examining Mtb infection in the same WSX-1−/−
mice observed increased IL-12-p40 and TNFα expression
and enhanced IFNγ production from CD4 T cells. This
group also reported reduced Mtb burden in the lungs of
infected WSX-1 knockout mice in comparison with wildtype mice. Despite restricted bacterial growth, the WSX-1
knockout mice succumbed to infection due to exaggerated
immunopathology, a scenario similar to what was first reported with Toxoplasma gondii infection in this strain of
knockout mice. Under conditions where pathogens do not
induce a Th1 response in the host, for example in Leishmania major infection of Balb/c mice, absence of WSX1 resulted in the generation of protective Th1 response
with concomitant Th2 downregulation in the host (84).
A tenet for future perusal is that the anti-inflammatory
activity of IL-27 is perhaps more critical than its Th1 promoting activity in response to pathogens that have high
Th1-inducing potential (85, 86).
�352
TNF
TNFα plays an important role in regulating the pathology of tuberculosis (87). TNFα exists in both soluble
and membrane bound forms and signals through TNFαR.
Mtb infection leads to TNFα secretion by macrophages,
dendritic cells, and T cells (60). Secretion of TNFα by
Mtb-infected macrophages is a potent mechanism to induce killing of Mtb via generation of reactive nitrogen
intermediates in conjunction with IFNγ (88). An attribute
of membrane TNFα is to induce apoptosis of the Mtbinfected alveolar macrophages (89), and thereby indirectly
contribute to the reduction of bacterial burden. TNFα’s
ability to induce alveolar macrophage apoptosis may also
be important in the cross-presentation of Mtb antigens
for CD8 cytotoxic T cell priming (90). It has also been
suggested that inhibition of TNFα-mediated macrophage
apoptosis is a virulence strategy of Mtb. Avirulent H37Ra
induced TNFα-dependent macrophage apoptosis, while
virulent H37Rv released soluble TNFR2 that reduced
TNFα activity and subsequent apoptosis of macrophages
(91). Although it needs to be examined in more detail,
TNFα has been shown to support the growth of Mtb in
human monocytes and macrophages (92).
The requirement for TNFα in host defense against Mtb
infection was demonstrated in studies which showed that
mice treated with antibody to TNFα became more susceptible to BCG infection and exhibited malformed granulomas (93). Mtb infection of mice lacking TNF receptor or neutralization of TNFα activity in mice also led
to the failure to control bacterial replication resulting in
enhanced susceptibility (94). This study indicated that
TNFα contributed to maintaining host resistance by inducing the production of reactive nitrogen intermediates
by macrophages. Later studies have indicated that TNFα
also participates in setting the chemokine circuitry in the
developing granuloma. Mice lacking TNFα had reduced
chemokine expression in lung granulomas (95–97) and
this resulted in reduced T cell infiltration into the lungs
and a failure to form a productive granuloma.
For the most part, the immunological forces that control
reactivation remain ill defined, except for the knowledge
that TNFα is a major player (98). Studies in a murine latent
model of tuberculosis from the Chan and Flynn laboratories clearly demonstrated that neutralization of TNFα
during the latent/persistent phase induced reactivation in
C57BL/6 mice, as indicated by the enhanced bacterial burden in the lungs (99). Further, histological examination
of lung tissue from TNFα-neutralized animals revealed
a disorganized granuloma with indications of a lack of
cellular turnover and increased fluid accumulation. NOS2
expression was attenuated, while IL-10 expression was
BHATT AND SALGAME
upregulated in the lungs. Immunohistochemical analysis
indicated an increased presence of apoptotic T cells and
macrophages in the lung, a feature not seen previously
in other reactivation models. The importance of TNF in
maintaining Mtb in a chronic/persistent phase in mice has
been corroborated in humans. It has been observed that the
use of anti-TNFα antibody in patients undergoing treatment for rheumatoid arthritis has resulted in reactivation
of tuberculosis in some latently infected individuals (100,
101).
Mtb-Induced Chemokines
In vitro and in vivo studies provide evidence for
the participation of chemokines in the control of TB.
It is present in the innate and adaptive immune response to Mtb (96, 102). Mtb infection of both human and murine macrophages results in the secretion
of a large number of chemokines, including CCL2,
CCL3, CCL7, CCL12, CXCL2, and CXCL10 (96). A
comparative chemokine expression analysis showed that
lung interstitial macrophages from a susceptible mouse
strain expressed significantly high levels of CXCL13
and CXCL14, while higher expression of CXCL9 and
CXCL0 was found in macrophages from the resistant
strain of mice (103). Regulation of chemokine production in macrophages is predominantly regulated by
TNFα. Mtb infection of macrophages leads to the production of TNFα which, in turn, regulates the secretion of a plethora of chemokines from macrophages,
including CCL2, CCL3, CCL4, CCL5, CXCL10, and
CXCL13 (104). Mtb-infected dendritic cells also secrete
chemokines, including CXCL9, CXCL10, CCL3, and
CCL4. CXCL10 secretion was IFNα-dependent and in
conjunction with CXCL9 and CXCL3 acted to recruit
inflammatory cells to the site of Mtb infection (105).
Studies to examine the role of chemokine and
chemokine receptors in host resistance against Mtb infection has led to conflicting results, in great part due to
redundancy in the function of chemokines and their receptors. In a mouse model of tuberculosis, it has been shown
that the first step in recruitment of cells into the lung,
specifically recruitment of immature dendritic cells and
monocytes to the site of infection, is mediated by CCR2
and, as a consequence, CCR2−/− mice (106) are more
susceptible to Mtb infection. These mice also show defective recruitment of dendritic cell to the draining lymph
nodes resulting in delayed and reduced priming of naive
T cells. However, a later study (107) indicated that susceptibility of CCR2 knockout mice to Mtb infection was
dose dependent. As seen with high dose infection, a lowdose aerosol challenge of the CCR2 knockout mice with
Journal of Clinical Immunology, Vol. 27, No. 4, 2007
�HOST INNATE IMMUNE RESPONSE TO
353
m. tuberculosis
Mtb also resulted in reduced cellular migration to the
lungs and delayed priming. However, there was no change
in bacterial burden or susceptibility to infection. Using
chimeric mice, where either the myeloid or the lymphoid
compartment was lacking CCR2, it was determined that
expression of CCR2 on macrophages and dendritic cells
was important for the recruitment of T cells to lungs (108).
However, mice deficient in CCL2/MCP-1, which is a ligand for CCR2, do not show reduced susceptibility to Mtb
infection, thereby indicating that in vivo other chemokines
such as CCL7, CCL8, and CCL12 can compensate for the
lack of CCL2/MCP-1 (109).
In addition to its expression on granulocytes and
macrophages, CCR5 is also present on immature dendritic cells and Mtb modulates its expression. Indeed, mycobacterial Hsp70 can interact with CCR5 on immature
dendritic cells and induce their maturation and the interaction also induces IL-12 secretion from dendritic cells
(110). Despite CCR5-mediated IL-12 production and the
enhanced production of CCR5 ligands, MIP-1α, MIP-1β,
and RANTES in the lungs of Mtb-infected mice, absence
of CCR5 did not affect the ability of the host to control bacterial replication in the lung (111, 112). The latter
study, in addition, observed that CCR5−/− mice exhibited
increased bacterial burden in the draining lymph nodes
(112). The intriguing possibility that CCR5 signals impede Mtb-bearing dendritic cell migration resulting in enhanced accumulation of Mtb in the draining lymph nodes
needs further scrutiny.
CCR7 expression on cells guides their migration to the
draining lymph nodes where its cognate ligands CCL19
and CCL21 are present. Indeed, Mtb infection upregulates
CCR7 expression on dendritic cells, but absence of CCR7
did not enhance bacterial replication (113). Although it
must be noted that the granulomas of CCR7−/− mice had
altered granuloma architecture with enhanced inflammation and a lack of follicular B cell architecture. How these
changes in the granuloma affect host resistance is still not
clear. As discussed in the next section, Mtb-infected dendritic cells migrate to the draining lymph nodes to initiate
an immune response. Therefore, it would be important to
determine what chemokine/receptor gradient controls the
migration of Mtb-infected dendritic cells from lungs to
draining lymph nodes.
CXCR3 is a chemokine receptor preferentially expressed on activated Th1 cells and regulates their migration in response to ligands CXCL10, CXCL9, and
CXCL11. Given the importance of Th1 in host resistance
against TB, C57BL/6 mice deficient in CXCR3 were studied following Mtb infection. Despite the ability of CXCR3
to regulate the migration of Th1 cells, absence of the
receptor did not affect Mtb replication in the host. The
Journal of Clinical Immunology, Vol. 27, No. 4, 2007
CXCR3 knockout mice, however, did exhibit a neutrophil
deficit in the granuloma. The consequence to host resistance of reduced neutrophils in the granuloma remains
unclear (114). Contrary findings were reported in a recent
study that examined mice lacking CXCR3 on the BALB/c
background. In this study, the CXCR3-deficient mice
exhibited heightened resistance to Mtb infection in the
chronic phase when compared with wild-type mice (115),
and the mice also had enhanced T cell activation (115).
The authors of the paper suggest that enhanced resistance
in BALB/cCXCR3 knockout mice could have resulted
from the absence of the immunosuppressive CXCR3–
CXCL10 chemokine gradient. Certain chemokine gradients, including CXCR3–CXCL10, have recently been
recognized as immunosuppressive and to interfere with
the formation of the immunological synapse (116). Together, these studies highlight the emerging recognition
that the chemokine circuitry activated during Mtb infection may not only regulate cellular recruitment, but also directly impact on the function of immune cells. The studies
also highlight the role of genetic differences in regulating
chemokine functions.
IL-10
Dendritic cells and macrophages in response to Mtb
produce the immunosuppressive and anti-inflammatory
cytokine IL-10. Interestingly, dendritic cells secrete substantial IL-12 in response to Mtb infection and can prime
naive T cells toward Th1-type, despite concomitant secretion of IL-10 (73, 117). IL-10-secreting CD8 suppressor/regulatory T cells are associated with susceptibility to
Mtb infection (118) and T cell expressing both IFNγ and
IL-10 have been isolated from the bronchoalveolar lavage
fluid of TB patients (119). Additionally, depressed T-cell
IFNγ responses in pulmonary tuberculosis was shown to
be associated with the induction of IL-10 from monocytes
(120). Interestingly, in patients with pleural TB, considered as the resistant and self-healing form of the disease,
IL-10 is found along with IFNγ at sites of infection in
the pleural fluid (121). In vitro, IL-10 downregulates the
production of IL-12 in human monocytes infected with
Mtb (122). Also, IL-10 down modulates the activity of
CD4 and CD8 T cells via downregulation of costimulatory molecules on macrophages (123). In addition, IL-10
inhibits the proliferation of IFNγ producing T cells and γ δ
T cells (124). Although absence of IL-10 did not enhance
resistance to Mtb infection in IL-10 knockout mice (125),
transgenic over-expression of IL-10 resulted in reactivation of chronic disease (126). Similarly, expression of human IL 10 in mice under the control of MHC II promoter
enhanced the susceptibility to disease, independent of
�354
T-cell-derived IL-10. The Mtb-infected macrophages
from these transgenic mice exhibited reduced antimycobacterial capacity (127). That IL-10 may have a role
in TB is suggested by the fact that polymorphism in
murine SLC11 A1, a tuberculosis susceptibility locus,
has been associated with variation in IL-10 production
(128). Together, these data suggest that IL-10 is induced
by Mtb and suppresses the generation anti-Mtb immunity.
However, Th1 cytokines are often found along with IL10. Perhaps the relative quantities of the two cytokines
determine whether Th1 immunity is suppressed or not.
DENDRITIC CELL MATURATION, MIGRATION,
AND ANTIGEN PRESENTATION
Recent work from several laboratories has focused on
dissecting the role of dendritic cells in Mtb infection.
Upon its interaction with Mtb, dendritic cells undergo a
repertoire of phenotypical changes, a process termed as
maturation. This process, which is TLR-dependent, brings
forth three major phenotypic changes in dendritic cells:
upregulation of costimulatory molecules-CD40, B7.1 and
B7.2, heightened expression of adhesion molecules, and
upregulation of chemokine receptor—CCR7. Whereas
immature dendritic cells are efficient at Mtb phagocytosis
and exhibit enhanced microbicidal property, maturation
endows them with the role of an efficient antigen presenter
and initiator of adaptive immune responses (129).
Following Mtb phagocytosis and concomitant TLR activation, the next step in the development of host immunity
is the transport of pathogen from the lung to the draining lymph nodes, where the matured dendritic cells can
present antigen to naive T cells and initiate the process
of adaptive immune response. Although Mtb uptake and
engagement of TLR signaling for cellular activation occurs in macrophages and dendritic cells, only the latter
cell type was shown to acquire the capacity to upregulate CCR7 expression and migrate to draining lymph
nodes (130). Consistent with this study that tracked intratracheally instilled cells, endogenous lung dendritic cells
also exhibited similar migratory property. Following intratracheal infection of mice with GFP-expressing BCG,
dissemination of mycobacteria from the lung was initiated by the migration of infected dendritic cells to the
draining lymph nodes (131), despite predominant infection of alveolar macrophages. Another study in BCGinfected mice also demonstrated that dendritic cells, and
not macrophages, were the antigen-presenting cells responsible for priming naı̈ve T cells (132). Direct evidence
for the role of dendritic cells as the priming APC for initiating pulmonary immunity came from the study where
BHATT AND SALGAME
mice depleted of CD11c + dendritic cells exhibited delayed CD4 responses to Mtb and worsening disease (133).
It has been argued that in addition to ferrying antigen for
T cell priming, migration of dendritic cells to the lymph
nodes may also aid in Mtb dissemination (131).
Are other cell types involved in transporting Mtb antigens to the draining lymph nodes? Indeed, a recent report implicates neutrophils as the carrier of live BCG
following intradermal vaccination from peripheral tissue
to the DLN capsule (134). Whether neutrophils participate in antigen transport during a pulmonary infection
with Mtb would be worth investigating, particularly since
neutrophils appear to marginally influence early immune
responses and the architecture of the ensuing granuloma
(135, 136). Following Mtb infection, there is an influx
of macrophages and dendritic cells from the periphery
into the lung. The relative contribution of interstitial
versus the newly recruited dendritic cells in Mtb transport from lung to the draining lymph nodes is also not
clear. However, absence of CCR2 was shown to impair
macrophage and dendritic cells trafficking into the infected lungs resulting in susceptibility to Mtb infection
(108), suggesting that dendritic cells recruited to the lung
may also function to carry Mtb to the draining lymph
nodes.
Collective data indicate that dendritic cells are the
antigen-presenting cells that migrate to the draining lymph
nodes, and process and present Mtb antigens on MHC
Classes I and II to naı̈ve CD4+ and CD8+ cells, respectively. This review will not address the mechanisms of
antigen processing and presentation and other molecular
events controlling T cell activation. However, we discuss
here one study from Kaufman’s group that demonstrated
a detour pathway for how antigens of Mtb, presumably
confined within the phagosome, are delivered to Class I
molecules. This study demonstrated that dendritic cells
take up apoptotic vesicles containing Mtb, the vesicles
are then degraded in an endosomal-dependent manner
and Mtb antigens are cross-presented on MHC Class I
molecules to CD8 T cells (137).
Since maturation and migration of dendritic cells is
such a key step in linking innate and adaptive immunity, it is not surprising that Mtb negatively interferes
with this step. IL-1β release from mycobacteria-infected
antigen-presenting cells inhibits dendritic cell maturation (138) and virulent Mtb has been reported to impair the maturation of monocyte derived dendritic cells
(139). The migration of dendritic cells appears to be regulated to some degree by IL-12p40 homodimers (140).
Whether IL-10, which can impede dendritic cell migration (141), functions by downregulating the p40 homodimers is worth considering. In addition, one also needs
Journal of Clinical Immunology, Vol. 27, No. 4, 2007
�HOST INNATE IMMUNE RESPONSE TO
355
m. tuberculosis
to examine whether in human infection Mtb interference with the dendritic cell maturation and migration
process is dependent on the degree of virulence of the
infecting clinical strain and its ability to induce IL-10
production.
timicrobial contents of the lysosomal compartment (148).
Whether autophagy or more specifically “immunophagy,”
(a term coined by Deretic to define the specialized function
of autophagy in host immunity (147)) restricts Mtb growth
in human macrophages and whether innate immune signaling pathways such as TLRs induce immunophagy are
all very significant questions that need to be addressed.
MODULATION OF INNATE IMMUNITY BY EFFECTORS
OF THE ADAPTIVE IMMUNE RESPONSE
OTHER INNATE IMMUNE CELLS
In effect, despite the early induction of chemokines
and cytokines from macrophages, Mtb is able to skillfully avoid the innate antimicrobial defense mechanisms
of the macrophage and find a safe niche in the phagosome for intracellular growth. IFNγ , an effector molecule
of the adaptive immune response, halts this unimpeded
growth of Mtb in the macrophage (60). Although it is clear
that IFNγ is highly effective in restricting mycobacterial growth in macrophages (60), the mechanisms through
which this is achieved is not fully understood. NOS2mediated antibacterial pathway is one mechanism that has
been extensively studied in the murine model of tuberculosis, wherein it has been demonstrated that IFNγ , in conjunction with TNF, upregulates NOS2 and the production
of reactive nitrogen intermediates within the phagolysosome, resulting in Mtb killing (142). Nitric oxide also
reacts with glutathione to form s-nitrosoglutathione that is
toxic to Mtb (143). Despite this accumulated evidence of
IFNγ -mediated antimycobacterial activity in the murine
model, the Mtb killing mechanism in human macrophages
is less clear (144). Individuals with mutations in the
IFNγ receptor are more susceptible to mycobacterial infections suggest that IFNγ -mediated antimycobacterial
pathways are active in human macrophages (69). Alveolar macrophages of tuberculosis patients express NOS2,
and isolation of NOS2-expressing macrophages exhibit
antimycobacterial activity in vitro, which can be abolished
in the presence of NOS2 inhibitors (145). Thus, whether
NOS2-mediated pathway is active in human macrophages
remains an open question and awaits better methodologies
for studying the enzyme.
Recent evidence indicates that IFNγ induced LRG-47,
a GTP-binding protein has a principal role in the ability
of the host to control Mtb replication, since mice lacking
LRG-47 are highly susceptible to Mtb infection (146).
Based on several elegant works, autophagy, originally
defined as a cellular homeostatic process, is emerging
as a powerful host defense machinery of innate immune
cells (147). IFNγ , through enhancement of LRG-47 activity, was shown to induce autophagy in Mtb-infected
macrophages, which resulted in revoking the restriction
on Mtb phagosome maturation and delivery of the an-
Journal of Clinical Immunology, Vol. 27, No. 4, 2007
Besides macrophages and dendritic cells, γ δ T cells,
NK cells, and NKT cells also participate in the innate
immune response to TB. Murine studies have indicated
that the induction of γ δ T cell in the immune response
against TB precedes that of conventional CD4 and CD8
cells and hence plays an important role in modulating the
effector response against tuberculosis. Following infection, the early recruitment of cells to the lung is mediated by the chemokines, CXCL2 and CXCL10, and the
cytokine, IL-12 released by macrophages and dendritic
cells in the lungs (149). Once activated, γ δ T cells secrete IFNγ and TNFα. The production of these cytokine
strengthens the bactericidal capacity of macrophages by
induction of NOS2. Recently, it has been shown that γ δ
T cells secrete IL 17 in response to IL 23 secreted by
dendritic cells, thereby implicating them as a main player
in the resistance against infection at the initial stage (150).
Response of mice deficient in γ δ T cells to Mtb infection
is dependent on the dose and the route of infection. These
knockout mice are able to contain Mtb infection with a
low inoculum; however, infection with a higher inoculum of Mtb administered intravenously resulted in the
formation of pyogenic granulomas, indicating that a role
for these cells is perhaps in cellular traffic during infection
(151, 152). In these experiments with high dose of virulent
Mtb, the lung pathology indicated enhanced migration of
neutrophils and increased size of granuloma thereby indicating a role of γ δ T cells in granuloma formation and
mycobacterial containment (152).
The antigen specificity of murine γ δ has not been well
studied. However, it has been shown that murine γ δ cells
do not respond to phosphate antigens, which are recognized by human γ δ cells. Upon contact with Mtb, γ δ cells
have been shown to secrete IL-2 and exhibit cytolytic
function and hence involved in innate immune effector
mechanism (153). In both humans and primates, antigenspecific γ δ cells recognizing phosphoantigens have been
documented and have been shown to generate a memory
response (154, 155). Loss of Vγ 9 + /Vγ δ2 + subset of
γ δ T cells was shown to be correlated with tuberculosis
(156).
�356
BHATT AND SALGAME
NK cells are recruited to the lungs early during Mtb
infection. There they are known to expand and become a
primary source of IFNγ . Activated NK cells are known to
cause lysis of infected macrophage by utilizing NK cell receptor in TLR-dependent manner (157). NK cell depletion
studies have shown no change in bacterial burden (158).
However, recent studies (159) indicate that NK cells provide resistance during early Mtb infection via production
of IFNγ . The IFNγ activated macrophage in a NOS2dependent manner and also by regulating neutrophil migration to the lung for controlling lung inflammation. Future experiments defining the exact contribution of NK
cells and the IFNγ secreted from them to innate immunity would help understand whether NK cell activation
has a role in preventing infection following exposure to
Mtb.
NKT cells are TCR-expressing T cells which also express the NK cell marker NK1.1. In mice, NKT cells
are mainly represented by Vα14 NKT cells, while in humans, there is a homologous population of Vα24 NKT
cells. NKT cells are known to recognize nonpeptide antigens in the context of CD1d. Role of NKT cells in tuberculosis has been studied in both humans and mice.
Human Vα24-restrcited NKT cells are activated by αgalactosylceramide. CD1d-restricted NKT in the presence
of α-galactosylceramide cells restrict the growth of Mtb
in a granulolysin-dependent manner (160). It has been
shown that NKT cells induce a granulomatous response
to a glycolipid fraction of Mtb cell wall (161). This finding
is further supported by the fact that α-galactosylceramideactivated NKT cells contribute to enhanced resistance
against Mtb infection (162).
Fig. 2. A paradigm for how the innate immune response to Mtb regulates the adaptive immune response. Initially,
Mtb survives and replicates inside macrophages since it can prevent fusion of its phagosome with the lysosomal
compartment. Concomitantly, dendritic cells capture Mtb, undergo maturation, and migrate to the draining lymph
nodes. Adaptive response is initiated in the draining lymph nodes wherein naı̈ve antigen-specific T cells are primed
by dendritic cells to Th1 and cytotoxic effector cell types. Mycobactericidal function of macrophages is dependent
on IFNγ , initially produced by innate immune cells such as NK cells and later on provided by effector T cells. The
secreted IFNγ promotes phagolysosomal fusion and enhances Mtb killing. TLR2-mediated innate IL-10 is released
during the induction of innate immune response and subsequent Th1 induction. The role of the innate IL-10 is to
control the magnitude of the Th1 response by either down modulating antigen-presentation function or by inducing
T regulatory cells. The TLR2/IL-10 axis, on the one hand, is important for allowing Mtb to achieve the latent state
and, on the other hand, may also cause excessive immunosuppression leading to disease. The unbroken lines indicate
that experimental evidence is available and dashed lines indicate that it is speculative and is an area for future
investigation.
Journal of Clinical Immunology, Vol. 27, No. 4, 2007
�HOST INNATE IMMUNE RESPONSE TO
357
m. tuberculosis
There is still much to learn regarding the contribution
of γ δ T cells, NK cells, and NKT cells to the overall innate
immune protection against TB in humans. A next step is
to study these cells in the context of protection against
clinical strains of Mtb in humans.
outcome of Mtb exposure is latent infection or tuberculosis disease.
ACKNOWLEDGMENTS
This work was supported in part by the NIH grants
AI-49778 and AI-55377 to PS.
CLOSING THOUGHTS
An emerging principle in intracellular parasitism is that
successful pathogens such as Mtb have acquired the ability
to persist in the host without always inducing disease and
mortality (163). The strategy on the part of Mtb is to
induce sufficient Th1 immunity in the host to control its
replication but not result in its complete eradication. The
advantage to the host is minimal collateral damage to
lung tissue. Thus, Mtb remains dormant in the host for
decades, in a sort of symbiotic relationship. Under certain
altered conditions in the host, Mtb will reactivate and
cause immunopathology such as lung cavitation, which
increases its infectivity and thereby maintains the cycle of
transmission to new hosts.
Although Mtb interacts with several different TLRs on
host cells, we posit that to establish a latent infection Mtb
specifically usurps the innate TLR2 signaling in the host
to blunt Th1 immune responses. Supporting evidence for
the paradigm include (i) Mtb possess a large gamut of
ligands for TLR2; (ii) Mtb/TLR2 interaction suppresses
macrophage functions; (iii) innate IL-10 secretion by dendritic cells and macrophages in response to live Mtb is
TLR-2 dependent; and (iv) absence of TLR2 results in
exaggerated immunopathology in the host. The mechanisms for limiting Th1 response may include inhibition of
antigen-presentation functions and induction of T regulatory cells (Fig. 2).
A corollary to the paradigm is that virulent strains can
tip the balance toward immunosuppression using the same
TLR2 signaling pathway. Although there is no evidence
that TLR2 interaction is necessary for protection against
Mtb disease, it must be pointed out that these conclusions
are drawn from studies performed with laboratory strains
of Mtb. It is highly probable that the interaction of clinical strains of Mtb with the TLR2 complex does result
in potent immunosuppression in the host. In this regard,
it would be interesting to determine if the immunosuppressive cytokines induced by the phenolic glycolipid of
the virulent Beijing strains (164) is TLR2-mediated, and
whether the induction of T regulatory cells present in TB
patients (165, 166) is TLR2-dependent.
Clearly, future studies should investigate if the differing
interaction of Mtb clinical strains with the TLR2/IL-10
axis is the control switch that determines whether the
Journal of Clinical Immunology, Vol. 27, No. 4, 2007
REFERENCES
1. Metchnikoff E: Immunity to Infective Diseases. London,
Cambridge University Press, 1905
2. World Health Organization: Anti-Tuberculosis Drug Resistance in
the World: The WHO/IUTLD Global Project on Anti-Tuberculosis
Drug Resistance Surveillance. Geneva, Switzerland, World Health
Organization, 2001
3. Murray JF: Tuberculosis and HIV infection: A global perspective.
Respiration 65:335, 1998
4. De Cock KM, Chaisson RE: Will DOTS do it? A reappraisal of
tuberculosis control in countries with high rates of HIV infection.
Int J Tuberc Lung Dis 3:457, 1999
5. Pablos-Mendez A, Raviglione MC, Laszlo A, Binkin N, Rieder
HL, Bustreo F, Cohn DL, Lambregts-van Weezenbeek CS, Kim SJ,
Chaulet P, Nunn P: Global surveillance for antituberculosis-drug
resistance, 1994–1997. World Health Organization–International
Union against Tuberculosis and Lung Disease Working Group on
Anti-Tuberculosis Drug Resistance Surveillance. N Engl J Med
338:1641, 1998
6. Raviglione MC, Snider DE, Jr, Kochi A: Global epidemiology of
tuberculosis. Morbidity and mortality of a worldwide epidemic.
JAMA 273:220, 1995
7. Medzhitov R, Janeway CJ: The Toll receptor family and microbial
recognition. Trends Microbiol 10:452, 2000
8. Kaisho T, Akira S: Critical roles of Toll-like receptors in host
defense. Crit Rev Immunol 20:393, 2000
9. Takeda K, Kaisho T, Akira S: Toll-like receptors. Annu Rev Immunol 21:335, 2003
10. Aderem A, Ulevitch RJ: Toll-like receptors in the induction of the
innate immune response. Nature 406:782, 2000
11. Stead WW: Pathogenesis of a first episode of chronic pulmonary
tuberculosis in man: Recrudescence of residuals of the primary
infection or exogenous reinfection? Am Rev Respir Dis 95:729,
1967
12. Stead WW: The pathogenesis of pulmonary tuberculosis among
older persons. Am Rev Respir Dis 91:811, 1965
13. Selwyn PA, Hartel D, Lewis VA, Schhoenbaum EE, Vermuns SH,
Klein RS, Walker AT, Freidland GH: A prospective study of the
risk of tuberculosis among intravenous drug users with human
immunodeficiency virus infection. N Engl J Med 320:545, 1989
14. Schlesinger LS, Bellinger-Kawahara CG, Payne NR, Horwitz MA:
Phagocytosis of Mycobacterium tuberculosis is mediated by human monocyte complement receptors and complement C3. J Immunol 144:2771, 1990
15. Ernst JD: Macrophage receptors for Mycobacterium tuberculosis.
Infect Immun 66:1277, 1998
16. Beharka AA, Gaynor CD, Kang BK, Voelker DR, McCormack
FX, Schlesinger LS: Pulmonary surfactant protein A up-regulates
activity of the mannose receptor, a pattern recognition receptor
expressed on human macrophages. J Immunol 169:3565, 2002
�358
17. Gaynor CD, McCormack FX, Voelker DR, McGowan SE,
Schlesinger LS: Pulmonary surfactant protein A mediates enhanced phagocytosis of Mycobacterium tuberculosis by a direct interaction with human macrophages. J Immunol 155:5343,
1995
18. Hu C, Mayadas TN, Tanaka K, Chan J, Salgame P: Mycobacterium
tuberculosis infection in complement receptor 3-deficient mice. J
Immunol 165:2596, 2000
19. Gatfield J, Pieters J: Essential role for cholesterol in entry of mycobacteria into macrophages. Science 288:1647, 2000
20. Armstrong JA, Hart PD: Response of cultured macrophages to
M. tuberculosis with observations of fusion of lysosomes with
phagosomes. J Exp Med 134:713, 1971
21. Armstrong JA, Hart PD: Phagosome–lysosome interactions in cultured macrophages infected with virulent tubercle bacilli. Reversal
of the usual nonfusion pattern and observations on bacterial survival. J Exp Med 142:1, 1975
22. Sturgill-Koszycki S, Schaible UE, Russell DG: Mycobacteriumcontaining phagosomes are accessible to early endosomes and reflect a transitional state in normal phagosome biogenesis. EMBO
J 15:6960, 1996
23. Clemens DL, Horwitz MA: The Mycobacterium tuberculosis
phagosome interacts with early endosomes and is accessible to
exogenously administered transferrin. J Exp Med 184:1349, 1996
24. Russell DG, Dant J, Sturgill-Koszycki S: Mycobacterium aviumand Mycobacterium tuberculosis-containing vacuoles are dynamic,
fusion-competent vesicles that are accessible to glycosphingolipids
from the host cell plasmalemma. J Immunol 156:4764, 1996
25. Sturgill-Koszycki S, Schlesinger PH, Chakraborty P, Haddix PL,
Collins HL, Fok AK, Allen RD, Gluck SL, Heuser J, Russell DG:
Lack of acidification in Mycobacterium phagosomes produced by
exclusion of the vesicular proton-ATPase. Science 263:678, 1994
26. Clemens DL, Lee BY, Horwitz MA: Deviant expression of Rab5 on
phagosomes containing the intracellular pathogens Mycobacterium
tuberculosis and Legionella pneumophila is associated with altered
phagosomal fate. Infect Immun 68:2671, 2000
27. Via LE, Deretic D, Ulmer RJ, Hibler NS, Huber LA, Deretic V:
Arrest of mycobacterial phagosome maturation is caused by a block
in vesicle fusion between stages controlled by Rab5 and Rab7. J
Biol Chem 272:13326, 1997
28. Fratti RA, Backer JM, Gruenberg J, Corvera S, Deretic V: Role of
phosphatidylinositol 3-kinase and Rab5 effectors in phagosomal
biogenesis and mycobacterial phagosome maturation arrest. J Cell
Biol 154:631, 2001
29. Deretic V, Vergne I, Chua J, Master S, Singh SB, Fazio JA, Kyei
G: Endosomal membrane traffic: Convergence point targeted by
Mycobacterium tuberculosis and HIV. Cell Microbiol 6:999, 2004
30. Kusner DJ: Mechanisms of mycobacterial persistence in tuberculosis. Clin Immunol 114:239, 2005
31. Anes E, Kuhnel MP, Bos E, Moniz-Pereira J, Habermann A,
Griffiths G: Selected lipids activate phagosome actin assembly
and maturation resulting in killing of pathogenic mycobacteria.
Nat Cell Biol 5:793, 2003
32. Kelley VA, Schorey JS: Mycobacterium’s arrest of phagosome
maturation in macrophages requires Rab5 activity and accessibility
to iron. Mol Biol Cell 14:3366, 2003
33. Fratti RA, Chua J, Vergne I, Deretic V: Mycobacterium tuberculosis glycosylated phosphatidylinositol causes phagosome maturation arrest. Proc Natl Acad Sci USA 100:5437, 2003
34. Chua J, Vergne I, Master S, Deretic V: A tale of two lipids: Mycobacterium tuberculosis phagosome maturation arrest. Curr Opin
Microbiol 7:71, 2004
BHATT AND SALGAME
35. Kang PB, Azad AK, Torrelles JB, Kaufman TM, Beharka
A, Tibesar E, DesJardin LE, Schlesinger LS: The human
macrophage mannose receptor directs Mycobacterium tuberculosis
lipoarabinomannan-mediated phagosome biogenesis. J Exp Med
202:987, 2005
36. Vergne I, Fratti RA, Hill PJ, Chua J, Belisle J, Deretic V: Mycobacterium tuberculosis phagosome maturation arrest: Mycobacterial
phosphatidylinositol analog phosphatidylinositol mannoside stimulates early endosomal fusion. Mol Biol Cell 15:751, 2004
37. Walburger A, Koul A, Ferrari G, Nguyen L, Prescianotto-Baschong
C, Huygen K, Klebl B, Thompson C, Bacher G, Pieters J: Protein
kinase G from pathogenic mycobacteria promotes survival within
macrophages. Science 304:1800, 2004
38. Bodnar KA, Serbina NV, Flynn JL: Fate of Mycobacterium tuberculosis within murine dendritic cells. Infect Immun 69:800, 2001
39. Tailleux L, Neyrolles O, Honore-Bouakline S, Perret E, Sanchez
F, Abastado JP, Lagrange PH, Gluckman JC, Rosenzwajg M,
Herrmann JL: Constrained intracellular survival of Mycobacterium tuberculosis in human dendritic cells. J Immunol 170:1939,
2003
40. Pan H, Yan BS, Rojas M, Shebzukhov YV, Zhou H, Kobzik L,
Higgins DE, Daly MJ, Bloom BR, Kramnik I: Ipr1 gene mediates
innate immunity to tuberculosis. Nature 434:767, 2005
41. Tosh K, Campbell SJ, Fielding K, Sillah J, Bah B, Gustafson P,
Manneh K, Lisse I, Sirugo G, Bennett S, Aaby P, McAdam KP,
Bah-Sow O, Lienhardt C, Kramnik I, Hill AV: Variants in the SP110
gene are associated with genetic susceptibility to tuberculosis in
West Africa. Proc Natl Acad Sci USA 103:10364, 2006
42. Thye T, Browne EN, Chinbuah MA, Gyapong J, Osei I, OwusuDabo E, Niemann S, Rusch-Gerdes S, Horstmann RD, Meyer CG:
No associations of human pulmonary tuberculosis with Sp110 variants. J Med Genet 43:e32, 2006
43. Brightbill HD, Libraty DH, Krutzik SR, Yang RB, Belisle JT,
Bleharski JR, Maitland M, Norgard MV, Plevy SE, Smale ST,
Brennan PJ, Bloom BR, Godowski PJ, Modlin RL: Host defense
mechanisms triggered by microbial lipoproteins through toll-like
receptors. Science 285:732, 1999
44. Pecora ND, Gehring AJ, Canaday DH, Boom WH, Harding CV:
Mycobacterium tuberculosis LprA is a lipoprotein agonist of TLR2
that regulates innate immunity and APC function. J Immunol
177:422, 2006
45. Gehring AJ, Dobos KM, Belisle JT, Harding CV, Boom WH: Mycobacterium tuberculosis LprG (Rv1411c): A novel TLR-2 ligand
that inhibits human macrophage class II MHC antigen processing.
J Immunol 173:2660, 2004
46. Quesniaux VJ, Nicolle DM, Torres D, Kremer L, Guerardel Y,
Nigou J, Puzo G, Erard F, Ryffel B: Toll-like receptor 2 (TLR2)dependent-positive and TLR2-independent-negative regulation of
proinflammatory cytokines by mycobacterial lipomannans. J Immunol 172:4425, 2004
47. Gilleron M, Himoudi N, Adam O, Constant P, Venisse A, Riviere M, Puzo G: Mycobacterium smegmatis phosphoinositolsglyceroarabinomannans. Structure and localization of alkalilabile and alkali-stable phosphoinositides. J Biol Chem 272:117,
1997
48. Jones BW, Means TK, Heldwein KA, Keen MA, Hill PJ, Belisle
JT, Fenton MJ: Different Toll-like receptor agonists induce distinct
macrophage responses. J Leukoc Biol 69:1036, 2001
49. Abel B, Thieblemont N, Quesniaux VJ, Brown N, Mpagi J, Miyake
K, Bihl F, Ryffel B: Toll-like receptor 4 expression is required to
control chronic Mycobacterium tuberculosis infection in mice. J
Immunol 169:3155, 2002
Journal of Clinical Immunology, Vol. 27, No. 4, 2007
�HOST INNATE IMMUNE RESPONSE TO
359
m. tuberculosis
50. Gilleron M, Nigou J, Nicolle D, Quesniaux V, Puzo G: The acylation state of mycobacterial lipomannans modulates innate immunity response through toll-like receptor 2. Chem Biol 13:39,
2006
51. Means TK, Lien E, Yoshimura A, Wang S, Golenbock DT, Fenton
MJ: The CD14 ligands lipoarabinomannan and lipopolysaccharide differ in their requirement for Toll-like receptors. J Immunol
163:6748, 1999
52. Kamath AB, Alt J, Debbabi H, Behar SM: Toll-like receptor 4defective C3H/HeJ mice are not more susceptible than other C3H
substrains to infection with Mycobacterium tuberculosis. Infect
Immun 71:4112, 2003
53. Reiling N, Holscher C, Fehrenbach A, Kroger S, Kirschning CJ,
Goyert S, Ehlers S: Cutting edge: Toll-like receptor (TLR)2- and
TLR4-mediated pathogen recognition in resistance to airborne infection with Mycobacterium tuberculosis. J Immunol 169:3480,
2002
54. Sugawara I, Yamada H, Li C, Mizuno S, Takeuchi O, Akira
S: Mycobacterial infection in TLR2 and TLR6 knockout mice.
Microbiol Immunol 47:327, 2003
55. Noss EH, Pai RK, Sellati TJ, Radolf JD, Belisle J, Golenbock DT,
Boom WH, Harding CV: Toll-like receptor 2-dependent inhibition
of macrophage class II MHC expression and antigen processing
by 19-kDa lipoprotein of Mycobacterium tuberculosis. J Immunol
167:910, 2001
56. Fortune SM, Solache A, Jaeger A, Hill PJ, Belisle JT, Bloom
BR, Rubin EJ, Ernst JD: Mycobacterium tuberculosis inhibits
macrophage responses to IFN-gamma through myeloid differentiation factor 88-dependent and -independent mechanisms. J Immunol
172:6272, 2004
57. Banaiee N, Kincaid EZ, Buchwald U, Jacobs WR, Jr, Ernst JD:
Potent inhibition of macrophage responses to IFN-gamma by live
virulent Mycobacterium tuberculosis is independent of mature
mycobacterial lipoproteins but dependent on TLR2. J Immunol
176:3019, 2006
58. Pompei L, Jang S, Zamlynny B, Ravikumar S, McBride A,
Hickman SP, Salgame P: Disparity in interleukin-12 release in
dendritic cells and macrophages in response to Mycobacterium
tuberculosis is due to utilization of distinct Toll-like receptors. J
Immunol, 2007 (in press)
59. Bafica A, Scanga CA, Feng CG, Leifer C, Cheever A, Sher A:
TLR9 regulates Th1 responses and cooperates with TLR2 in mediating optimal resistance to Mycobacterium tuberculosis. J Exp
Med 202:1715, 2005
60. Flynn JL, Chan J: Immunology of tuberculosis. Annu Rev Immunol
19:93, 2001
61. Denis M: Killing of Mycobacterium tuberculosis within human
monocytes: Activation by cytokines and calcitriol. Clin Exp Immunol 84:200, 1991
62. Wilkinson RJ, Llewelyn M, Toossi Z, Patel P, Pasvol G, Lalvani A,
Wright D, Latif M, Davidson RN: Influence of vitamin D deficiency
and vitamin D receptor polymorphisms on tuberculosis among
Gujarati Asians in west London: A case–control study. Lancet
355:618, 2000
63. Liu PT, Stenger S, Li H, Wenzel L, Tan BH, Krutzik SR, Ochoa
MT, Schauber J, Wu K, Meinken C, Kamen DL, Wagner M, Bals
R, Steinmeyer A, Zugel U, Gallo RL, Eisenberg D, Hewison M,
Hollis BW, Adams JS, Bloom BR, Modlin RL: Toll-like receptor
triggering of a vitamin D-mediated human antimicrobial response.
Science 311:1770, 2006
64. Auricchio G, Garg SK, Martino A, Volpe E, Ciaramella A, De
Vito P, Baldini PM, Colizzi V, Fraziano M: Role of macrophage
Journal of Clinical Immunology, Vol. 27, No. 4, 2007
65.
66.
67.
68.
69.
70.
71.
72.
73.
74.
75.
76.
77.
78.
79.
80.
phospholipase D in natural and CpG-induced antimycobacterial
activity. Cell Microbiol 5:913, 2003
Russell DG: Who puts the tubercle in tuberculosis? Nat Rev Microbiol 5:39, 2007
Ulrichs T, Kaufmann SH: New insights into the function of granulomas in human tuberculosis. J Pathol 208:261, 2006
Salgame P: Host innate and Th1 responses and the bacterial factors that control Mycobacterium tuberculosis infection. Curr Opin
Immunol 17:374, 2005
Estaquier J, Idziorek T, Weiping Z, Emilie D, Farber C-M,
Bourez J-M, Ameisen JC: T helper type 1/T helper type 2 cytokines and T cell death: Preventive effect of IL-12 on activationinduced and CD95 (Fas/Apo-1)-mediated apoptosis of CD4+ T
cells from human immunodeficiency virus-infected persons. J Exp
Med 182:1759, 1995
Rosenzweig SD, Holland SM: Defects in the interferon-gamma
and interleukin-12 pathways. Immunol Rev 203:38, 2005
Brombacher F, Kastelein RA, Alber G: Novel IL-12 family members shed light on the orchestration of Th1 responses. Trends Immunol 24:207, 2003
Zhang M, Gong J, Iyer DV, Jones BE, Modlin RL, Barnes PF:
T cell cytokine responses in persons with tuberculosis and human immunodeficiency virus infection. J Clin Invest 94:2435,
1994
Giacomini E, Iona E, Ferroni L, Miettinen M, Fattorini L, Orefici
G, Julkunen I, Coccia EM: Infection of human macrophages and
dendritic cells with Mycobacterium tuberculosis induces a differential cytokine gene expression that mosulates T cell response. J
Immunol 166:7033, 2001
Hickman SP, Chan J, Salgame P: Mycobacterium tuberculosis induces differential cytokine production from dendritic cells and
macrophages with divergent effects on naive T cell polarization. J
Immunol 168:4636, 2002
Verreck FA, de Boer T, Langenberg DM, Hoeve MA, Kramer
M, Vaisberg E, Kastelein R, Kolk A, de Waal-Malefyt R,
Ottenhoff TH: Human IL-23-producing type 1 macrophages promote but IL-10-producing type 2 macrophages subvert immunity
to (myco)bacteria. Proc Natl Acad Sci USA 101:4560, 2004
Flynn J, Goldstein M, Triebold K, Sypek J, Wolf S, Bloom B:
IL-12 increases resistance of BALB/c mice to Mycobacterium tuberculosis infection. J Immunol 155:2515, 1995
Castro A, Silva R, Appelberg R: Endogenously produced IL-12 is
required for the induction of protective T cells during Mycobacterium avium infections in mice. J Immunol 155:2013, 1995
Feng CG, Jankovic D, Kullberg M, Cheever A, Scanga CA, Hieny
S, Caspar P, Yap GS, Sher A: Maintenance of pulmonary Th1
effector function in chronic tuberculosis requires persistent IL-12
production. J Immunol 174:4185, 2005
Khader SA, Pearl JE, Sakamoto K, Gilmartin L, Bell GK, JelleyGibbs DM, Ghilardi N, deSauvage F, Cooper AM: IL-23 Compensates for the Absence of IL-12p70 and is essential for the IL-17
response during tuberculosis but is dispensable for protection and
antigen-specific IFN-{gamma} responses if IL-12p70 is available.
J Immunol 175:788, 2005
Chackerian AA, Chen S-J, Brodie SJ, Mattson JD, McClanahan
TK, Kastelein RA, Bowman EP: Neutralization or absence of the
interleukin-23 pathway does not compromise immunity to mycobacterial infection. Infect Immun 74:6092, 2006
Cooper AM, Kipnis A, Turner J, Magram J, Ferrante J, Orme
IM: Mice lacking bioactive IL-12 can generate protective,
antigen-specific cellular responses to mycobacterial infection only
if the IL-12 p40 subunit is present. J Immunol 168:1322, 2002
�360
81. Happel KI, Lockhart EA, Mason CM, Porretta E, Keoshkerian E,
Odden AR, Nelson S, Ramsay AJ: Pulmonary interleukin-23 gene
delivery increases local T-cell immunity and controls growth of
Mycobacterium tuberculosis in the lungs. Infect Immun 73:5782,
2005
82. Hunter CA: New IL-12-family members: IL-23 and IL-27,
cytokines with divergent functions. Nat Rev Immunol 5:521,
2005
83. Pearl JE, Khader SA, Solache A, Gilmartin L, Ghilardi N, deSauvage F, Cooper AM: IL-27 signaling compromises control
of bacterial growth in mycobacteria-infected mice. J Immunol
173:7490, 2004
84. Artis D, Johnson LM, Joyce K, Saris C, Villarino A, Hunter CA,
Scott P: Cutting edge: Early IL-4 production governs the requirement for IL-27-WSX-1 signaling in the development of protective
Th1 cytokine responses following Leishmania major infection. J
Immunol 172:4672, 2004
85. Villarino A, Hibbert L, Lieberman L, Wilson E, Mak T, Yoshida
H, Kastelein RA, Saris C, Hunter CA: The IL-27R (WSX-1) is required to suppress T cell hyperactivity during infection. Immunity
19:645, 2003
86. Villarino AV, Huang E, Hunter CA: Understanding the proand anti-inflammatory properties of IL-27. J Immunol 173:715,
2004
87. Stenger S: Immunological control of tuberculosis: Role of tumour
necrosis factor and more. Ann Rheum Dis 64(Suppl 4):iv24, 2005
88. Chan J, Xing Y, Magliozzo R, Bloom B: Killing of virulent Mycobacterium tuberculosis by reactive nitrogen intermediates produced by activated murine macrophages. J Exp Med 175:1111,
1992
89. Keane J, Balcewicz-Sablinska MR, Remold HG, Chupp GL, Meek
BB, Fenton MJ, Kornfeld H: Infection by Mycobacterium tuberculosis promotes human alveolar macrophage apoptosis. Infect
Immun 65:298, 1997
90. Winau F, Weber S, Sad S, de Diego J, Hoops SL, Breiden B,
Sandhoff K, Brinkmann V, Kaufmann SHE, Schaible UE: Apoptotic vesicles crossprime CD8 T cells and protect against tuberculosis. Immunity 24:105, 2006
91. Balcewicz-Sablinska MK, Keane J, Kornfeld H, Remold HG:
Pathogenic Mycobacterium tuberculosis evades apoptosis of host
macrophages by release of TNF-R2, resulting in inactivation of
TNF-alpha. J Immunol 161:2636, 1998
92. Engele M, Castiglione K, Schwerdtner N, Wagner M, Bolcskei
P, Rollinghoff M, Stenger S: Induction of TNF in human alveolar macrophages as a potential evasion mechanism of virulent
Mycobacterium tuberculosis. J Immunol 168:1328, 2002
93. Kindler V, Sappino A-P, Grau GE, Piguet P-F, Vassalli P: The
inducing role of tumor necrosis factor in the development of bactericidal granulomas during BCG infection. Cell 56:731, 1989
94. Flynn JL, Goldstein MM, Chan J, Triebold KJ, Pfeffer K,
Loenstein CL, Schreiber R, Mak TW, Bloom BR: Tumor necrosis factor is required in the protective immune response against
Mycobacterium tuberculosis in mice. Immunity 2:561, 1995
95. Roach DR, Bean AGD, Demangel C, France MP, Briscoe H,
Britton WJ: TNF regulates chemokine induction essential for cell
recruitment, granuloma formation, and clearance of mycobacterial
infection. J Immunol 168:4620, 2002
96. Algood HMS, Chan J, Flynn JL: Chemokines and tuberculosis.
Cytokine Growth Factor Rev 14:467, 2003
97. Algood HMS, Lin PL, Flynn JL: Tumor necrosis factor and
chemokine interactions in the formation and maintenance of granulomas in tuberculosis. Clin Infect Dis 41:S189, 2005
BHATT AND SALGAME
98. Tufariello JM, Chan J, Flynn JL: Latent tuberculosis: Mechanisms
of host and bacillus that contribute to persistent infection. Lancet
Infect Dis 3:578, 2003
99. Mohan VP, Scanga CA, Yu K, Scott HM, Tanaka KE, Tsang E, Tsai
MM, Flynn JL, Chan J: Effects of tumor necrosis factor alpha on
host immune response in chronic persistent tuberculosis: Possible
role for limiting pathology. Infect Immun 69:1847, 2001
100. Keane J, Gershon S, Wise RP, Mirabile-Levens E, Kasznica J,
Schwieterman WD, Siegel JN, Braun MM: Tuberculosis associated with infliximab, a tumor necrosis factor {alpha}-neutralizing
agent. N Engl J Med 345:1098, 2001
101. Gardam MA, Keystone EC, Menzies R, Manners S, Skamene E,
Long R, Vinh DC: Anti-tumour necrosis factor agents and tuberculosis risk: Mechanisms of action and clinical management. Lancet
Infect Dis 3:148, 2003
102. Peters W, Ernst JD: Mechanisms of cell recruitment in the immune
response to Mycobacterium tuberculosis. Microbes Infect 5:151,
2003
103. Orlova MO, Majorov KB, Lyadova IV, Eruslanov EB, M’lan CE,
Greenwood CMT, Schurr E, Apt AS: Constitutive differences in
gene expression profiles parallel genetic patterns of susceptibility
to tuberculosis in mice. Infect Immun 74:3668, 2006
104. Tessier P, Naccache P, Clark-Lewis I, Gladue R, Neote K, McColl
S: Chemokine networks in vivo: Involvement of C-X-C and CC chemokines in neutrophil extravasation in vivo in response to
TNF-alpha. J Immunol 159:3595, 1997
105. Lande R, Giacomini E, Grassi T, Remoli ME, Iona E, Miettinen M,
Julkunen I, Coccia EM: IFN-alpha beta released by Mycobacterium
tuberculosis-infected human dendritic cells induces the expression
of CXCL10: Selective recruitment of NK and activated T cells. J
Immunol 170:1174, 2003
106. Peters W, Scott HM, Chambers HF, Flynn JL, Charo IF, Ernst
JD: Chemokine receptor 2 serves an early and essential role in
resistance to Mycobacterium tuberculosis. Proc Natl Acad Sci USA
98:7958, 2001
107. Scott HM, Flynn JL: Mycobacterium tuberculosis in chemokine
receptor 2-deficient mice: Influence of dose on disease progression.
Infect Immun 70:5946, 2002
108. Peters W, Cyster JG, Mack M, Schlondorff D, Wolf AJ, Ernst JD,
Charo IF: CCR2-dependent trafficking of F4/80dim macrophages
and CD11cdim/intermediate dendritic cells is crucial for T cell
recruitment to lungs infected with Mycobacterium tuberculosis. J
Immunol 172:7647, 2004
109. Kipnis A, Basaraba RJ, Orme IM, Cooper AM: Role of chemokine
ligand 2 in the protective response to early murine pulmonary
tuberculosis. Immunology 109:547, 2003
110. Floto RA, MacAry PA, Boname JM, Mien TS, Kampmann B,
Hair JR, Huey OS, Houben ENG, Pieters J, Day C, Oehlmann
W, Singh M, Smith KGC, Lehner PJ: Dendritic cell stimulation by
mycobacterial Hsp70 is mediated through CCR5. Science 314:454,
2006
111. Badewa AP, Quinton LJ, Shellito JE, Mason CM: Chemokine receptor 5 and its ligands in the immune response to murine tuberculosis. Tuberculosis 85:185, 2005
112. Algood HM, Flynn JL: CCR5-deficient mice control Mycobacterium tuberculosis infection despite increased pulmonary lymphocytic infiltration. J Immunol 173:3287, 2004
113. Kahnert A, Hopken UE, Stein M, Bandermann S, Lipp M,
Kaufmann SHE: Mycobacterium tuberculosis triggers formation
of lymphoid structure in murine lungs. J Infect Dis 195:46, 2007
114. Seiler P, Aichele P, Bandermann S, Hauser AE, Lu B, Gerard
NP, Gerard C, Ehlers S, Mollenkopf HJ, Kaufmann SH: Early
Journal of Clinical Immunology, Vol. 27, No. 4, 2007
�HOST INNATE IMMUNE RESPONSE TO
115.
116.
117.
118.
119.
120.
121.
122.
123.
124.
125.
126.
127.
128.
361
m. tuberculosis
granuloma formation after aerosol Mycobacterium tuberculosis infection is regulated by neutrophils via CXCR3-signaling
chemokines. Eur J Immunol 33:2676, 2003
Chakravarty SD, Xu J, Lu B, Gerard C, Flynn J, Chan J: The
chemokine receptor CXCR3 attenuates the control of chronic Mycobacterium tuberculosis infection in BALB/c mice. J Immunol
178:1723, 2007
Bromley SK, Peterson DA, Gunn MD, Dustin ML: Cutting edge:
Hierarchy of chemokine receptor and TCR signals regulating T
cell migration and proliferation. J Immunol 165:15, 2000
Jang S, Uematsu S, Akira S, Salgame P: IL-6 and IL-10 induction
from dendritic cells in response to Mycobacterium tuberculosis is
predominantly dependent on TLR2-mediated recognition. J Immunol 173:3392, 2004
Boussiotis VA, Tsai EY, Yunis EJ, Thim S, Delgado JC, Dascher
CC, Berezovskaya A, Rousset D, Reynes JM, Goldfeld AE: IL10-producing T cells suppress immune responses in anergic tuberculosis patients. J Clin Invest 105:1317, 2000
Gerosa F, Nisii C, Righetti S, Micciolo R, Marchesini M, Cazzadori
A, Trinchieri G: CD4+ T cell clones producing both interferongamma and interleukin-10 predominate in bronchoalveolar lavages
of active pulmonary tuberculosis patients. Clin Immunol 92:224,
1999
Hirsch CS, Toossi Z, Othieno C, Johnson JL, Schwander SK,
Robertson S, Wallis RS, Edmonds K, Okwera A, Mugerwa R,
Peters P, Ellner JJ: Depressed T-cell interferon-gamma responses
in pulmonary tuberculosis: Analysis of underlying mechanisms
and modulation with therapy. J Infect Dis 180:2069, 1999
Barnes PF, Lu S, Abrams JS, Wang E, Yamamura M, Modlin RL:
Cytokine production at the site of disease in human tuberculosis.
Infect Immun 61:3482, 1993
Fulton SA, Cross JV, Toossi ZT, Boom WH: Regulation of
interleukin-12 by interleukin-10, transforming growth factor-beta,
tumor necrosis factor-alpha, and interferon-gamma in human
monocytes infected with Mycobacterium tuberculosis H37Ra. J
Infect Dis 178:1105, 1998
De La Barrera S, Aleman M, Musella R, Schierloh P, Pasquenelli
V, Garcia V, Abbate E, Sasiain M, Del C: IL-10 down-regulates
costimulatory molecules on Mycobacterium tuberculosis-pulsed
macrophages and impairs the lytic activity of CD4 and CD8
CTL in tuberculosis patients. Clin Exp Immunol 138:128,
2004
Rojas RE, Balaji KN, Subramanian A, Boom WH: Regulation
of human CD4+ alpha beta T-cell-receptor-positive (TCR+ ) and
gamma delta TCR+ T-cell responses to Mycobacterium tuberculosis by interleukin-10 and transforming growth factor beta. Infect
Immun 67:6461, 1999
North RJ: Mice incapable of making IL-4 or IL-10 display normal
resistance to infection with Mycobacterium tuberculosis. Clin Exp
Immunol 113:55, 1998
Turner J, Gonzalez-Juarrero M, Ellis DL, Basaraba RJ, Kipnis A,
Orme IM, Cooper AM: in vivo IL-10 production reactivates chronic
pulmonary tuberculosis in C57BL/6 mice. J Immunol 169:6343,
2002
Feng CG, Kullberg MC, Jankovic D, Cheever AW, Caspar P,
Coffman RL, Sher A: Transgenic mice expressing human
interleukin-10 in the antigen-presenting cell compartment show
increased susceptibility to infection with Mycobacterium avium
associated with decreased macrophage effector function and apoptosis. Infect Immun 70:6672, 2002
Awomoyi AA, Marchant A, Howson JM, McAdam KP, Blackwell JM, Newport MJ: Interleukin-10, polymorphism in SLC11A1
Journal of Clinical Immunology, Vol. 27, No. 4, 2007
129.
130.
131.
132.
133.
134.
135.
136.
137.
138.
139.
140.
141.
142.
143.
144.
(formerly NRAMP1), and susceptibility to tuberculosis. J Infect
Dis 186:1808, 2002
Buettner M, Meinken C, Bastian M, Bhat R, Stossel E, Faller
G, Cianciolo G, Ficker J, Wagner M, Rollinghoff M, Stenger S:
Inverse correlation of maturity and antibacterial activity in human
dendritic cells. J Immunol 174:4203, 2005
Bhatt K, Hickman SP, Salgame P: Cutting edge: A new approach to
modeling early lung immunity in murine tuberculosis. J Immunol
172:2748, 2004
Humphreys IR, Stewart GR, Turner DJ, Patel J, Karamanou D,
Snelgrove RJ, Young DB: A role for dendritic cells in the dissemination of mycobacterial infection. Microbes Infect 8:1339, 2006
Jiao X, Lo-Man R, Guermonprez P, Fiette L, Deriaud E, Burgaud
S, Gicquel B, Winter N, Leclerc C: Dendritic cells are host cells
for mycobacteria in vivo that trigger innate and acquired immunity.
J Immunol 168:1294, 2002
Tian T, Woodworth J, Skold M, Behar SM: in vivo depletion of
CD11c+ cells delays the CD4+ T cell response to Mycobacterium
tuberculosis and exacerbates the outcome of infection. J Immunol
175:3268, 2005
Abadie V, Badell E, Douillard P, Ensergueix D, Leenen PJ, Tanguy
M, Fiette L, Saeland S, Gicquel B, Winter N: Neutrophils rapidly
migrate via lymphatics after Mycobacterium bovis BCG intradermal vaccination and shuttle live bacilli to the draining lymph nodes.
Blood 106:1843, 2005
Pedrosa J, Saunders BM, Appelberg R, Orme IM, Silva MT, Cooper
AM: Neutrophils play a protective nonphagocytic role in systemic Mycobacterium tuberculosis infection of mice. Infect Immun
68:577, 2000
Tsai MC, Chakravarty S, Zhu G, Xu J, Tanaka K, Koch C,
Tufariello J, Flynn J, Chan J: Characterization of the tuberculous
granuloma in murine and human lungs: Cellular composition and
relative tissue oxygen tension. Cell Microbiol 8:218, 2006
Schaible UE, Winau F, Sieling PA, Fischer K, Collins HL, Hagens
K, Modlin RL, Brinkmann V, Kaufmann SH: Apoptosis facilitates
antigen presentation to T lymphocytes through MHC-I and CD1
in tuberculosis. Nat Med 9:1039, 2003
Makino M, Maeda Y, Mukai T, Kaufmann SH: Impaired maturation
and function of dendritic cells by mycobacteria through IL-1beta.
Eur J Immunol 36:1443, 2006
Hanekom WA, Mendillo M, Manca C, Haslett PA, Siddiqui MR,
Barry C, III, Kaplan G: Mycobacterium tuberculosis inhibits maturation of human monocyte-derived dendritic cells in vitro. J Infect
Dis 188:257, 2003
Khader SA, Partida-Sanchez S, Bell G, Jelley-Gibbs DM, Swain
S, Pearl JE, Ghilardi N, deSauvage FJ, Lund FE, Cooper AM:
Interleukin 12p40 is required for dendritic cell migration and T
cell priming after Mycobacterium tuberculosis infection. J Exp
Med 203:1805, 2006
Demangel C, Bertolino P, Britton WJ: Autocrine IL-10 impairs
dendritic cell (DC)-derived immune responses to mycobacterial infection by suppressing DC trafficking to draining lymph
nodes and local IL-12 production. Eur J Immunol 32:994,
2002
Flynn JL, Chan J: Immune evasion by Mycobacterium tuberculosis:
Living with the enemy. Curr Opin Immunol 15:450, 2003
Dayaram YK, Talaue MT, Connell ND, Venketaraman V: Characterization of a glutathione metabolic mutant of Mycobacterium tuberculosis and its resistance to glutathione and nitrosoglutathione.
J Bacteriol 188:1364, 2006
Thoma-Uszynski S, Stenger S, Takeuchi O, Ochoa MT, Engele M, Sieling PA, Barnes PF, Rollinghoff M, Bolcskei PL,
�362
145.
146.
147.
148.
149.
150.
151.
152.
153.
154.
155.
BHATT AND SALGAME
Wagner M, Akira S, Norgard MV, Belisle JT, Godowski PJ, Bloom
BR, Modlin RL: Induction of direct antimicrobial activity through
mammalian Toll-like receptors. Science 291:1544, 2001
Nozaki Y, Hasegawa Y, Ichiyama S, Nakashima I, Shimokata
K: Mechanism of nitric oxide-dependent killing of Mycobacterium bovis BCG in human alveolar macrophages. Infect Immun
65:3644, 1997
MacMicking JD, Taylor GA, McKinney JD: Immune control of
tuberculosis by IFN-gamma-inducible LRG-47. Science 302:654,
2003
Deretic V: Autophagy as an immune defense mechanism. Curr
Opin Immunol 18:375, 2006
Gutierrez MG, Master SS, Singh SB, Taylor GA, Colombo MI,
Deretic V: Autophagy is a defense mechanism inhibiting BCG
and Mycobacterium tuberculosis survival in infected macrophages.
Cell 119:753, 2004
Ferrero E, Biswas P, Vettoretto K, Ferrarini M, Uguccioni M, Piali
L, Leone BE, Moser B, Rugarli C, Pardi R: Macrophages exposed
to Mycobacterium tuberculosis release chemokines able to recruit
selected leucocyte subpopulations: Focus on γ δ cells. Immunology
108:365, 2003
Lockhart E, Green AM, Flynn JL: IL-17 production is dominated by {gamma}{delta} T cells rather than CD4 T cells during Mycobacterium tuberculosis infection. J Immunol 177:4662,
2006
Mogues T, Goodrich ME, Ryan L, LaCourse R, North RJ: The relative importance of T cell subsets in immunity and immunopathology of airborne Mycobacterium tuberculosis infection in mice. J
Exp Med 193:271, 2001
Saunders BM, Frank AA, Cooper AM, Orme IM: Role of
gamma delta T cells in immunopathology of pulmonary Mycobacterium avium infection in mice. Infect Immun 66:5508,
1998
Munk M, Gatrill A, Kaufmann S: Target cell lysis and IL-2 secretion by gamma/delta T lymphocytes after activation with bacteria.
J Immunol 145:2434, 1990
Chen ZW: Immune regulation of [gamma][delta] T cell responses
in mycobacterial infections. Clin Immunol 116:202, 2005
Shen Y, Zhou D, Qiu L, Lai X, Simon M, Shen L, Kou Z, Wang
Q, Jiang L, Estep J, Hunt R, Clagett M, Sehgal PK, Li Y, Zeng X,
Morita CT, Brenner MB, Letvin NL, Chen ZW: Adaptive immune
response of Vgamma 2Vdelta 2+ T cells during mycobacterial
infections. Science 295:2255, 2002
156. Li B, Rossman M, Imir T, Oner-Eyuboglu A, Lee C, Biancaniello
R, Carding S: Disease-specific changes in gamma delta T cell
repertoire and function in patients with pulmonary tuberculosis. J
Immunol 157:4222, 1996
157. Vankayalapati R, Garg A, Porgador A, Griffith DE, Klucar P, Safi
H, Girard WM, Cosman D, Spies T, Barnes PF: Role of NK cellactivating receptors and their ligands in the lysis of mononuclear
phagocytes infected with an intracellular bacterium. J Immunol
175:4611, 2005
158. Junqueira-Kipnis AP, Kipnis A, Jamieson A, Juarrero MG,
Diefenbach A, Raulet DH, Turner J, Orme IM: NK cells respond
to pulmonary infection with Mycobacterium tuberculosis, but play
a minimal role in protection. J Immunol 171:6039, 2003
159. Feng CG, Kaviratne M, Rothfuchs AG, Cheever A, Hieny S, Young
HA, Wynn TA, Sher A: NK cell-derived IFN-{gamma} differentially regulates innate resistance and neutrophil response in T
cell-deficient hosts infected with Mycobacterium tuberculosis. J
Immunol 177:7086, 2006
160. Gansert JL, Kiebler V, Engele M, Wittke F, Rollinghoff M, Krensky
AM, Porcelli SA, Modlin RL, Stenger S: Human NKT cells express granulysin and exhibit antimycobacterial activity. J Immunol
170:3154, 2003
161. Apostolou I, Takahama Y, Belmant C, Kawano T, Huerre M,
Marchal G, Cui J, Taniguchi M, Nakauchi H, Fournie J-J, Kourilsky P, Gachelin G: Murine natural killer cells contribute to the
granulomatous reaction caused by mycobacterial cell walls. PNAS
96:5141, 1999
162. Chackerian A, Alt J, Perera V, Behar SM: Activation of NKT cells
protects mice from tuberculosis. Infect Immun 70:6302, 2002
163. Aliberti J, Bafica A: Anti-inflammatory pathways as a host evasion mechanism for pathogens. Prostaglandins Leukot Essent Fatty
Acids 73:283, 2005
164. Reed MB, Domenech P, Manca C, Su H, Barczak AK, Kreiswirth
BN, Kaplan G, Barry CE, III: A glycolipid of hypervirulent tuberculosis strains that inhibits the innate immune response. Nature
431:84, 2004
165. Ribeiro-Rodrigues R, Resende Co T, Rojas R, Toossi Z, Dietze R,
Boom WH, Maciel E, Hirsch CS: A role for CD4+ CD25+ T cells
in regulation of the immune response during human tuberculosis.
Clin Exp Immunol 144:25, 2006
166. Guyot-Revol V, Innes JA, Hackforth S, Hinks T, Lalvani A: Regulatory T cells are expanded in blood and disease sites in patients
with tuberculosis. Am J Respir Crit Care Med 173:803, 2006
Journal of Clinical Immunology, Vol. 27, No. 4, 2007
�
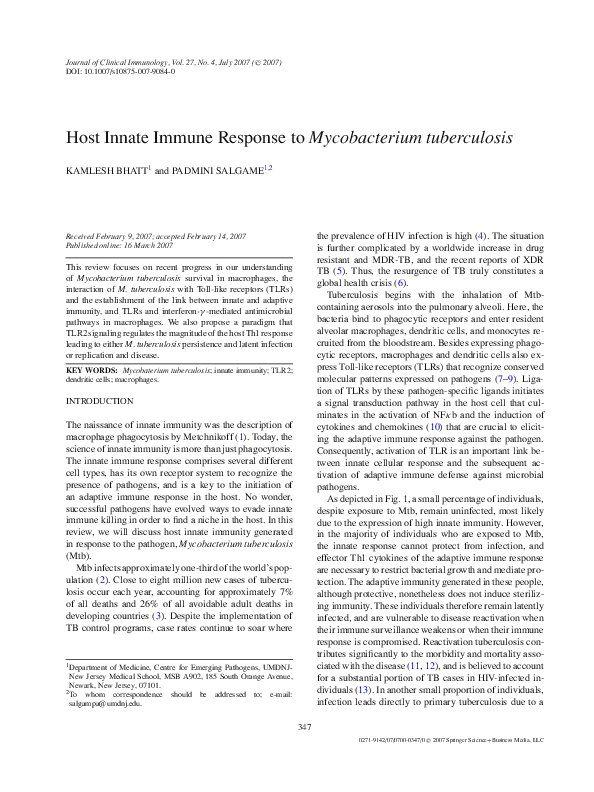
 Kamlesh Bhatt
Kamlesh Bhatt